OBJECTIVE: To identify the determinants of improvement in walking capacity following therapeutic exercise in chronic stroke survivors.
DESIGN: A secondary analysis of data obtained from a prospective, single-blind, randomized controlled intervention trial.
SUBJECTS: Sixty-three community-dwelling individuals (mean age = 65 years, age range = 50–87 years) with a chronic stroke (post-stroke duration: mean = 5.5 years, range = 1–28 years).
METHODS: Subjects were randomized into a leg exercise group (n = 32) or an arm exercise group (n = 31). Subjects in each group underwent 3 1-hour exercise sessions per week for 19 weeks. Walking capacity, cardiorespiratory fitness, isometric knee extensor muscle strength, balance ability, and balance confidence were evaluated before and after the interventions. Multiple regression analysis was performed to identify the determinants of improvement in walking capacity.
RESULTS: After controlling for age, gender, post-stroke duration, and baseline walking capacity, gain in paretic leg muscle strength and peak oxygen consumption remained independently associated with gain in walking capacity (R2 = 0.229).
CONCLUSION: Enhancement of cardiorespiratory fitness and paretic leg muscle strength are both significant determinants in improving walking capacity among chronic stroke survivors. However, the rather weak relationship (R2 = 0.229) indicates that other factors not measured in this study may also contribute to the improvement in walking capacity.
Key words: cerebrovascular accident, health promotion, physical fitness, rehabilitation, walking.
J Rehabil Med 2008; 40: 284–290
Correspondence address: Marco Y. C. Pang, Department of Rehabilitation Sciences, Hong Kong Polytechnic University, Hong Kong. E-mail: rsmpang@inet.polyu.edu.hk
Submitted June 25, 2007; accepted November 14, 2007
INTRODUCTION
Walking ability is often impaired following stroke (1). Reduced physical activity level after stroke is common and may induce further deconditioning and decline in walking capacity, as measured by the 6-Minute Walk Test (6MWT) (2). Indeed, walking capacity remains limited for many community-dwelling stroke survivors (3). This may have important health implications for older people with chronic stroke. Poor performance in long-distance walking is associated with mortality and incident cardiovascular disease in older adults (4). Individuals who survive a stroke also have a higher risk of dying from cardiovascular disease than from any other cause (5).
In previous cross-sectional studies, walking capacity following stroke has been related to various physical factors, such as motor recovery (6–8), balance ability (6, 7, 9), spasticity (6), leg muscle strength (6, 9–11) and cardiorespiratory fitness (8, 9, 12). In addition to physical parameters, psychological measure such as balance confidence (i.e. level of confidence that a person has in performing mobility tasks without losing balance or becoming unsteady) may also influence walking capacity among individuals with chronic stroke (13). However, these studies are cross-sectional in nature and could not reflect the temporal relationships between changes in walking capacity and other relevant parameters. Only one study by Pohl et al. (14) has examined the relationship between recovery in walking capacity and other stroke-related impairments in patients after subacute stroke using a prospective design. They found that different factors (i.e. cardiorespiratory fitness, lower limb motor recovery, balance ability) account for the gain in walking capacity at 3-month follow-up, depending upon the initial 6MWT distance (14). In summary, it is apparent that walking capacity in stroke survivors has multiple determinants.
A recent meta-analysis found that gait-oriented training, but not lower limb strengthening training, can significantly improve walking capacity after stroke (15). Different exercise programs have been devised to improve walking capacity after stroke by targeting specific impairments that are related to walking capacity (i.e. balance, leg muscle strength, cardiorespiratory fitness) (15). A study on gait-related training post-stroke has also found that improvement in walking capacity is significantly related to change in balance confidence (16). Evidence is, however, limited for a positive effect of cardiorespiratory exercise training on walking capacity, mainly due to the limited number of randomized controlled trials in this area (15). Overall, the mechanisms underlying improvement in walking capacity following different types of exercise training in stroke are not entirely clear.
We have previously reported that a 19-week multi-dimensional group exercise program, with elements of cardiovascular training, balance exercises, and leg muscle strengthening, significantly improves walking capacity in individuals with chronic stroke (17). However, the determinants of improvement in walking capacity following the exercise training have not been investigated. Moreover, the effect of the program on balance confidence, a psychological factor that may exert important influence on walking capacity (16), has not been reported.
This secondary analysis attempted to identify the physical and psychological factors contributing to improvement in walking capacity following the 19-week multi-dimensional exercise program (17). We hypothesized that changes in walking capacity would be related to changes in cardiorespiratory fitness, leg muscle strength, balance ability, and balance confidence. This hypothesis was proposed because previous cross-sectional studies demonstrated strong associations of walking capacity with these measures (6–12). Our exercise program also contained different components that were designed specifically to target these same impairments.
