OBJECTIVE: Most brain injuries occur in people of working age. Individuals with mild or moderate injuries may have unrecognized problems affecting return to work. Previous studies have focused on factors that predict return to work after brain injury. There is limited information about the experiences of individuals returning to work.
DESIGN: Individual interviews explored the work-related expectations and experiences of workers who had sustained mild to moderate brain injury. A sampling frame ensured a spread of participants by age, injury severity and work type.
METHODS: Thirty-three interviews were conducted 4–6 months post-injury. Most participants had returned to work. Interviews were transcribed verbatim for thematic analysis.
RESULTS: Key emerging issues for participants were the invisibility of their injury, continuing symptoms affecting their ability to do their job and lack of advice and guidance on returning to work. Return to work support systems were considered to be poorly coordinated and managed.
CONCLUSION: It is important that healthcare professionals anticipate the vocational rehabilitation needs of patients who have sustained mild to moderate brain injury. These patients may require additional coordinated interventions and specific person-centred information to ensure a successful and, most importantly, a sustained return to work.
Key words: brain injury, qualitative, work.
J Rehabil Med 2008; 40: 334–339
Correspondence address: Gill Gilworth, University of Leeds UK, Academic Unit of Musculoskeletal and Rehabilitation Medicine, University of Leeds, 36 Clarendon Rd, Leeds LS2 9NZ, UK. E-mail: gilworths@aol.com
Submitted June 7, 2007; accepted November 29, 2007
*This paper was presented as a poster at the winter meeting of the Society for Research in Rehabilitation Medicine on the 8th of Februaty 2007 in Sheffield (UK).
INTRODUCTION
Approximately 1.4 million people in Britain attend accident and emergency (A&E) departments each year with a head injury, constituting 11% of all A & E presentations (1). Most injuries are classified as mild, the majority of patients are discharged home within a few hours, and of those admitted the majority are retained for 48 h or less. Patients are often discharged with little or no follow-up, with rehabilitation focusing primarily on the severely injured (2). Approximately 63% of all brain injuries occur in people aged 15–64 years, i.e. the working population (3). One of the most common long-term consequences of brain injury is difficulty with or inability to return to work and estimates of the number of people who return to work following these injuries vary (4–6). Previous studies have identified factors that predict return to work (7, 8). In a recent review paper (9), Ownsworth & McKenna listed the factors most consistently associated with employment outcome as pre-injury employment status, both physical and cognitive functioning, executive functioning, involvement in vocational rehabilitation services and emotional status.
For those sustaining mild to moderate brain injury, significant numbers return to work with continuing symptoms (2, 10, 11). Most commonly reported are attentional deficits, such as impaired concentration and information processing capacity. However, information about individual experiences of returning to work after brain injury is limited. In a qualitative analysis of narratives of individuals who had sustained a head injury, Nochi (12) found that some survivors of mild head injuries reported that their injury was not significant enough to be a (serious) brain injury from a medical perspective, yet their lives were affected in a dramatic way. This highlights discrepancy between the likely “outcome” identified from clinical diagnosis and the lived experience of individuals with a brain injury.
The theoretical framework on which this study was based is that work is known to serve a number of important functions, including contributing to a person’s sense of identity and life satisfaction. Delay or inability to return to work has economic and personal costs. Participants in this study were in work at the time they sustained mild to moderate brain injury, enabling us to examine the expectations and experiences of workers recovering from brain injury. It is known that work-disabled individuals with other long-term conditions, for example rheumatoid arthritis, stroke and multiple sclerosis, show increased depression and reduced quality of life (QoL) (13, 14), whereas those who return to work report improved subjective well-being and life satisfaction and fewer unmet needs (15, 16). Consequently, it is reasonable to assume that the majority of those in work at the time of a brain injury will benefit from returning to work.
The aim of this study was to explore expectations and experiences of the return to work process through individual interviews, and to gain further insight into the experiences of those who had not been able to return, something which has not previously been reported in any detail. The study population of individuals who had sustained mild or moderate brain injury, who were in work at the time of their injury and interviewed relatively soon afterwards were chosen as a population likely to generate rich data relating first-hand experiences of the challenges experienced by people returning to work, and working with the consequences of a brain injury.
