OBJECTIVE: To explore and compare severely injured patients’ rehabilitation goals with respect to their functioning and the reported goals of rehabilitation professionals.
DESIGN: A prospective cohort study, including longitudinal data on patients’ functioning and cross-sectional data from the patients’ and professionals’ goal descriptions.
SUBJECTS: Sixty-six patients (53 men, 13 women, mean age 35 (standard deviation 13.8) years) with multiple injuries with a New Injury Severity Score > 15 and 76 physiotherapists and other municipal rehabilitation professionals/services.
METHODS: Patient questionnaire and interview were applied after return home and a further questionnaire one year post-injury. Short-Form Health Survey was used for self-assessed health. A questionnaire was applied to the professionals. Rehabilitation goals were reported by patients and professionals. International Classification of Functioning, Disability and Health coding of the goals was performed.
RESULTS: Short-Form Health Survey scores were below those of the general population. The patients’ goals concerned body functions/structures (8.6%), activities (16.2%) and participation (31.7%). The professionals, mainly physiotherapists, reported few participation goals (10.7%). Agreement between the patients’ and professionals’ goals were poor, with kappa scores ≤ 0.20 for musculoskeletal functions/structures, self-care, mobility, interpersonal interactions/relationships, work and recreation/leisure. A statisticaly significant difference between patients’ and professionals’ goals was demonstrated for musculoskeletal functions/structures (p < 0.001), interpersonal interactions/relationships (p = 0.002), work (p =0.001) and recreation/leisure (p = 0.002).
CONCLUSION: The patients mainly reported activity and participation goals. There was poor agreement between patients and professionals for body functions and participation goals.
Key words: multiple trauma, rehabilitation, goals, ICF.
J Rehabil Med 2008; 40: 340–346
Correspondence address: Helene L. Soberg, Department of Physical Medicine and Rehabilitation, Ulleval University Hospital, N-0407 Oslo, Norway. E-mail: h.l.soberg@medisin.uio.no; helene.soberg@ulleval.no
Submitted May 2, 2007; accepted December 18, 2007
INTRODUCTION
Rehabilitation following severe multiple injuries is emphasized as important in a perspective that has developed from saving lives to restoring functioning and quality of life. In recent years goal setting has been considered increasingly important in rehabilitation, and fundamental in order to take the process forward (1–3). Goal setting has been defined as a process of agreeing on goals (3) or, more broadly, as the establishment of goals (4). Improving rehabilitation outcomes and enhancing patient autonomy are among the main purposes for goal setting. Goals can be patient devised, mutually agreed, or staff-directed, and should be set both at a team level in multidisciplinary rehabilitation and at the level of a single health professional (3, 5). Goal setting is a dynamic process, and short- and longer term goals are important (1). In an analysis of rehabilitation goals it will be of interest to study to what extent the goals formulated by rehabilitation personnel are similar to or discrepant from the goals held by patients.
In rehabilitation of patients with multiple injuries the rehabilitation goals will be related to the severity and nature of sudden and serious losses of functioning, often with profound long-term consequences (6–8). At the impairment level, patients may experience musculoskeletal and pain problems, as well as reduced cognitive and mental health (8–11). They also often report problems related to activities and participation comprising mobility, social- and role-functioning, and return to work. The post-injury problems may be considered to constitute a basis for their rehabilitation goals.
The rehabilitation concept comprises the process, structure and outcome, and goal setting is considered a core skill (12). An underlying premise in goal setting research is that the outcomes considered important by the professionals should be in accordance with those of the patients. However, in practice this is not always the case (1). Most research founded on goal setting relates to specific patient groups, and has been performed mainly in inpatient rehabilitation settings (2, 5, 13–17). Aspects of the process and the goals set have been studied. Patients with multiple sclerosis and their rehabilitation team have been shown to agree on less than 2 of 5 prioritized goals from a pre-existing list (14). Mobility was a goal selected by both the patients and the team. In another study, patients with stroke had goals that concerned activities of daily living and mobility, whereas physiotherapists focused mainly on mobility, and occupational therapists on activities of daily living and communication (13). The level of agreement between rheumatic patients’ and their physiotherapists’ goals was relatively low, with mostly fair to moderate agreement for pain, range of motion and muscle strength (15). Physiotherapists focus mainly on body functions and activities in their approaches to patients’ problems and goals (13, 18), whereas occupational therapists to a larger extent emphasize communication, personal care, other activities and participation (13, 18). However, the context of the rehabilitation process for patients with severe multiple injuries after return home differs from these studies due to the community setting, the patients’ young age and diversity of functional problems post-injury. To our knowledge, except for a tutorial article, there are no studies of post-discharge rehabilitation in the community for patients with severe multiple injuries in which the rehabilitation goals reported by the patients and rehabilitation providers, respectively, have been explored (19).