METHODS
Subjects
Subjects were recruited from a local rehabilitation hospital database, community stroke clubs and local newspaper advertisements. Inclusion criteria were: a single episode of stroke more than one year ago, aged 50 years or more, ability to walk more than 10 meters independently (with or without walking aids), living at home, (a Mini Mental State Examination (MMSE) score > 22 (18), the ability to pedal the cycle ergometer (Excalibur, Lode BV Medical Technology, Groningen, Netherlands) at 60 rpm and increase the heart rate to at least 60% of the maximal heart rate (estimated as 220–age) (19). Exclusion criteria were: neurological conditions in addition to stroke, history of serious cardiac disease, uncontrolled hypertension (systolic blood pressure > 140 mmHg, diastolic blood pressure > 90 mmHg), pain while walking, and other serious diseases that preclude the individual from participating in the study. All subjects provided informed written consent before they participated in the study. The study was approved by the University of British Columbia and G. F. Strong Rehabilitation Centre research ethics committees. The study was conducted in accordance with the Helsinki Declaration for human experiments.
Each subject was classified according to the functional classification level of the American Heart Association Stroke Outcome Classification, to indicate the residual disability in basic (e.g. dressing, bathing, grooming) and instrumental activities of daily living (e.g. shopping, preparing meals) (BADL and IADL) (level I = as independent as before the stroke; level V = completely dependent in BADL and IADL) (20).
Study design
This was a secondary analysis of data obtained from a prospective, single-blind, randomized controlled trial (17). The subjects were stratified according to gender and then randomly assigned to the leg exercise or arm exercise group by drawing lots. The randomization was done before any outcome assessments and interventions.
Interventions
Individuals in each group underwent their respective programs for 19 weeks (1-hour sessions, 3 sessions per week). For both groups, each exercise session (9–12 participants) was supervised by a physiotherapist, an occupational therapist and an exercise instructor.
The details of the intervention programs were described elsewhere (17). Briefly, in the leg exercise group, subjects rotated through 3 different exercise stations. In the first station, participants were engaged in aerobic exercises such as brisk walking, repeated sit-to-stand, and alternate stepping onto low risers. Exercise intensity was initially set at 40–50% heart rate reserve (HRR) and increased by 10% HRR every 4 weeks, up to 70–80% HRR, as tolerated. At station 2, participants were engaged in various balance exercises, such as walking in different directions, and standing on a balance disc or a tilting board. At station 3, subjects participated in leg muscle strengthening exercises including partial squats and toe rises while holding hand weights.
The arm exercise group completed an upper extremity exercise program in the same setting. Similar to the leg exercise group, subjects rotated through 3 exercise stations. At station 1, subjects performed shoulder muscle strengthening exercises using theraband. At station 2, upper limb weight-bearing exercises (i.e. push-ups on the arm-rests of chair) and muscle strengthening exercises using dumb-bells or cuff weights were performed, in addition to passive or self-assisted range of motion exercises. At station 3, the program consisted of hand muscle strengthening exercises using putty or grippers and functional training (i.e. transferring objects of various shapes and sizes). For participants with less than 20 degrees of active wrist extension, electrical stimulation (Neurotrac Sports, Verity Medical Ltd., Hampshire, UK) to the wrist extensor muscles was also applied.
Outcomes
All outcomes were measured by blinded assessors immediately before the commencement and immediately after the termination of the exercise program.
Physical outcomes. Walking capacity was measured using the 6MWT (21). The subjects were asked to cover as much distance as tolerated within 6 minutes. The total distance walked to the nearest meter was recorded. 6MWT has been shown to be a reliable method to assess walking capacity in individuals after stroke (22).
Cardiorespiratory fitness was indicated by peak oxygen consumption rate (O2 in ml/kg/min) obtained from a maximal exercise test on the Excalibur cycle ergometer. V.02 was continuously measured using a portable metabolic unit (Cosmed K4 b2 system; COSMED Srl; Rome, Italy). The workload started at 10–20 W and increased by 10–20 W/min. Participants were required to pedal at 60 rpm. Peak V.O2 was considered to have been reached if at least 2 out of 3 criteria for maximal effort were fulfilled: (i) a respiratory exchange ratio of ≥ 1.0, (ii) a plateau in V.O2 (< 150 ml/min) with increase in exercise intensity, or (iii) volitional fatigue (i.e. decline in cycling rate < 30 rpm) (19). The V.O2 data were averaged at a rate of every 15 sec. The peak value obtained was considered to be the peak V.O2 (ml/kg/min).