METHODS
Individual, semi-structured, in-depth interviews were used to explore the work-related expectations and experiences of workers who had sustained mild to moderate brain injury. The interviews were arranged at a time and venue to suit the participants. The majority of interviews were conducted in the participants’ homes, although some interviews were carried out at the university and some at the workplace, depending on individual preferences. Evening interviews were offered if required. Interviews were between 1 and 2 h in length. Four experienced interviewers facilitated the interviews, and interviewers and participants did not meet prior to the interviews.
The interviews concentrated on work factors, for example the impact of any remaining symptoms on the individual’s experiences when trying to return to, or continue in work following their brain injury. Although a brief topic list was used (Table I) the interviewees were encouraged to speak freely about any issues relevant to them in relation to their injury, its consequences and work.
Ethical approval was obtained from the local research ethics committee. Signed consent was obtained prior to each interview.
| Table I. Topic guide used for individual interviews |
| The accident or injury Personal and emotional impact Current issues/symptoms |
| Recovery | |
| Work Usual job demands/task analysis Issues at work in relation to injury Planning and organizing Relationships at work – colleagues and boss Process of getting back to work Possible adaptations at work If not back at work perceived barriers to return |
| Family and friends | |
| Social life and life – work balance |
Recruitment
All the A & E records at a busy general hospital in Leeds, a large city in the north of England were checked for a 3-month period. Those identified as eligible to participate in the study were sent a letter from the A & E consultant, with a participant information sheet and a form to return to the researchers at the university. On the form they were asked to record their employment status at the time of their injury, occupation and when they last worked.
Recruitment for the interviews was carried out using purposive sampling. All participants had to be in work at the time they sustained their brain injury. The aim was to recruit a spread of participants by severity of injury, age and type of work (see Table II). As part of the sampling process subjects were divided into 2 severity groups. The moderate group were those with a lowest recorded Glasgow Coma Score (GCS) in the range 9–13 or those admitted for 48 h or more because of their injury; the mild group were those with a lowest recorded GCS of 14 or 15. This information was obtained from the A & E records. With regard to employment participants were categorized into 2 groups: (i) blue-collar (manual and non-sedentary occupations) and (ii) white-collar workers (non-manual work, such as an office worker or manager). This information was obtained directly from the participants. All interviews took place 4–6 months post-injury; participants included some people who had returned to work and some who had not.
Analysis
With the participants’ consent all the interviews were taped and subsequently transcribed verbatim, and their content analysed. Thematic analysis and coding was undertaken by GG, SE and AC, commencing when the first 3 transcripts were available. In order to validate and increase reliability of the data, the main emerging themes from the first 6 interviews were discussed and agreed with the fourth qualitative interviewer.
Each transcript was read in full in order to obtain an overall perspective and identify emergent themes. Appropriate sections of transcripts were then coded and grouped together based on themes identified from the whole transcript. The emerging themes were compared with those in other transcripts as the analysis and development of the thematic structure continued. Re-reading and re-coding of earlier transcripts was carried out to ensure decisions about major themes and sub-themes were grounded in the content of the interviewee’s responses, in a process referred to as constant comparison (17).
RESULTS
A total of 75 potential participants returned forms indicating that they were willing to be interviewed. From those who were in work at the time of their brain injury, purposive sampling was then used to ensure a wide spread of participants as described above (Table II).
| Table II. Sampling frame used for individual interviews (n = 33) |
| | | Lowest recorded GCS |
| Age range (years) | Work status | 14 or 15 | 9–13, or admitted to hospital for ≥ 48 h |
| Blue-collar | White-collar | Blue-collar | White-collar |
| 18–34 | Back at work | 4 | 6 | 1 | 3 |
| Off sick/Lost job | 2 | 0 | 2 | 0 |
| 35–55 | Back at work | 2 | 5 | 2 | 2 |
| Off sick/Lost job | 0 | 1 | 1 | 2 |
| GCS: Glasgow Coma Scale. |
A total of 33 people were subsequently interviewed, (11 females, 22 males; mean age 37 years, age range 19–55 years). Eight interviewees were either still off work or had lost their job since their injury. It was not possible to recruit participants for all the cells in the sampling frame, for example there was a shortfall in participants who were not back at work. The participants had a range of occupations, e.g. mechanic, journalist, accountant, panel beater, police officer, plasterer, carpenter, security guard and solicitor.