The International Classification of Functioning, Disability and Health (ICF) presents a multidimensional perspective on functioning and may be applied both in the analysis of disability and in the setting of rehabilitation goals. The ICF is a recommended tool for rehabilitation research that enables perspectives and inter-individual differences in functioning and rehabilitation to be explored (11, 12, 20), and should thus be well suited for analysis of agreement and discrepancies between patients and providers in terms of rehabilitation goals.
The importance of continued rehabilitation in the community for patients with severe multiple injuries after return home has been emphasized (6) and is considered increasingly important (21). The municipal rehabilitation organizations in Norway mainly provide generic rehabilitation services, mostly performed by physiotherapists and occupational therapists, but may also involve social, educational or vocational services. Furthermore, physiotherapists in private practice often have contracts that oblige them to participate in municipal rehabilitation provision. Thus, patients receive rehabilitation measures from municipal rehabilitation organizations and/or physiotherapists in private practice. Both the municipal rehabilitation services and the physiotherapists in private practice are financed through public insurance systems.
To be able to improve outcomes in locally based rehabilitation, however, it is important to gain knowledge of concurrent patient and provider goals in the process. Thus, the specific aims of this study were to identify the rehabilitation goals in the community from the patients’ and municipal rehabilitation professionals’ perspectives, and to analyse potential discrepancies between the groups in these goals for severely injured patients after their return home.
More specifically the study examined the following questions:
• Which self-reported short- and long-term rehabilitation goals were reported by the patients and by the professionals, respectively, according to the ICF?
• Do the patients' goals reflect their self-reported functioning and health?
• What are the agreements and differences between the patients and the providers reported goals?
Material and methods
This study is part of a prospective cohort study of patients with severe multiple injuries performed at Ulleval University Hospital (UUH) in Oslo, Norway. Post-injury functioning and the rehabilitation process in the community are studied (7, 22). The study was approved by the Norwegian Data Inspectorate and the Regional Committee for Medical Research Ethics.
Study population – patients and professionals
The patient population consisted of consecutive trauma patients from eastern and southern parts of Norway admitted to Ulleval University Hospital within 24 hours after the injury from January 2002 through June 2003. Inclusion criteria were: patients aged 18–67 years, with a New Injury Severity Score (NISS) > 15, with at least 2 injuries classified in the Abbreviated Injury Scale (AIS) injury scoring system (23, 24). Exclusion criteria were: former multiple trauma, substance addiction or severe psychological disease registered in the medical records, or insufficient command of Norwegian. Data were collected on 105 patients. The full sample of 105 patients has been described elsewhere (7, 22). For the present study only patients who received rehabilitation in the municipalities after their return home and for whom data on both patient and provider goals were available, were included.
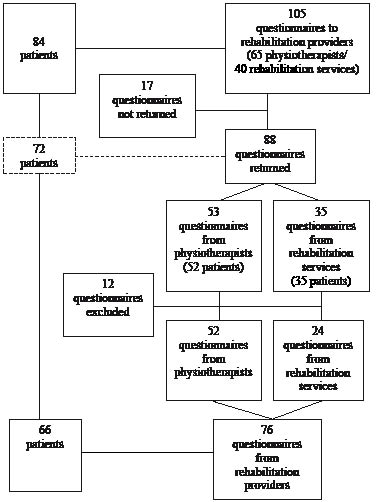
Professionals providing rehabilitation in the community were contacted based on information from the patients. Of the full sample of 105 patients, 84 had contact with 105 rehabilitation professionals, representing both municipal rehabilitation services (n = 40) and physiotherapists in private practice (n = 65). Twenty-one patients named both contacts within the rehabilitation service and physiotherapists in private practice. Forty-nine percent of the professionals were women; their mean age was 40.7 (standard deviation (SD) 10.1) years. They were sent a questionnaire, of which 88 (84%) were returned. Twelve questionnaires that contained no goal information were excluded. There were no significant differences in age or gender between the responders and non-responders. The 24 questionnaires from the rehabilitation services were submitted by 10 physiotherapists, 8 occupational therapists, 4 nurses, 2 rehabilitation co-ordinators and one social worker. The 76 included questionnaires contained goal information concerning 66 patients. Only data from these 66 patients are presented here. In cases where more than one questionnaire per patient was received from the professionals, the information was considered to be potentially complementary, and was thus all included. Fig. 1 shows the process of inclusion for the 66 patients and their professionals.