Isometric knee extension strength was measured by using hand-held dynamometry (Nicholas MMT, Lafayette Instruments, Lafayette, IN, USA). The knee was placed in 90° flexion while the subject was sitting upright in a chair with back support. After the thigh was stabilized by the assessor, each subject was instructed to perform a maximal isometric contraction of knee extension. Three trials were performed on each side and force data (Newtons (N)) were averaged. Using hand-held dynamometry to assess isometric knee extension strength has been shown to relate to walking capacity in patients after stroke (23). It can also be easily performed in the daily clinical setting and is a reliable method to assess muscle strength in people with stroke (11).
Balance ability was assessed by Berg Balance Scale (BBS; maximal score = 56) (24). It contains 14 items and the rating of each item is based on an ordinal scale from 0 to 4, with a higher score indicating better balance ability. BBS is a reliable and valid tool to assess balance in people after stroke (24).
Psychological outcome. Balance confidence was evaluated using the Activities-Specific Balance Confidence (ABC) scale (25, 26). The scale consists of 16 functional activities and each participant was required to rate their level of confidence in performing each activity without losing their balance or becoming unsteady (e.g. get in and out of a car, walk on an icy sidewalk). The rating is based on a scale ranging from 0 (no confidence at all) to 100 (completely confident). The score for each item were summed and then averaged to yield the mean ABC score. A higher ABC score indicates a higher level of balance confidence. The ABC scale has good internal consistency (Cronbach’s alpha = 0.94) and test-retest reliability (Intraclass Correlation Coefficient (ICC) = 0.85) among individuals after stroke (27).
Statistical methods
For this secondary analysis, any dropouts (3 out of 63) were excluded from the analysis. Two-way analysis of variance (ANOVA) with repeated measures (mixed design; within-subject factor: time, between-subject factor: group) was first used to assess whether one exercise group had significantly more gain in each variable than the other group (i.e. significant group × time interaction). The alpha was set at 0.05 for this analysis. Paired t-tests were then used to compare the pre-test and post-test scores within each exercise group. The level of significance for this analysis was adjusted to 0.02.
The change score of each outcome variable was computed as post-test score minus the pre-test score. The percent change score was calculated by dividing the change score by the pre-test score. Pearson’s product-moment correlation coefficients were then used to measure the degree of association (1) between the baseline score and the change score for each outcome variable, (2) between the change in walking capacity and that in other outcome variables. The alpha level for these analyses was set at 0.05.
To avoid possible multi-colinearity, Pearson’s product moment correlation coefficients were used to determine the degree of association among the change scores for peak V.O2, paretic leg muscle strength, BBS, and ABC. A multiple regression analysis was performed to predict change in walking capacity. Age, gender, post-stroke duration and baseline walking capacity were first forced into the regression model. Next, changes in peak V.O2, paretic leg muscle strength, BBS score, and ABC score were then entered into the model using the forward stepwise method, as no significant correlation was found among the change scores. Variables were entered in the stepwise model at a significance level of p ≤ 0.05 and removed from it at p ≥ 0.10. All statistical analyses were performed using SPSS 14.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Subject characteristics
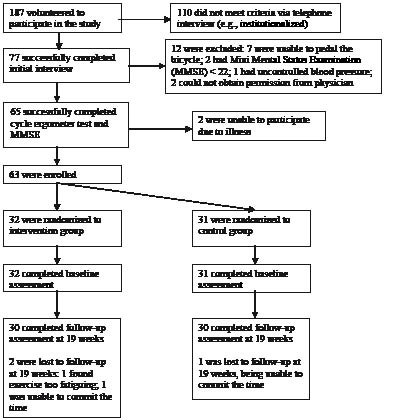
Sixty-three individuals fulfilled all eligibility criteria and participated in the study (Fig. 1). During the course of the 19-week trial, 3 subjects dropped out of the study (2 in the leg exercise group and one in the arm exercise group) and were excluded from subsequent analyses. Subject characteristics are described in Table I.
Fig. 1. Sixty subjects completed all baseline and follow-up assessments. Reprinted with permission from Blackwell Publishing. J Am Geriatr Soc 2005; 53: 1667–1674 (17).