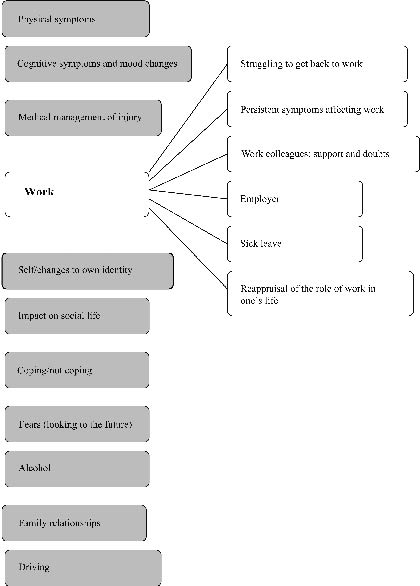
Although the topic list used to guide the interviews focused mainly on work, this was only one of the 11 major emergent themes (Fig. 1). In addition to work, the major themes identified were wide ranging and included aspects of the medical management of the injury, persistent physical symptoms, perceived changes to own identity by patient and family, cognitive symptoms and mood changes. Participants also identified impact on their social life, fears (looking to the future) and family relationships as important.
Fig. 1. Thematic structure following analysis of interview transcripts showing sub-themes within the major theme of “Work”.
The results reported here focus on the data regarding the major theme of work. The following work-related sub-themes emerged as important aspects of the consequences of brain injury:
• Getting back to work (including making adaptations at work and support systems)
• Persistent symptoms (affecting work or return to work plans)
• Work colleagues
• Employer
• Sick leave
• Stopping work (or choosing not to return)
The data is presented in 6 sections with representative quotes to illustrate these themes. Within some themes there were also a number of important further sub-themes that emerged from the analysis.
Sub-theme 1: struggling to get back to work
It was just like starting a new job all over again, I still write things down (pause) just to make sure.
This short quote summarizes the challenge of returning to work for an interviewee who had sustained what would be considered a moderate brain injury in medical terms. Most of the interviewees (25 of 33) in the study were back at work, although for many this had been a challenge. It was also clear that some participants felt that they had returned to work too soon, possibly because of lack of advice about work and how long their recovery might take. Most participants reported struggling when back at work, with a number of barriers they had had to overcome. In addition there was an added pressure of “having to prove yourself” once back at work in some cases:
I was trying to get on in my career and I just felt that I’d got this massive hurdle put in my way,… you really wanted to prove something but you know I was really struggling in the first 4 or 5 weeks.
In contrast, one interviewee had made her own decision about when she felt ready to return to work and saw this as part of her rehabilitation:
It was my idea to go back to work, my doctor wasn’t right happy about that but I did sort of point out to him that I felt it was good for my own rehabilitation that if I go back to work, get some normality back in my life that it would help and he said, “Yeah, fair enough, I agree with that” and it probably has.
Lack of support in the workplace was highlighted by some participants. Some felt there were unrealistic expectations of working at pre-injury levels immediately on return to work. It was notable that none of the participants recalled being given any advice or guidance on the best time to resume working or what to expect when they went back. Some simple vocational rehabilitation advice for the individuals and their employers would have helped some participants:
I think it’s just quite difficult because people just expect you to be straight up and running again once you’re back in work. I think that people assume that everything’s alright and that you should be working to the same level that you worked before.
Sub-theme 2: persistent symptoms affecting work
Persistent symptoms were described by those who had returned to work and those who had not managed to go back to work (or who had chosen not to). There were a number of further sub-themes including the “invisibility” of symptoms, such as problems with memory and concentration. In addition, a perceived decline in skill level compared with pre-injury and a reduced capacity to plan and organize the work were affecting some interviewees’ confidence and mood in the workplace.
I do try and concentrate more, although that was one of the things that I had great difficulty with after the accident was concentrating and thinking, … now I’ll repeat something over in my mind again and again and again.
…that skill level will suddenly just drop and it will last for the rest of the day, my confidence is gone, so, you know, have to go to bed, go to sleep, wake up next morning, fresh start…
For some interviewees changes post-injury were less specific, but they tended to describe a feeling of either “not being with it” or being distanced from their day to day working life. Some participants perceived their symptoms as a sign of weakness and there was increased anxiety about their ability to do a good job.