Fig. 1. Inclusion process, from the initial 84 patients with multiple injuries and their 105 treating rehabilitation professionals who were sent a questionnaire, to the included 66 patients and 76 professionals. (Note: 10 patients received services from both rehabilitation services and community physiotherapists in private practice).
The 66 patients’ mean age was 35.0 (SD 13.8) years, 80% were male, 82% had high school or higher education, 71% were blue-collar workers. The median length of stay in hospital/rehabilitation institution was 97 days (inter-quartile range (IQR) 113). Inpatient rehabilitation was provided for 77% of the patients before their return home. They lived in 51 different municipalities. The majority (77%) was injured in traffic. Mean number of injuries was 7.4 (SD 3.6). NISS was 34.4 (SD 12.9). Glasgow Coma Scale (GCS) score was 12.6 (SD 3.8). Table I shows the injured body areas. There were no significant differences between the full sample and the included 66 patients concerning age, gender, education or injury severity variables, nor differences in goal descriptions (data not shown).
| Table I. Injured body regions. Patient frequencies for the 66 patients with multiple injuries* |
| Body regions | Patients’ frequency | Specifics |
| Head | 34 | GCS ≤ 9 in 14 patients (severe) GCS 9–12 in 8 patients (moderate) |
| Face | 17 | |
| Chest | 37 | |
| Abdomen/pelvic contents | 21 | |
| Spine total | 37 | Spinal cord injuries: 6 incomplete, 8 complete |
| Upper extremities | 31 | 1 amputation |
| Lower extremities | 48 | 2 amputations |
| *Frequencies do not include multiple injuries in one body region. GCS: Glasgow coma scale. |
Methods
Information was collected by a patient interview 6 weeks after return home (median), which was 20.0 (SD 9.5) weeks post-injury. Questionnaires about self-reported health and functioning were completed prior to the interviews, and at one year post-injury. Information about diagnosis and injury severity was collected from the Trauma Registry at Ulleval University Hospital, Oslo, Norway (2003).
Injury severity. The injuries were scored according to the AIS on a scale from 1 to 6 (minor–maximum injury) (24). The NISS expresses the severity of the 3 most severe injuries (23). A score above 15 is considered a serious injury. The GCS expresses the degree of motor, verbal and eye opening response on a scale from 3 to 15 (25). A score of 3–8 indicates severe, 9–12 moderate and 13–15 mild/no brain injury.
Functioning. The Short-Form Health Survey (SF-36) measures self-reported health status, with scales for physical functioning, role-physical function, bodily pain, general health, vitality, social functioning, role-emotional function and mental health. The scale range is 0–100, worst to best (26). Norwegian general population data for SF-36 weighted for gender and age were used for comparison (27). Work status was also registered.
Patient interview. The structured interview had several open-ended questions about the rehabilitation process. Three questions about goals were selected for the present study. In order to clarify the rehabilitation concept the questions had an introduction stating: “In rehabilitation it is emphasized that you should achieve best possible functioning physically, mentally and with respect to family, friends, work and leisure”. The questions were: What are your most important rehabilitation goals? What is most important for you right now? (Short-term perspective) What are your goals for the future? (Long-term perspective) The answers were written down by the interviewer (author H.L.S.) using the patient’s own words, and read out to the patients, who either accepted or corrected them. This procedure strengthened the validity of the raw text (28).
Rehabilitation providers – questionnaire. The rehabilitation professionals received a questionnaire as soon as possible after the patient interview. It concerned the rehabilitation process and contained several open-ended questions about their respective patients’ problems, resources and short- and longer term goals. For the present study the responses to the goal questions were selected.
ICF and analysis of goals
The ICF consists of 4 classifications: Body Functions (b), Body Structures (s), Activities and Participation (d), and Environmental Factors (e). Activities (a) and Participation (p) can be applied separately. In this study the ICF domains “d7 Interpersonal interactions and relationships”, “d8 Major life areas” and “d9 Community, social and civic life” were characterized as participation. Inter-rater and intra-rater reliability of the ICF in classifying instruments and descriptions of functioning have showed moderate to excellent results (29–31). The raw text materials for coding in this present study were transcriptions of rehabilitation goals from questionnaires (professionals) and interviews (patients). Linking rules developed for linking descriptions of functioning to the ICF categories were applied (32). Second-level categories (3-digit codes) were used since they are considered to provide the best trade-off between breadth and depth of coding functioning (20). According to the rules, concepts to which it is not possible to assign a specific ICF code, should be assigned a code of “not definable general health” (ndgh), “not definable physical health” (ndph), “not definable mental health” (ndmh) or “not definable quality of life” (ndqol) (32). The distinction between ndqol and ndgh was based on whether the text referred to goals related to the patient as a person (Getting back to being me) or to their way of living (Living the way I did before, all included), whereas the ndgh category covered aspects of general health (Getting well again; Getting my health back). One additional category labelled “not definable activities and participation” (ndap), was formed (Function in my daily life, Be active like before, Function in my roles) since activities and participation goals are central in rehabilitation (11, 12). Furthermore, the background for ndap goals may be rooted in physical or mental health problems that are not explicit enough to be coded as either ndph or ndmh.