| Table I. Subject characteristics |
| | Leg exercise group (n = 30) | Arm exercise group (n = 30) | Dropout (n = 3) |
| Demographics |
| Female gender (n) | 13 | 12 | 2 |
| Age (years), mean (SD) | 66.0 (8.7) | 65.0 (8.5) | 61.7 (13.2) |
| Height (cm), mean (SD) | 168.9 (11.4) | 169.6 (9.3) | 165.5 (20.7) |
| Weight (kg), mean (SD) | 76.6 (17.9) | 78.1 (12.0) | 66.2 (30.0) |
| Walking aid (cane/quad cane/crutch/walker) (n/n/n) | 3/1/1/6 | 2/0/2/5 | 0/0/0/0 |
| American Heart Association Stroke Functional Classification (I/II/III/IV/V) (n) | 3/17/9/1/0 | 1/19/8/2/0 | 3/0/0/0/0 |
| Education (years), mean (SD) | 14.4 (3.3) | 14.0 (3.4) | 12.0 (1.0) |
| Stroke characteristics |
| Paretic side (left) (n) | 19 | 21 | 1 |
| Ischemic stroke (n) | 18 | 18 | 1 |
| Post-stroke duration (years), mean (SD) | 5.2 (5.0) | 5.1 (3.6) | 12.1 (11.0) |
| Variables of interest, mean (SD) |
| 6MWT distance (m) | 317.8 (140.4) | 296.6 (118.6) | 498.3 (90.2) |
| Peak V.O2 (ml/kg/min) | 22.3 (5.2) | 21.3 (4.2) | 26.7 (4.9) |
| Paretic leg muscle strength (N) | 177.7 (71.9) | 194.6 (69.9) | 238.5 (74.9) |
| Non-paretic leg muscle strength (N) | 248.0 (87.0) | 268.9 (87.2) | 225.4 (81.8) |
| BBS score (0–56) | 47.2 (6.8) | 47.0 (6.0) | 54 (3.5) |
| ABC score (0–100) | 67.0 (19.6) | 72.3 (18.0) | 85.6 (21.7) |
| 6MWT: Six-Minute Walk Test; peak V.O2: peak oxygen consumption rate; BBS: Berg balance scale; ABC: Activities-specific Balance Confidence; SD: standard deviation. |
Change scores in each exercise group
Two way-ANOVA revealed that the leg group had significantly more gain in walking capacity (F1,58 = 6.49, p = 0.01), peak V.O2, (F1,58 = 7.47, p = 0.01) and paretic leg muscle strength (F1,58 = 6.50, p = 0.01) than the arm group. No significant time × group interaction was found between the 2 groups in non-paretic leg muscle strength, BBS, and ABC scores (p > 0.10). When the data for each exercise group were analyzed separately, both the leg and arm exercise groups showed a significant increase in walking capacity and BBS score during the course of the trial (paired t-tests, p < 0.02) (Table II). Only the leg exercise group showed a significant increase in peak V.O2, paretic leg muscle strength, and non-paretic leg muscle strength. ABC scores showed no significant change in both groups.
| Table II. Change scores in variables of interest given as mean values with standard deviation (SD) within parentheses |
| Variables of interest | Leg exercise group (n = 30) | Arm exercise group (n = 30) |
| Change score | Percent change | Change score | Percent change |
| 6MWT distance (m) | 68.8 (52.4)* | 25.6 (22.6) | 39.6 (34.6)* | 14.3 (10.9) |
| Peak V.O2 (ml/kg/min) | 2.1 (3.2)* | 15.9 (17.3) | 0.3 (3.0) | 4.7 (17.3) |
| Paretic leg muscle strength (N) | 43.3 (55.1)* | 25.9 (35.6) | 10.8 (42.9) | 5.7 (22.0) |
| Non-paretic leg muscle strength (N) | 30.2 (59.5)* | 15.6 (26.5) | 6.6 (52.2) | 4.2 (20.7) |
| BBS score | 2.2 (3.6)* | 5.8 (9.5) | 2.0 (2.9)* | 4.6 (6.6) |
| ABC score | 2.9 (14.4) | 12.7 (37.9) | 0.4 (13.4) | 7.0 (43.3) |
| *p < 0.02 significant change from the baseline value (paired t-test). 6MWT: Six-Minute Walk Test; peak V.O2: peak oxygen consumption rate; BBS: Berg balance scale; ABC: Activities-specific Balance Confidence; N: newton. |
Correlations between baseline scores and change scores
The correlations between baseline score and change scores are shown in Table III. A significant, negative correlation was found between the baseline scores and the change scores for BBS (r = –0.61) and ABC scale (r = –0.60), indicating that those with higher baseline BBS or ABC tend to have smaller gain in these variables after the program. No significant correlation was found between the baseline score and the change score for 6MWT (r = 0.14), peak V.O2 (r = –0.23), paretic leg muscle strength (r = 0.09), and non-paretic leg muscle strength (r = –0.35).
| Table III. Correlations (r) between baseline scores and change scores |
| | All subjects | Leg exercise group | Arm exercise group |
| 6MWT distance | 0.14 | 0.06 | 0.23 |
| Peak V.O2 | –0.23 | –0.19 | –0.15 |
| Paretic leg muscle strength | 0.09 | 0.26 | –0.04 |
| Non-paretic leg muscle strength | –0.35 | –0.29 | –0.38* |
| BBS score | –0.61* | –0.82* | –0.33 |
| ABC score | –0.60* | –0.61* | –0.58* |
| *p < 0.05. 6MWT: Six-Minute Walk Test; peak V.O2: peak oxygen consumption rate; BBS: Berg balance scale; ABC: Activities-specific Balance Confidence. |
The negative correlation between the baseline scores and the changes scores for BBS and ABC was still apparent when the leg and arm exercise groups were analyzed separately.