I’d say for, several weeks after the accident I didn’t feel quite right…. I continued to feel a little bit dazed and just not quite with it really, not all day long, but just for periods of the day.
It was, it was like I wasn’t really there (at work), if you know what I mean. It was like it was happening and I wasn’t really a part of it.
It started to play on my mind you know, was I impressing them enough and was I doing a good job and you know all them things so you know lost a bit of self-confidence in work.
Sub-theme 3: work colleagues – support and doubts
All the participants who had returned to work talked about their employer and/or work colleagues. Experiences varied in terms of colleagues’ expectations and their level of understanding of brain injury. In most cases colleagues were supportive.
…they were quite good…they said take your time to get your confidence back.
…everybody were very supportive, as they’re supposed to be you know.
The invisibility of a brain injury has already been mentioned. With no “visible injury” some participants felt that their work colleagues doubted whether their difficulties were genuine. This may have been related to lack of understanding of the impact of brain injury:
Whilst I thought that my senior management they were giving me the support you got the feeling that other colleagues were a little bit, erm, doubting because you can’t see it …. I think it breeds a little bit of resentment really or you know they don’t quite understand the problem.
Sub-theme 4: employer
The reported reaction of employers was also mixed; some employers were perceived as being more supportive and understanding than others. Again, lack of information about the effects of brain injury in relation to work to pass on to their employer was an issue for some:
I told my boss at the time what symptoms I can potentially have, but then it’s just how widely that is communicated…it’s something that probably should have gone out to the rest of the team and been explained to them and that probably didn’t happen…..looking back it should have done just so people understand.
In some cases the benefits of having a flexible approach to return to work and allowing a phased build-up of work hours was evident, however some interviewees had chosen not to disclose continuing symptoms to their employer because they perceived that their symptoms may be seen as a sign of inability to undertake the work
Work were fantastic about it …making sure that I went early and came in a bit later to start with you know, just did what I could cope with basically, so they were brilliant…really supportive.
Interviewer: Does anyone know at work?
Interviewee: No, no-one at all.
Interviewer: Why didn’t you tell them?
Interviewee: Male ego – they knew about the mugging incident (pause) don’t know about any of the symptoms. Everyone knew about the incident, everybody was very supportive…but the other side of the coin, the after-affects are just signs of weakness.
Sub-theme 5: sick leave
Sick leave was an important theme because of the potential consequences of even a relatively short period off work for some people:
I told them I have to go to work even though they (hospital staff) said you shouldn’t be going to work…I’ve actually lost my house now because I didn’t have enough money (for the rent).
A more typical reaction was to feel under pressure to go back to work quickly because of concerns over their work attendance record and comments from colleagues. In addition some participants felt that taking time off work was something that could affect their chances of promotion or future employment:
I was getting a lot of comments about being off sick all the time which really, really frustrated me.
I don’t know how I managed to get through the week…but I felt I couldn’t take any more time off. It’s just that I think my boss has the opportunity of putting a black mark against my name mentally then it could affect me later on.
…it’s a corporate environment, catch up with that sort of thing, stops the promotion.
Sub-theme 6: reappraisal of the role of work in one’s life
Eight of the 33 interviewees were either still off work or had lost their job since their injury. Within this group there was a wide range of experiences. Some of them were still intending to return to work and were still in communication with their employer. This group tended to experience anxiety, feeling the pressure from their colleagues to return and unsure whether they would be able to do their job if they were to go back. For others it was the employer who was reluctant to take what might be seen as a risk of having someone back at work that was not fully recovered.
I mean it might be all right, but it might not, so nobody dare take the risk; same as going back to work, they won’t let me go back to work because if anything happened …
Finally, a small group felt that the brain injury had appeared to change their attitude to work, given them an opportunity to re-appraise their priorities in life or simply affected their motivation to work. Below are 2 quotes from people who had been back at work for a short time after their injury but by the time of the interview were not working out of choice:
I’ve noticed that my attitude to work has changed; whereas before I was quite uptight about it, since then I’ve just thought what’s the point of putting yourself through that sort of stress, so I’ve taken a step back. That’s part of the reason why I’m not going to work now.
I wasn’t really caring about it [work] and I found it hard to motivate myself…felt like I was just in the wrong job really.