The ICF coding of the goal descriptions in the present study was performed by the first author, HLS. The coding procedure was first tested in a study of reliability of the ICF for the current project, in which HLS was one of the experienced raters (29). The kappa scores were 0.78 (good) for inter-rater and 1.00 (excellent) for intra-rater reliability for the experienced raters (29). In order to control for the potential bias associated with the fact that the coder is a physiotherapist, a selection of goals was coded by an occupational therapist experienced with the ICF. There was a high level of agreement in the coding (> 90%). The not definable coding was also discussed until agreement was reached.
Statistics
Descriptive data are presented by means, SD or by median and IQR or range. One-sample t-tests with the reference population scores as test-values were performed on the self-reported health scales. Cross-tabulations with χ2 tests were performed for nominal data. The level of agreement between the patients’ goals taken together and the rehabilitation professionals’ goals was tested with kappa statistics. Six groups of goals were formed, comprising the most frequently reported goal concepts and ICF codes from the 66 patients’ and their providers’ reported goals. They were: musculoskeletal functions/structures (all categories in b7, s7), mobility (categories d450–d469), self-care (all categories in d5), interpersonal interactions and relationships (all categories in d7), work/education (categories d820, d830, d850) and recreation and leisure (category d920) (11). These codes comprised 75% of the patients’ and 65% of providers’ short- and longer term goals coded with 3-digit codes. An agreement required coding of a similar concept from the goal descriptions presented by the patients and professionals. Examples were “walk properly again” (patient) and “walk normally” (professional), both coded as “d450 Walking” and thus registered as an agreement. Kappa is a measure of strength of agreement corrected for agreement by chance. A kappa level ≤ 0.20 is considered poor, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 good and 0.81–1.00 excellent (33). Non-parametric sign test for 2 related samples was used to test for statistical difference between patients’ and professionals’ coded goals. p-values of ≤ 0.05 were considered statistically significant. Analyses were performed using SPSS for Windows version 14 (SPSS Inc, Chicago, IL, USA).
Results
Self-reported disability and functioning
Table II shows that the 66 patients’ self-reported functioning and health was significantly lower than the reference populations on all scales. Although the largest difference was for the physical health scales, psychosocial functioning was also reduced throughout the first year post-injury. At their return home all patients reported worse physical functioning than the population norm, with the mean score being > 4 SDs below the Norwegian population mean (27). One year post-injury 94% reported lower scores, with a mean > 3 SDs worse than the population mean. Twenty-three percent of the 66 patients working/studying pre-injury had completely returned to work at one year post-injury.
| Table II. SF-36 after return home and one year post-injury for the 66 patients with multiple injuries. Differences in scores to general population scores |
| ICF components | 6 weeks after return home n = 65 Mean (SD) | 1 year post-injury n = 65 Mean (SD) | 1 year post-injury. Difference to norm Mean |
| Physical functioning | 40.6 (25.8) | 55.8 (32.3) | –37.9* |
| Role-physical | 6.9 (18.0) | 25.8 (37.5) | –60.6* |
| Bodily pain | 49.7 (27.9) | 58.3 (26.6) | –20.9* |
| General health | 60.0 (21.4) | 64.1 (18.6) | –17.0* |
| Vitality | 45.6 (21.6) | 53.7 (20.6) | –8.7* |
| Social functioning | 57.5 (28.2) | 69.8 (29.4) | –19.0* |
| Role-emotional | 51.3 (46.4) | 65.6 (41.7) | –20.3* |
| Mental health | 69.9 (19.1) | 71.6 (18.2) | –7.9* |
| *p ≤ 0.001 SD: standard deviation; ICF: International Classification of Functioning, Disability and Health; SF-36: Short Form of Health Survey. |
Rehabilitation, patients’ and professionals’ goals
The 66 patients reported a total of 581 goal concepts. Most important now were 179 goals, mean per patient was 2.8 (SD 1.5), range 1–7. Furthermore, they reported 184 most important rehabilitation goals, mean per patient was 2.7 (SD 1.2), range 1–5, and 218 future life goals, mean per patient 3.3 (SD 1.5), range 1–6. Table III shows the distribution of the ICF components and the not definable codes for the patients and providers.