Correlations between change in walking capacity and that in other variables
There was a significant, positive correlation between change in walking capacity and that in peak V.O2 (r = 0.28, p = 0.03) and paretic leg muscle strength (r = 0.38, p < 0.01). There was a trend for a negative relationship between change in walking capacity and that in BBS score (r = –0.24, p = 0.07). No significant correlation was found between change in walking capacity and change in ABC score (r = 0.19, p = 0.16) and non-paretic leg muscle strength (r = 0.22, p = 0.10).
Multiple regression for predicting change in walking capacity
After controlling for age, gender, post-stroke duration and baseline walking capacity, adding change in paretic leg muscle strength (Table IV, model 2) significantly improved the multiple regression model (F change1,54 = 7.74, p = 0.01). Adding change in peak V.O2 in the final model (Table IV, model 3) also significantly improved the prediction (F change1,53 = 4.19, p = 0.05). The final regression model explained a total of 22.9% of the variance in change in walking capacity, with change in paretic leg muscle strength and peak V.O2 accounting for 11.9% and 6.1%, respectively. Change in BBS score and ABC score were removed from the stepwise model (p > 0.05). The multi-colinearity statistics revealed that the tolerance values were all close to 1.0 (> 0.84). Thus, there were no problems with multi-colinearity in this regression analysis.
| Table IV. Multiple regression analysis for predicting change in walking capacity |
| Independent variable | R2 | R2 change | Regression coefficient B (standard error) | Beta weight (β) | p |
| Model 1 | 0.048 | 0.048 | | | |
| Age | | | –0.019 (0.744) | –0.035 | 0.80 |
| Gender | | | –10.521 (12.370) | –0.113 | 0.40 |
| Post-stroke duration | | | –1.316 (1.498) | –0.122 | 0.38 |
| Baseline 6MWT distance | | | 0.055 (0.048) | 0.154 | 0.25 |
| Model 2 | 0.168 | 0.119 | | | |
| Age | | | –0.241 (0.702) | –0.044 | 0.73 |
| Gender | | | –2.186 (12.54) | –0.023 | 0.86 |
| Post-stroke duration | | | –1.159 (1.415) | –0.108 | 0.42 |
| Baseline 6MWT distance | | | 0.042 (0.045) | 0.117 | 0.36 |
| Change paretic leg muscle strength | | | 0.323 (0.116) | 0.360 | 0.01* |
| Model 3 | 0.229 | 0.061 | | | |
| Age | | | –0.026 (0.690) | –0.005 | 0.97 |
| Gender | | | –9.506 (12.246) | –0.102 | 0.44 |
| Post-stroke duration | | | –0.504 (1.412) | –0.047 | 0.72 |
| Baseline 6MWT distance | | | 0.036 (0.044) | 0.101 | 0.42 |
| Change paretic leg muscle strength | | | 0.286 (0.114) | 0.318 | 0.02* |
| Change peak VO2 | | | 3.836 ( (1.873) | 0.265 | 0.05* |
| *p < 0.05. 6MWT: Six-Minute Walk Test. |
DISCUSSION
This is the first study to report the association between the improvement in walking capacity and that in leg muscle strength and cardiorespiratory fitness among individuals with chronic stroke in a prospective randomized controlled intervention trial. The results of this study have highlighted the importance of addressing leg muscle strength and cardiorespiratory fitness when attempting to enhance walking capacity in the population after chronic stroke.
In our sample of 60 subjects, the mean 6MWT distance achieved is around 40–50% below the reference values (28). This may have tremendous health and functional implications. For example, inability to perform long-distance walk (400 m) or increased performance time to complete the 400-m walk are associated with mortality, incident cardiovascular disease, mobility limitation and disability in community-dwelling older adults (4). Although the relationship between 6MWT and risk of mortality and cardiovascular risk in the chronic stroke population is currently unknown, our results have nevertheless highlighted the pronounced deficits in walking capacity in chronic stroke survivors and the potential health risk that ensues.
