


Department of Dermatology, Venereology and Allergology, Wroclaw Medical University, Poland. *E-mail: jacek.szepietowski@umed.wroc.pl
Accepted Sep 8, 2021; Epub ahead of print Sep 13, 2021
Acta Derm Venereol 2021; 101: adv00552.
doi: 10.2340/00015555-3921
Pityriasis lichenoides (PL) is an uncommon cutaneous disorder of unclear origin (1). Studies suggest that PL is a benign lymphoproliferative disease, initiated by antigenic triggers, especially viruses (2). There are 3 forms of PL: pityriasis lichenoides chronica (PLC); pityriasis lichenoides et varioliformis acuta (PLEVA); and severe febrile Mucha Habermann’s disease, which is considered a subtype of PLEVA (1). PL predominantly affects young adults and children. The greatest risk of manifesting PL extends into the third decade of life (1, 3).
Gardasil 9® is a nonavalent vaccine against HPV (HPV 6, 11, 16, 18, 31, 33, 45, 52, 58). Injection site reactions, such as pain, erythema, swelling, injection site warmth, pruritus, induration, nodule and urticaria, are the main side-effects. Systemic adverse effects are rare, and include seizure, hyperhidrosis and chills (4). To the best of our knowledge PLEVA following vaccination with the nonevalent HPV vaccine Gardasil 9®, has not been reported previously.
A 33-year-old woman was referred to the dermatology department for diagnosis and treatment of papular non-itchy skin lesions, which appeared for the first time approximately 2 weeks prior to admission. The appearance of the lesions, according to the patient, was associated with vaccination with Gardasil 9® against HPV. The patient’s past medical and family history was unremarkable; she was taking no medications or illicit drugs and her previous vaccinations were uneventful. The patient was vaccinated because of a detected active HPV infection, as suggested by the patient’s gynaecologist. The patient denied any newly introduced drug that could have been given either simultaneously or prior to vaccination. Lesions appeared 3 days after vaccination, initially on the thighs and buttocks. The eruption was characterized by recurrent flares of inflammatory papules without complete regression. The patient reported no fever or any other general symptoms indicating infection. Initial treatment with antihistamine preparations and topical corticosteroids was not effective.
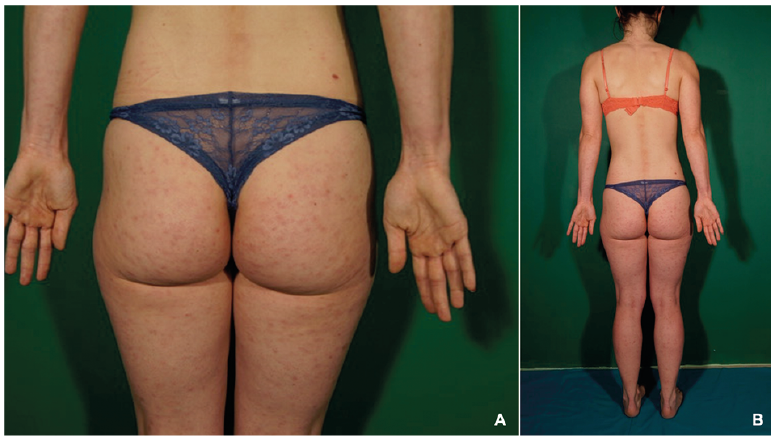
On admission, physical examination revealed disseminated inflammatory papular lesions on the trunk, buttocks and volar forearms, and the entire surface of the lower limbs, abdomen and lower back. The patient’s face was not affected (Fig. 1).
Fig. 1. Disseminated inflammatory papular lesions on the buttocks and volar forearms, on the entire surface of the lower limbs and a few lesions located on the lower back, which appeared 3 days after the first dose of human papillomavirus (HPV) vaccine.
Serologies for HIV, HBV, HCV, Cytomegalovirus, Epstein-Barr virus, parvovirus B19, Chlamydia pneumoniae, Mycoplasma pneumoniae, Borrelia burgdorferi, Toxoplasma gondii and Treponema pallidum were negative.
Complementary examination revealed a slightly elevated bilirubin concentration. No abnormalities were detected on ultrasound examination of the abdomen. Microscopic examination of a punch skin biopsy of a recent lesion showed perivascular lymphocytic infiltration with foci of keratinocyte necrosis and erythrocytes extravasation (Fig. 2).
Fig. 2. Microscopic examination of a punch skin biopsy showed acanthosis, basal cell vacuolar degeneration and spongiosis with foci of keratinocyte necrosis in the epidermis. In the dermis, perivascular lymphocytic infiltration with exocytosis of lymphocytes into the epidermis was observed. Numerous extravasated red blood cells were observed. (Haematoxylin and eosin A: ×100; B: ×400).