| Table III. Distribution of the ICF components body functions/structures, activities/participation* and environmental factors and the not definable categories applied on the reported goals for 66 patients with multiple injuries and on the provider’ goals |
| ICF components and not definable categories | Coded goals, patients (%) n = 66 | Coded goals, professionals (%) n = 76 |
| Body functions/structures | 8.6 | 52.8 |
| Activities | 16.2 | 19.6 |
| Participation | 31.7 | 10.7 |
| Environmental factors | 4.5 | 5.8 |
| Not definable physical health | 5.2 | 4.6 |
| Not definable mental health | 2.6 | 0.7 |
| Not definable general health | 12.1 | 1.7 |
| Not definable activities and participation | 9.6 | 3.2 |
| Not definable quality of life | 9.6 | 1.0 |
| Sum | 100 | 100 |
| *ICF domains “d7 Interpersonal interactions and relationships”, “d8 Major life areas” and “d9 community, social and civic life” were characterized as participation. ICF: International Classification of Functioning, Disability and Health. |
The 5 most frequently applied 3-digit ICF codes on the patient goals are shown in Table IV. The code “d570 Looking after one’s health” was most frequently applied on goals reported as important right now, and mostly concerned training/performing exercises to regain physical functioning. “Work (d850)” was the second most frequently applied code described as important right now. As opposed to frequency of training, the frequency of work increased within a longer term perspective on the rehabilitation process. Some goals were reported in all 3 goal perspectives. They were “Walking (d450)”, “Family and Intimate relationships (d760–d770)”, “Remunerative employment/work (d850)” and “Recreation/Leisure (d920). Approximately 80% of the 66 patients reported work/education goals. Few goals related specifically to body functions such as musculoskeletal functioning or pain, and these were not among the most frequently reported goals. A total of 39% of the goals were given a not definable code.
| Table IV. Frequencies of the 5 most frequently applied 3-digit ICF codes among each of the 179 short-term, 184 and 218 longer term goal concepts reported by the 66 patients and among the 413 short- and longer term goals reported by the professionals, respectively |
| ICF code and text | Patients | Professionals |
| Most important right now | Most important rehabilitation goals | Future life goals | Short- and longer term goals |
| b280 Pain | | | | 25 |
| b710 Mobility of joints functions | | | | 46 |
| b730 Muscle power functions | | | | 59 |
| d230 Carrying out daily routine | 7 | | | |
| d450 Walking | 7 | 15 | 7 | 23 |
| d475 Driving | | 4 | | |
| d570 Looking after one’s health | 17 | 7 | | |
| d760 Family relationships/ d770 Intimate relationships | 10 | 4 | 16 | |
| d820 School education/ d830 Higher education | | | 11 | |
| d850 Remunerative employment | 12 | 29 | 39 | 22 |
| d920 Recreation/leisure | 8 | 8 | 24 | |
| ICF: International Classification of Functioning, Disability and Health. |
As for the rehabilitation providers, more than one-third of the 413 coded goal concepts concerned musculoskeletal functions and structures. Mobility (walking/driving) comprised 12% of the goals, and the participation goals of interpersonal interactions and relationships, work/education and recreation/leisure comprised 10% of the goal concepts (data not shown). The 5 most frequently applied 3-digit ICF codes for the provider goals are shown in Table IV. “Mobility of joint functions (b710)” and “muscle power functions (b730)” were the 2 dominating groups. Eleven percent of the goals were given one of the not-definable codes.
The levels of agreement among the 6 most frequently reported groups of patient goals: musculoskeletal functions/structures, mobility, self-care, interpersonal interactions/relationships, work/education and recreation/leisure were tested for the 66 patients and their rehabilitation professionals. The results are shown in Table V. Agreement occurred either when patient and professional(s) both described a goal within a goal group, or when none of them reported a goal within the group. Table V also shows agreement within a goal group when the goal was reported by the patient. Percentage agreements ranged from 48.5% for work/education to 65.2% for interpersonal interactions and relationships. Work/education goals were reciprocated by the professionals for 40.4% of the patients. The professionals reported goals related to musculoskeletal functions for 60.0% of the patients who themselves did not mention such goals (not shown in Table V). Mobility goals were set for 50.0% of the patients who reported such goals, but also for almost one-third of the patients who did not describe a mobility goal (not shown in Table V). For all 6 groups of coded goal concepts, agreement measured by kappa was poor. Sign tests for statistical difference between the patient and provider goals showed that the providers reported significantly more goals related to musculoskeletal functions/structures (p < 0.001), and significantly fewer goals concerning interpersonal interactions/relationships (p = 0.001), work/education (p < 0.001) and recreation/leisure (p < 0.001) than the patients.