DISCUSSION
In this study in-depth individual interviews with participants across a varied range of occupations showed some individual differences, although in many of the cases their experiences of getting back to work were similar. Most of the participants (25 out of 33) had returned to work by the time of their interview, although some reported significant persistent symptoms. These included problems with concentration, memory and executive functioning, leading to lack of self-confidence in some cases. This is consistent with the findings of previous studies (4–8). The support systems, or lack of support in the workplace and unrealistic expectations of working at pre-injury level immediately when people returned to work were highlighted by some participants. It was also clear that some participants felt that they had returned to work too soon, although in contrast one interviewee had made her own decision about when she felt ready to return to work and saw it as part of her rehabilitation.
The importance of vocational outcome as a measure of the success of rehabilitation following brain injury is widely acknowledged; Leverack et al. (18) also suggests that subjective evaluations that include job satisfaction and quality of non-work life are needed. Work serves a number of important functions, including contributing to a person’s sense of identity and life satisfaction. O’Neill et al. (19) found that employment was significantly related to QoL for individuals who had sustained brain injury. In addition, work-disabled individuals with other long-term conditions, for example rheumatoid arthritis and multiple sclerosis, have been shown to suffer increased depression and reduced QoL (13, 14). However, individuals who return to work after stroke report significantly higher subjective well-being and life satisfaction and fewer unmet needs (20, 21). Although for some brain injury survivors return to work may be unrealistic, it is reasonable to assume that the majority of those in work at the time of their injury will want to go back to work.
Many of the participants in this study (particularly those who had sustained mild injuries), had not received formal medical follow-up. However, even those who had rehabilitation or had reported contact with their primary care doctor could not recount any detailed discussions about the return to work process. This may, of course, relate to some participants’ cognitive problems, but it does highlight the lack of work-related advice given by healthcare professionals. Key issues for the participants who were back at work were the invisibility of the consequences of their injury and persistent symptoms affecting their ability to work. Lack of advice and guidance on the best time to resume working meant that some had returned too soon. It was felt that return to work support systems were poorly coordinated and managed. Participants lacked information and advice on the benefits of phased return to work, coping strategies (although some individuals had adopted their own strategies) and in-work support that could be available through other agencies, for example the government agency Jobcentre Plus.
This study suggests that the vocational rehabilitation needs of people sustaining mild to moderate brain injury are sub-optimal. It is essential that appropriate information and advice to facilitate return to work is supplied at the earliest opportunity, both to the patient and employer. Such information has the potential to reassure patients and employers and reduce the likelihood of secondary symptoms such as anxiety. This is supported by Ponsford et al. (22), who have reported that early, but inexpensive, intervention in the form of an information booklet has been shown to have a significant impact on anxiety and ongoing problems following mild brain injury. Such information should include potential symptoms and how they might be manifest and affect work, workplace environment, coping strategies, and reassurance about return to work in spite of continuing symptoms provided appropriate support is in place in the workplace.
We recognize that our findings are drawn from a sample of participants with brain injury who all presented at a single hospital in the north of England, and a question therefore arises as to the generalizability of the results. In addition, participants were interviewed on only one occasion (4–6 months post-injury), so there is a degree of reliance on interviewee’s retrospective memories.
In conclusion, following a minor or moderate head injury, people continue to experience a number of symptoms that affect their capacity to work. It is important that doctors and other healthcare professionals anticipate the vocational rehabilitation needs of patients who have sustained mild to moderate brain injury. Such patients may require additional coordinated interventions to ensure a successful and, most importantly, a sustained return to work.
There is some evidence that simple information delivered in a timely manner can reduce anxiety and ongoing problems following brain injury and this type of approach warrants further study, particularly if suitable information could be designed to help reduce the “mystery” surrounding invisible symptoms and give advice and support about work.
Further research in the area of brain injury and return to work systems could include studying innovative ways of working across agencies in both the health and employment sectors to help maximize job retention in this population.
ACKNOWLEDGEMENTS
We would like to thank Remedi UK for providing financial support for this study.
We would also like to thank Glyn Smyth (Work Fit Ltd) who helped with the interviews, Vikki Lane for producing transcripts from the audio tapes, and all the participants in the study.
REFERENCES
1. Tennant A. Admission to hospital following head injury in England: incidence and socio-economic associations. BMC Public Health 2005; 5: 21.