Both exercise groups in our study had significant gain in walking capacity, but the leg exercise group (25.6%) improved significantly more than the arm exercise group (14.3%). (Table II). It is difficult to compare with other types of exercise programs due to the different exercise frequency and intensity used. Nevertheless, the gain obtained in this group is comparable to that obtained in a recent study by Macko et al. (29). In their study on treadmill training in patients after chronic stroke, a similar exercise frequency and duration was used (i.e. 3 times per week for 6 months) and a significant 30% increase in walking capacity was reported (29). It is interesting that the arm exercise group also had a substantial gain in walking capacity, which may be due to several factors. First, practice effect may partly contribute to the increase in walking capacity. Secondly, although many of the exercises were performed in sitting, the subjects in the arm exercise group had to walk through 3 exercise stations in each session, thus providing opportunities for them to practice walking. Thirdly, activity to attend the sessions (e.g. walking between the community hall and the parking lot) (3 times a week) may well exceed their usual daily amount of walking, as it is well known that low ambulatory activity is common in stroke survivors (2).
One important finding is that gain in paretic leg muscle strength is independently associated with improvement in walking capacity (Table IV). This finding confirms the results from previous cross-sectional studies showing a positive correlation between leg muscle strength and walking capacity (6, 9–11). However, evidence suggests that improvement in strength from resistance training does not necessarily translate into significant gains in walking capacity (15, 30). Strengthening in a functionally relevant way (task-oriented approach) may be a more appropriate way to promote walking capacity, as training effects may be specific to the task itself. The task-oriented approach has been used to enhance walking capacity in chronic stroke and positive outcomes are reported (31, 32). We used a similar approach in our leg exercise group. For example, stepping onto the low risers is a walking-related task which aims to increase the strength of the knee extensor muscle groups.
Another important finding of this study is that gain in peak V.O2 is a significant determinant of improvement in walking capacity. Our results are in agreement with those obtained by Patterson et al. (9) and Pohl et al. (14). In a cross-sectional correlation study, Patterson et al. (9) found that walking capacity is largely determined by cardiorespiratory fitness (R2 = 0.26) for those who can walk faster (gait velocity > 0.48 m/sec) whereas walking capacity is more influenced by balance ability for slow walkers (gait velocity < 0.48 m/sec). Similarly, Pohl et al. (14) found that for good performers in 6MWT at baseline (distance > 213 m), gain in peak V.O2 is a significant determinant of gain in walking capacity at 3-month follow-up. In contrast, gain in balance is the only significant determinant of gain in walking capacity at 3-month follow-up for poor performers in 6MWT at baseline (distance < 213 m) (14). Using their definitions, a large proportion of our subjects can be considered fast walkers (gait velocity > 0.48 m/sec) (82% of subjects) or good performers in 6MWT at baseline (distance > 213 m) (72% of subjects). And we found that gain in cardiorespiratory fitness is a significant determinant of improvement in walking capacity following the exercise intervention. Taken together, the results have highlighted the important role of enhancing cardiorespiratory fitness while attempting to improve walking capacity in chronic stroke survivors, particularly for those who have mild to moderate gait deficits.
It is surprising that change in BBS score was not significantly related to change in walking capacity, as previous cross-sectional studies have demonstrated a strong correlation between balance function and walking capacity (6, 7, 9). This may be explained by the fact that our subjects have only mild to moderate deficits in walking, whereas balance seems to be a major factor in determining gain in walking capacity among those with more severe gait deficits (9, 14). Another explanation is the ceiling effect of the BBS (33). The subjects in our study have a relatively high level of balance functioning (mean BBS score = 47). It may explain why the gain in balance induced by the 2 exercise programs is only around 2 points (Table II), which is below what is considered to be a clinically meaningful change (i.e. ± 6 points) (33). The ceiling effect of BBS may also explain why the change in BBS score is negatively correlated with the baseline BBS score, indicating that those with higher baseline balance ability tend to have a smaller gain in BBS score.
The 2 exercise programs did not result in significant increase in balance confidence. Some suggested mechanisms for enhancing self-efficacy are: successful completion of a task; observing others successfully complete a task; and receiving positive feedback from others (34). Presumably, the group exercise programs in this study would allow for such experiences. The lack of significant improvement in balance confidence may be due to the relatively high level of balance confidence (mean = 70.5) in our sample (i.e. ceiling effect). We found that a high baseline ABC score is related to a lower subsequent gain in the same after exercise intervention.