| Table V. Rehabilitation goals within the 6 groups of coded goals for the 66 patients and their professionals. Patient frequencies of within a goal group, percentage agreement between patients/providers and between patients/providers when the goal was reported by the patient (kappa scores) |
| Goal group based on ICF | Patient frequency (%) in goal group | Professional frequency (%) in goal group | Agreement patients/ providers (%) | Agreement patients/providers for goals reported by patient (%) | Kappa score |
| Musculoskeletal function (b7, s7) | 16 (24.4) | 43 (65.2) | 50.0 | 81.3 | 0.14 |
| Mobility (d450, d460, d465) | 22 (33.3) | 24 (36.4) | 63.6 | 50.0 | 0.20 |
| Self care (d5) | 23 (34.8) | 4 (6.1) | 59.1 | 0.0 | –0.12 |
| Interpersonal interactions and relations (d7) | 24 (36.4) | 5 (7.6) | 65.2 | 12.5 | 0.09 |
| Work/education (d820, d830, d850) | 52 (78.8) | 24 (36.4) | 48.5 | 40.4 | 0.11 |
| Leisure/recreation (d920) | 31 (47.7) | 8 (12.3) | 57.6 | 19.4 | 0.14 |
| ICF: International Classification of Functioning, Disability and Health. |
Discussion
This study is the first to report data on rehabilitation goals from patients and community rehabilitation providers in a sample of patients with multiple injuries. A marked discrepancy was found between the patients’ and providers’ reported goals. The patients emphasized activities and participation, whereas the professionals, the majority of whom were physiotherapists, reported goals mainly related to body functions/structures.
The patients’ goals reflected the fact that they had reduced self-reported functioning, and a relatively low return to work rate of 23% at one year post-injury (22). Body functions/structures and activities that comprised 9% and 16%, respectively, of the patients’ 581 goals, corresponded to the lower scores for physical functioning, bodily pain and, to some extent, mental health. However, corresponding to the reduced social- and role-functioning, goals mainly describing participation socially, in work and leisure/recreation predominated. Other studies performed on patients’ goals in rehabilitation units showed a greater emphasis on activities of daily living than was found in our study (13, 16). According to Siegert & Taylor (1), after return home patients’ goals are likely to concern participation issues that depend on the personal and psychosocial context of the patients’ life. The present study supports this view because most patient goals concerned participation and quality of life issues.
The basis for goal setting in rehabilitation should concern the patients’ functional needs and their longer-term life goals. The rehabilitation professionals, the majority of whom were physiotherapists, presented a pattern in their goal descriptions that differed from the patients’, but that was in accordance with a physiotherapy focus (18). They focused on physical functioning, and to a lesser extent reported participation goals. However, patients with multiple injuries may face other challenges than physical ones in reaching participation goals such as returning to work (8, 22). Holliday et al. (2) found that a problem-oriented approach to goal setting was most commonly reported, and that the patients engaged in the goal setting process only to a limited degree. Physiotherapists rather than the patients supplied the target problems or abilities for which goals were set (17). Since the physiotherapists group was the majority one in the present study, these may be explanatory factors for the relatively dominating focus on body functions/structures. Other studies also found that descriptions of participation goals generally were sparse, and that, as in our study, a focus on body functions/structures and activities dominated (18).
Our study also sheds light on the structure and process that may explain some of the findings. For the majority of patients the rehabilitation involved a single professional, mainly physiotherapists. Thus, at the community level, there seemed to be a more traditional approach to rehabilitation consisting of fragmented services focusing on physical functioning, rather than having an approach based on a rehabilitation philosophy (12, 21). Even so, another study found that active involvement in the establishment of physiotherapy goals made the patients more likely to achieve their goals (15), indicating that a goal setting process would be required anyhow. In order better to address the patients’ psychosocial needs and goals, the participation of other professions or services would probably be required. In another article by the group, education and social functioning at return home, but not physical functioning, were among the significant predictors of return to work 2 years post-injury (22).
The professionals were to a larger extent more specific in their goal descriptions than the patients. Only 11% of the coded provider goals were categorized in one of the not definable ICF categories, as opposed to almost 40% of the patients’ goals. “Regaining my health” and “Getting back in shape” are examples of patients’ global expressions that may be converted into goals addressing body functions/structures or basic movement activities, hence reducing some of the discrepancy found in this study. Furthermore, some of the discrepancy may also be resolved in a goal setting process. However, little evidence has been found as to whether goal setting processes lead to improved outcomes (4). Thus, more research is needed to explore goal setting as a client-centred process and as a means for improving a wider perspective of rehabilitation outcomes.