2. King NS, Crawford S, Wendon JJ, Moss NEG, Wade DT. Interventions and service need following mild and moderate head injury: the Oxford Head Injury Service. Clin Rehab 1997; 11: 13–27.
3. Kalsbeek WD, McLaurin RL, Harris BS 3rd, Miller JD. The national head and spinal cord injury survey: major findings. J Neurosurg Suppl 1980; 53: S19–S29.
4. MacKenzie EJ, Morris JA Jr, Jurkovich GJ, Yasui Y, Cushing BM, Burgess AR, et al. Return to work following injury: the role of economic, social, and job-related factors. Am J Public Health 1998; 88: 1630–1637.
5. Greenspan AI, Wrigley JM, Kresnow M, Branche-Dorsey CM, Fine PR. Factors influencing failure to return to work due to traumatic brain injury. Brain Inj 1996; 10; 207–218.
6. Stambrook M, Moore AD, Peters LC, Deviaene C, Hawryluk GA. Effects of mild, moderate and servere closed head injury on long-term vocational status. Brain Inj 1990; 4: 183–190.
7. Van der Naalt. Prediction of Outcome in mild to moderate head injury: a review. J Clin Exp Neuropsychol 2001; 23: 837–851.
8. Keyser-Marcus LA, Bricout JC, Wehman P, Campbell LR, Cifi DX, Englander J, et al. Acute predictors of return to employment after traumatic brain injury: a longitudinal follow-up. Arch Phys Med Rehabil 2002; 83: 635–641.
9. Ownsworth T, Mc Kenna K. Investigation of factors related to employment outcome following traumatic brain injury: a critical review and conceptual model. Disabil Rehabil 2004; 26: 756–784.
10. Englander J, Hall K, Stimpson T, Chaffin S. Mild traumatic brain injury in an insured population: subjective complaints and return to employment. Brain Inj 1992; 6: 161–166.
11. Van Der Naalt J, Van Zomeren AH, Sluiter WJ, Minderhoud JM. One year outcome in mild to moderate head injury: the predictive value of acute injury characteristics related to complaints and return to work. J Neurol Neurosurg Psychiatry 1999; 66: 207–213.
12. Nochi M. “Loss of self” in the narratives of people with traumatic brain injuries: a qualitative analysis. Soc Sci Med 1998; 46: 869–878.
13. Chaney JM, Mullins LL, Uretsky DL, Doppier MJ, Palmer MJ, Wees SJ, et al. Attributional style and depression in rheumatoid arthritis: the moderating role of perceived illness control. Rehabil Psychol 1996; 41: 205–223.
14. Aronson KJ. Quality of life among persons with multiple sclerosis and their caregivers. Neurology 1997; 48: 74–80.
15. Kersten P, Low JTS, Ashburn A, George SL, McLellan DL. The unmet needs of young people who have had a stroke: results of a national UK survey. Disabil Rehabil 2002; 24: 860–866.
16. Vestling M, Tufvesson B, Iwarsson S. Indicators for return to work after stroke and the importance of work for subjective well-being and life satisfaction. J Rehabil Med 2003; 35: 127–131.
17. Weber R, editor. Basic content analysis. London: Sage Publications Inc; 1990.
18. Levack W, McPherson K, McNaughton H. Success in the workplace following traumatic brain injury: are we evaluating what is most important? Disabil Rehabil 2004; 26: 290–298.
19. O’ Neill J, Hibbard MR, Brown M, Jaffe M, Sliwinski M, Vandergoot D, Weiss MJ. The effect of employment on quality of life and community integration after traumatic brain injury. J Head Trauma Rehabil 1998; 13: 68–79.
20. Saciri BM, Kos N. Aneurysmal subarachnoid haemorrhage: outcomes of early rehabilitation after repair of ruptured intracranial aneurysms. J Neurol Neurosurg Psychiatry 2002; 72: 334–337.
21. Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros RC, et al. Guidelines for the management of aneurysmal subarachnoid haemorrhage. Stroke 1994; 25: 2315–2328.
22. Ponsford J, Willmott C, Rothwell A, Cameron P, Kelly A-M, Nelms R, et al. Impact of early intervention on outcome following mild head injury in adults. J Neurol Neurosurg Psychiatry 2002; 73: 330–332.