This study has several limitations. First, the results are generalizable only to ambulatory individuals with chronic stroke. Secondly, over 70% of the variance in change in walking capacity remains unexplained. The determinants of walking capacity may be multifactorial, and not all of the potential determinants were measured in this study (i.e. practice effect, motivation, perceptual deficits, existing co-morbidities, type of stroke). A larger sample size will be needed to identify other potential determinants with smaller effect size. Thirdly, knee extension strength was measured isometrically. A higher correlation between muscle strength and walking capacity might have been obtained if we had measured dynamic muscle strength (10, 11). Finally, the relationship between gain in walking capacity and other measures may vary according to the specific training regimen and other factors such as the physical setting, and client–therapist ratio. It would be interesting to compare the determinants of increase in walking capacity among different types of exercise programs (i.e. resistive training, aerobic training, agility training). Nevertheless, our results have highlighted the important role of leg muscle strength and cardiorespiratory fitness in walking capacity.
In conclusion, this study shows that improvement in walking capacity can be induced by therapeutic exercise in the chronic stroke population and is independently associated with enhancement of paretic leg muscle strength and cardiorespiratory fitness. Unfortunately, it is common that contemporary rehabilitation programs are not intensive enough to induce a cardiovascular training effect (35). Given the serious potential health and functional implications of poor walking capacity, augmentation of leg muscle strength and cardiorespiratory fitness should be important components of stroke rehabilitation or health promotion programs.
ACKNOWLEDGMENTS
Marco Y. C. Pang was supported by a post-doctoral fellowship from Natural Sciences and Engineering Research Council of Canada. Janice J. Eng was supported by a grant-in-aid from the Heart Stroke Foundation of British Columbia and Yukon and from career scientist awards from Canadian Institute of Health Research and the Michael Smith Foundation for Health Research.
Conflict of interest
No commercial party having a direct financial interest in the results of the research supporting this paper has or will confer a benefit upon the author(s) or upon the organization with which the author(s) is/are associated.
REFERENCES
1. Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Stroke: neurologic and functional recovery. The Copenhagen Study. Phys Med Rehabil Clin N Am 1999; 10: 887–906.
2. Michael KM, Allen JK, Macko RF. Reduced ambulatory activity after stroke: the role of balance, gait and cardiovascular fitness. Arch Phys Med Rehabil 2005; 86: 1552–1556.
3. Mayo NE, Wood-Dauphinee S, Ahmed S, Gordon C, Higgins J, McEwen S, et al. Disablement following stroke. Disabil Rehabil 1999; 21: 258–268.
4. Newman AB, Simonsick EM, Naydeck BL, Boudreau RM, Kritchevsky SB, Nevitt MC et al. Association of long-distance corridor walk performance with mortality, cardiovascular disease, mobility limitation, and disability. JAMA 2006; 295: 2018–2026.
5. Roth EJ. Heart disease in patients with stroke: incidence, impact, and implications for rehabilitation. Part I: classification and prevalence. Arch Phys Med Rehabil 1993; 74: 752–760.
6. Eng JJ, Chu KS, Dawson AS, Kim CM, Hepburn KE. Functional walk tests in individuals with stroke: relation to perceived exertion and myocardial exertion. Stroke 2002; 33: 756–761.
7. Pohl PS, Duncan PW, Perera S, Liu W, Lai SM, Studenski S, et al. Influence of stroke-related impairments on performance in 6-minute walk test. J Rehabil Res Dev 2002; 39: 439–444.
8. Courbon A, Calmels P, Roche F, Ramas J, Fayolle-Minon I. Relationship between maximal exercise capacity and walking capacity in adult hemiplegic stroke patients. Am J Phys Med Rehabil 2006; 85: 436–444.
9. Patterson SL, Forrester LW, Rodgers MM, Ryan AS, Ivey FM, Sorkin JD, et al. Determinants of walking function after stroke: differences by deficit severity. Arch Phys Med Rehabil 2007; 88: 115–119.
10. Flansbjer U-B, Downham D, Lexell J. Knee muscle strength, gait performance, and perceived participation after stroke. Arch Phys Med Rehabil 2006; 87: 974–980.
11. Bohannon RW. Muscle strength and muscle training after stroke. J Rehabil Med 2007; 39:14–20.
12. Kelly JO, Kilbreath SL, Davis GM, Zeman B, Raymond J. Cardiorespiratory fitness and walking ability in subacute stroke patients. Arch Phys Med Rehabil 2003; 84: 1780–1785.
13. Salbach NM, Mayo NE, Robichaud-Ekstrand S, Hanley JA, Richards CL, Wood-Dauphinee S. Balance self-efficacy and its relevance to physical function and perceived health status after stroke. Arch Phys Med Rehabil 2006; 87: 364–370.
14. Pohl PS, Perera S, Duncan PW, Maletsky R, Whitman R, Studenski S. Gains in distance walking in a 3-month follow-up post-stroke: what changes. Neurorehabil Neural Repair 2004; 18: 30–36.