The conceptual advances in rehabilitation do not appear to be well implemented into a goal setting practice in the municipalities for patients with multiple injuries. Goals such as work/education, social functioning and recreation should be considered on an equal level to that of physical functioning. Improved referral routines to the municipal rehabilitation services, increased understanding of rehabilitation as a multidisciplinary and multidimensional process, and improved goal setting procedures are considered necessary (1, 21). Moreover, there is a need for more research into the relationships between the process, structure and outcome in rehabilitation for severely injured patients (12, 19).
Strengths and limitations
The strength of this study is the representative sample of patients with severe multiple injuries that received rehabilitation in the community. The use of multiple methods enabled the goal perspectives of the patients and the providers, mainly physiotherapists, to be explored.
This study also has limitations. By excluding patients with pre-injury diagnoses of severe mental disorder or substance abuse, the generalizability of the study might be reduced. However, such problems might represent other challenges demanding rehabilitation services outside the scope of this study. Furthermore, a response shift may have influenced the patients’ self-reported functioning (34).
Some other methodological weaknesses should be mentioned. Firstly, interviews and questionnaires represent different methods and contexts that might have influenced the goal descriptions. Thus, the low agreement between patients and professionals should be interpreted with some caution, and this study may be considered more exploratory in nature. However, if an introduction stating the aims of rehabilitation was provided to the professionals, socially desirable responses might have biased the goal descriptions, hampering the validity of the text. Secondly, the patients may have communicated goals to the professionals that were in accordance with their preconception of rehabilitation and mainly physiotherapists’ qualifications. Nevertheless, it should be the professionals’ responsibility to discuss and set goals within a biopsychosocial perspective. Thirdly, the interviews were performed, goals written down (28) and analysed according to the ICF (11, 32) by HLS. Aspects of the interview content and the interviewer behaviour may have influenced the responses in the approximately 45-min interview. However, we aimed to collect and record the patients’ responses as precisely as possible and in a standardized manner across patients. Furthermore, it is a limitation that only a selection of the goals and the not definable codes were coded by and discussed with another allied health professional. Finally, a limitation is that only the main groups, covering 65% of the patients’ goal concepts, were tested for agreement.
In conclusion, this study of 66 patients with multiple injuries showed marked discrepancies between goals reported by the patients and the community rehabilitation providers. The patients’ goals mainly concerned activities and participation. The rehabilitation professionals, the majority of whom were physiotherapists, mainly reported goals related to body functions and activities (70%). The agreement between the patients’ and providers’ goals was poor, with kappa scores below 0.20. A statistical difference between patient and provider goals was demonstrated for musculoskeletal functions/structures, interpersonal interactions/relationships, work and recreation/leisure. The patients reported goals that may require effort from several professions and services. Our findings indicate a need for a multidisciplinary and biopsychosocial approach to the rehabilitation process.
Acknowledgements
The authors thank Professor Leiv Sandvik, Department of Epidemiology, Research Forum Ulleval University Hospital, for analytic assistance, and occupational therapist, Unni Sveen, PhD, for assistance in the ICF coding procedure.
This project was financed with the aid of EXTRA funds from the Norwegian Foundation for Health and Rehabilitation.
REFERENCES
1. Siegert RJ, Taylor WJ. Theoretical aspects of goal-setting and motivation in rehabilitation. Disabil Rehabil 2004; 26: 1–8.
2. Holliday RC, Antoun M, Playford ED. A survey of goal-setting methods used in rehabilitation. Neurorehabil Neural Repair 2005; 19: 227–231.
3. Wade DT. Evidence relating to goal planning in rehabilitation. Clin Rehabil 1998; 12: 273–275.
4. Levack WM, Taylor K, Siegert RJ, Dean SG, McPherson KM, Weatherall M. Is goal planning in rehabilitation effective? A systematic review. Clin Rehabil 2006; 20: 739–755.
5. Hurn J, Kneebone I, Cropley M. Goal setting as an outcome measure: a systematic review. Clin Rehabil 2006; 20: 756.
6. Anke AG, Stanghelle JK, Finset A, Roaldsen KS, Pillgram-Larsen J,
Fugl-Meyer AR. Long-term prevalence of impairments and disabilities after multiple trauma. J Trauma 1997; 42: 54–61.
7. Soberg HL, Bautz-Holter E, Roise O, Finset A. Long term multidimensional functional consequences of severe multiple injuries two years after trauma: a prospective longitudinal cohort study.
J Trauma 2007; 62: 461–470.