Immunohistochemical staining revealed that infiltrated lymphocytes consisted of mainly CD3-positive T cells. The increased number of CD8-positive T cells and foci of B lymphocytes were also observed. CD30 expression was absent.
A diagnosis of PLEVA was made based on the clinical features and histopathological data. The patient was given a course of oral azithromycin, 250 mg daily for 7 days, and mild corticosteroid ointment was applied for 1 month. Subsequently, it was decided to continue therapy with 5 cycles of azithromycin (1 dose of 250 mg every week) and to apply narrow-band ultraviolet-B phototherapy thrice-weekly due to the persistence of cutaneous lesions. New lesions stopped appearing within 2–3 weeks of therapy and the eruption improved partially and at 3-month follow-up. To date, the patient has declined the scheduled booster vaccination.
The underlying pathomechanism of PL remains unclear. One of the principal hypotheses for the aetiology of PL is an inflammatory reaction in genetically vulnerable individuals to an infectious agent, particularly viruses (1). Furthermore, an association between prior viral vaccinations and PL has been reported (3, 5–12). An inflammatory reaction due to T-cell dyscrasia and an immune complex-mediated vasculitis have also been implicated as pathomechanisms of PL (1). The differential diagnosis of PLEVA is broad and includes pityriasis rosea, varicella, Gianotti-Crosti syndrome, psoriasis and secondary syphilis (1).
Gardasil 9® is a nonavalent vaccine against HPV, which contains virus-like particles that elicit strong immune response (13). To the best of our knowledge, only a few cases of skin eruption following HPV vaccination have been reported to date, and all of them were associated with quadrivalent HPV vaccine. Katoulis et al. (14) described the case of 19-year-old woman who developed erythema multiforme 10 days after the injection of the second dose of Gardasil® HPV vaccine. Lesions were located on the patient’s hands and feet. There was no evidence of mucous membrane involvement. Pinheiro et al. (15) reported cutaneous pseudolymphoma associated with HPV immunization in 28-year-old female. The lesion was located in the area of previous intramuscular injections of Gardasil® vaccines. Ojamini et al. (16) described 2 cases of females who developed lipoatrophy at the site of quadrivalent HPV recombinant vaccine injections.
In reviewing the literature, we found 9 cases of PL following immunization (Table SI1) (3, 5–12). To date, one vaccination-associated case of PLC, one case of atypical PL and 7 cases of PLEVA have been reported. PL was connected with various vaccines, both inactivated and live-attenuated. The most frequent type of vaccine was measles, mumps and rubella (MMR) vaccine (3 cases). The range of ages of onset were 1.08–37 years, with a nearly 2-fold male predominance. The latency period for the appearance of the lesions fluctuated from 1 to 10 days. Most patients reported itching concomitant with skin lesions. We have been unable to find any reports on PL related to HPV vaccination.
Considering the aetiology of PLEVA in the current patient, HPV immunization seems to be a possible cause. The lack of other known triggers and temporal correlation between the appearance of skin lesions and the injection of HPV vaccine suggest a causative link. Cross-reactivity between protein molecules of Gardasil 9® and shared epitopes on keratinocytes in connection with trauma from vaccination could trigger PL.
In summary, this is the first case report of PLEVA following HPV immunization.
It is emphasized that HPV vaccination makes a substantial contribution to preventing cervical cancer, and the association of PL with vaccination is an extremely rare event. Nevertheless, dermatologists should be aware of this potential benign side-effect of the vaccine.


 Click to show fullsize
Click to show fullsize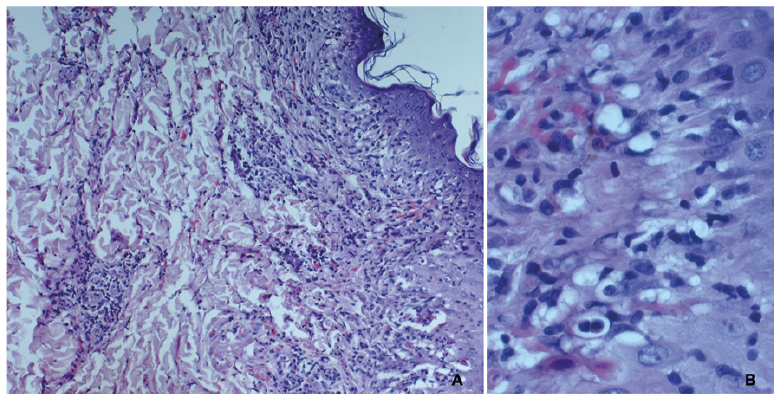 Click to show fullsize
Click to show fullsize