15. van de Port IG, Wood-Dauphinee S, Lindeman E, Kwakkel G. Effects of exercise training programs on walking competency after stroke: a systematic review. Am J Phys Med Rehabil [10.1097/PHM.0b013e31802ee464]. 2007 Feb 12 [cited 2007 April 5]; [about 10 p.] [Epub ahead of print]. Available from: http://www.amjphysmedrehab.com/pt/re/ajpmr/paptoc.htm.
16. Salbach NM, Mayo NE, Robichaud-Ekstrand S, Hanley JA, Richards C, Wood-Dauphinee S. The effect of a task-oriented walking intervention on improving balance self-efficacy poststroke: a randomized controlled trial. J Am Geriatr Soc 2005; 53: 576–582.
17. Pang MYC, Eng JJ, Dawson AS, MacKay HA, Harris JE. A community-based fitness and mobility exercise program for individuals with chronic stroke: a randomized controlled trial. J Am Geriatr Soc 2005; 53: 1667–1674.
18. Folstein MF, Folstein, SE, McHugh PR. Mini-Mental State: a practical method for grading the state of patients for the clinician. J Psychiat Res 1975; 12: 189–198.
19. American College of Sports Medicine. ACSM’s guidelines for exercise testing and prescription. 7th edn. Philadelphia, PA: Lippincott Williams & Wilkins; 2005.
20. Kelly-Hayes M, Robertson JT, Broderick JP, Duncan PW, Hershey LA, Roth EJ, et al. The American Heart Association Stroke Outcome Classification: Executive Summary. Circulation 1998; 97: 2474–2478.
21. American Thoracic Society. ATS Statement: Guidelines for the Six-Minute Walk Test. Am J Respir Crit Care Med 2002; 166: 111–117.
22. Flansbjer U-B, Holmback AM, Downhan D, Patten C, Lexell J. Reliability of gait performance tests in men and women with hemiparesis after stroke. J Rehabil Med 2005; 37: 75–82.
23. Bohannon RW. Selected determinants of ambulatory capacity in patients with hemiplegia. Clin Rehabil 1989; 3: 47–53.
24. Berg K, Wood-Dauphinee S, Williams JB. The balance scale: reliability assessment with elderly residents and patients with acute stroke. Scand J Rehabil Med 1995; 27: 27–36.
25. Powell LE, Myers AM. The Activities-Specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci 1995; 50A: M28–M34
26. Myers AM, Fletcher PC, Myers AH, Sherk W. Discriminative and evaluative properties of the Activities-specific Balance Confidence (ABC) Scale. J Gerontol A Biol Sci Med Sci 1998; 53: M287–M294.
27. Botner EM, Miller WC, Eng JJ. Measurement properties of the Activities-specific Balance Confidence Scale among individuals with stroke. Disabil Rehabil 2005; 27: 156–163.
28. Steffen TM, Hacker TA, Mollinger L. Age- and gender-related test performance in community-dwelling elderly people: Six-Minute Walk Test, Berg Balance Scale, Timed Up & Go test, and gait speeds. Phys Ther 2002; 82: 128–137.
29. Macko RF, Ivey FM, Forrester LW, Hanley D, Sorkin JD, Katzel LI, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: a randomized controlled trial. Stroke 2005; 36: 2206–2211.
30. Ouellette MM, LeBrasseur NK, Bean JF, Phillips E, Stein J, Frontera WR, et al. High-intensity resistance training improves muscle strength, self-reported function, and disability in long-term stroke survivors. Stroke 2004; 35: 1404–1409.
31. Salbach NM, Mayo NE, Wood-Dauphinee SW, Hanley JA, Richards, CL, Cote R. A task-oriented intervention enhances walking distance and speed in the first year post stroke: a randomized controlled trial. Clin Rehabil 2004; 18: 509–519.
32. Dean CM, Richards CL, Malouin F. Task-related circuit training improves performance of locomotor tasks in chronic stroke: a randomized controlled trial. Arch Phys Rehabil 2000; 81: 409–417.
33. Stevenson TJ. Detecting change in patients with stroke using the Berg Balance Scale. Aust J Physiother 2001; 47: 29–38.
34. Bandura A. Exercise of personal and collective efficacy in changing societies. In: Bandura A, editor. Self-efficacy in changing societies. Cambridge: Cambridge University Press; 1995, p. 145.
35. MacKay-Lyons MJ, Makrides L. Cardiovascular stress during a contemporary stroke rehabilitation program: is the intensity adequate to induce a training effect. Arch Phys Med Rehabil 2002; 83: 1378–1383.