8. Holbrook TL, Anderson JP, Sieber WJ, Browner D, Hoyt DB. Outcome after major trauma: 12-month and 18-month follow-up results from the Trauma Recovery Project. J Trauma 1999; 46: 765–771.
9. MacKenzie EJ, McCarthy ML, Ditunno JF, Forrester-Staz C,
Gruen GS, Marion DW et al. Using the SF-36 for characterizing outcome after multiple trauma involving head injury. J Trauma 2002; 52: 527–534.
10. MacKenzie EJ, Morris JA, Jr, Jurkovich GJ, Yasui Y, Cushing BM,
Burgess AR, et al. Return to work following injury: the role of economic, social, and job-related factors. Am J Public Health 1998; 88: 1630–1637.
11. WHO. International classification of functioning, disability and health. Geneva: World Health Organization; 2001.
12. Wade DT, de Jong BA. Recent advances in rehabilitation. BMJ 2000; 320: 1385–1388.
13. Wressle E, Oberg B, Henriksson C. The rehabilitation process for the geriatric stroke patient –an exploratory study of goal setting and interventions. Disabil Rehabil 1999; 21: 80–87.
14. Bloom LF, Lapierre NM, Wilson KG, Curran D, DeForge DA, Blackmer J. Concordance in goal setting between patients with multiple sclerosis and their rehabilitation team. Am J Phys Med Rehabil 2006; 85: 807–813.
15. Arnetz JE, Almin I, Bergstrom K, Franzén Y, Nilssin H. Active patient involvement in the establishment of physical therapy goals: effects on treatment outcome and quality of care. Adv Physiother 2004; 6: 50–69.
16. Duff J, Evans MJ, Kennedy P. Goal planning: a retrospective audit of rehabilitation process and outcome. Clin Rehabil 2004; 18: 275–286.
17. Parry RH. Communication during goal-setting in physiotherapy treatment sessions. Clin Rehabil 2004; 18: 668–682.
18. Dekker J. Application of the ICIDH in survey research on rehabilitation: the emergence of the functional diagnosis. Disabil Rehabil 1995; 17: 195–201.
19. Hetherington H, Earlam RJ. Rehabilitation after injury and the need for coordination. Injury 1994; 25: 527–531.
20. Stucki G, Grimby G. Foreword: applying the ICF in medicine.
J Rehabil Med 2004; 36: 5–6.
21. Wade DT. Community rehabilitation, or rehabilitation in the community? Disabil Rehabil 2003; 25: 875–881.
22. Soberg HL, Finset A, Bautz-Holter E, Sandvik L, Roise O. Return to work after severe multiple injuries: a multidimensional approach on status 1 and 2 years postinjury. J Trauma 2007; 62: 471–481.
23. Osler T, Baker SP, Long W. A modification of the injury severity score that both improves accuracy and simplifies scoring. J Trauma 1997; 43: 922–925.
24. Association for the Advancement of Automotive Medicine. The Abbreviated Injury Scale 1990 Revision Update 98. Des Plaines, IL: Association for the Advancement of Automotive Medicine; 1998.
25. Prasad K. The Glasgow Coma Scale: a critical appraisal of its clinimetric properties. J Clin Epidemiol 1996; 49: 755–763.
26. Ware JE, Jr, Gandek B. Overview of the SF-36 Health Survey and the International Quality of Life Assessment (IQOLA) Project.
J Clin Epidemiol 1998; 51: 903–912.
27. Loge JH, Kaasa S. Short form 36 (SF-36) health survey: normative data from the general Norwegian population. Scand J Soc Med 1998; 26: 250–258.
28. Kvale S, editor. InterViews. 1996 edn. London: SAGE Publications; 2006.
29. Soberg HL, Sandvik L, Ostensjo S. Reliability and applicability of the ICF in coding problems, resources and goals of persons with multiple injuries. Disabil Rehabil 2008;.30: 98–106.
30. Cieza A, Stucki G. Content comparison of health-related quality of life (HRQOL) instruments based on the international classification of functioning, disability and health (ICF). Qual Life Res 2005; 14: 1225–1237.
31. Okochi J, Utsunomiya S, Takahashi T. Health measurement using the ICF: test-retest reliability study of ICF codes and qualifiers in geriatric care. Health Qual Life Outcomes 2005; 3: 46.
32. Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustrun TB, Stucki G. ICF linking rules: an update based on lessons learned. J Rehabil Med 2005; 37: 212–218.
33. Altman DG, editor. Practical statistics for medical research. 1st edn. London: Chapman & Hall; 1991.
34. Schwartz CE, Rapkin BD. Reconsidering the psychometrics of quality of life assessment in light of response shift and appraisal. Health Qual Life Outcomes 2004; 2: 16.