OBJECTIVE: To compare the effectiveness and safety of supervised aerobic exercise and home aerobic exercise in female Chinese patients with rheumatoid arthritis.
DESIGN: Single-blind randomized controlled trial.
SUBJECTS: Thirty female Chinese patients with rheumatoid arthritis were assigned to either supervised aerobic exercise or home aerobic exercise groups.
METHODS: The supervised aerobic exercise programme was supervised by a physical therapist, while the home aerobic exercise programme was performed at home after one session of exercise instruction. Each programme consisted of 1 h of aerobic exercise conducted 3 times per week for 8 weeks. Aerobic capacity and disease-related variables, including pain intensity, functional ability, psychological status and joint function, were measured.
RESULTS: Significant difference in changed score between pre- and post-exercise data was observed between the supervised aerobic exercise and home aerobic exercise groups regarding aerobic capacity (p < 0.0001). Pre- and post-exercise within-group comparisons showed significant improvement (20%) in aerobic capacity only in the supervised aerobic exercise group. Pre- and post-exercise within-group comparison showed significant improvement in 5 and 3 items of disease-related variables in supervised aerobic exercise and home aerobic exercise groups, respectively.
CONCLUSION: An 8-week supervised aerobic exercise programme induced significant improvement in the aerobic capacity of female Chinese patients with rheumatoid arthritis, and was superior to a home aerobic exercise programme. Both programmes of aerobic exercise were safe for female Chinese patients with rheumatoid arthritis.
Key words: exercise, rheumatoid arthritis, rehabilitation.
Correspondence address: Chih-Cheng Chuang, Department of Allergy, Immunology and Rheumatology, Shin Kong Wu Ho-Su Memorial Hospital, No. 95, Wen Chang Road, Shih Lin District, Taipei 111, Taiwan. E-mail: M001005@ms.skh.org.tw
J Rehabil Med 2009; 41: 332–337
Submitted February 20, 2008; accepted October 31, 2008
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, systemic, inflammatory autoimmune disease that causes symmetrical polyarthritis and a variety of extra-articular manifestations. Pain, stiffness and fatigue generally occur early in the course of RA. Reduction in physical function, such as range of motion (ROM), muscle strength, and aerobic capacity, may follow, and thus RA often leads to difficulty in activities of daily living (ADL) and poor quality of life (1). In previous studies, the aerobic capacity of patients with RA was found to be reduced by 20–30% (2), and the susceptibility to osteoporosis and cardiovascular disease was increased (3, 4). For these reasons, ROM exercise, strengthening programmes (isometric and isotonic) and aerobic exercise are recommended to maintain and promote joint mobility, muscle strength, and aerobic capacity.
Traditionally, it is suggested that excessive rhythmic dynamic exercise or any prolonged intensive exercise should be avoided in RA in order not to exacerbate joint symptoms, even though inflammation may be well controlled (5). However, this concept has been challenged by many authors. Since 1975 (6), a large number of studies have been conducted to investigate whether regular physical exercise programmes might be valuable in the management of RA. These studies are summarized in several reviews on exercise and RA (2, 7–9). The consensus in these reviews is that patients with RA show improved aerobic capacity, muscle strength, joint mobility, functional ability, and psychological status with exercise, without detrimental effects on disease activity and pain.
In designing an exercise programme, either supervised group exercise or home-based individual exercise has been used. Although aerobic exercise has been shown to be effective in promoting aerobic capacity and joint function in patients with RA, comparison of the effectiveness of supervised aerobic exercise (SAE) with home aerobic exercise (HAE) has rarely been investigated, and, as far as we know, has never been reported in the Chinese population. It has also never been proved whether Chinese patients with RA can improve their aerobic capacities after exercise like Western patients. Although previous reviews have shown that exercise could improve psychological status without causing pain in patients with RA (2, 7–9), we do not know whether it is the same in our population. The objectives of this study were therefore: (i) to compare levels of effectiveness between SAE and HAE in female Chinese patients with RA; and (ii) to determine if there was any adverse reaction after exercise.
METHODS
Participants
A total of 38 female patients with RA were recruited from 2 departments, Allergy-Immunology-Rheumatology and Physical Medicine & Rehabilitation, in a private teaching hospital and an RA aid group (a society organized by patients with RA in Taiwan). The eligibility criteria for entry into the study were: (i) age range 20–65 years; (ii) RA fulfilling the criteria from 1987 of the American College of Rheumatology (ACR) (formerly, the American Rheumatism Association) (10); (iii) disease lasting at least 6 months; and (iv) disease in well-controlled (stable) condition (no acute signs of inflammation). Exclusion criteria included: (i) arthroplasties or major operations in the knee or hip joints; (ii) presence of serious cardiac or pulmonary disease or any severe medical condition; and (iii) severe arthritis or contracture of knee joints precluding bicycle exercise testing. Prior to enrolment in the study, all participants signed a consent form approved by the hospital ethics committee.
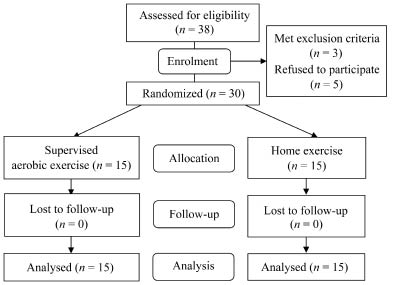
Of the first 38 volunteers with RA screened for this study, 2 had received total hip replacement, one had coronary artery disease, and another 5 declined to participate, so that a total of 30 patients were randomized to the 2 exercise groups. Randomization was performed by computer-generated random number. The allocation of the groups was initially concealed in an envelope, which was opened for each consecutive patient to reveal her group assignment at the time she was recruited into the study. A group of 15 participants (mean age 54.1 years, standard deviation (SD) 8.3 years) comprised the SAE group, and another 15 participants (mean age 51.2 years, SD 12.0 years) served as the HAE group. All 30 RA participants completed the study (Fig. 1).
Fig. 1. Consolidated Standards of Reporting Trials (CONSORT) flow-
chart for randomization procedure.
Twenty-three of the 30 patients reported their current occupation as home-maker, one as teacher and 6 as administrative staff. For recreational activities, 3 patients in the SAE group, and 2 in the HAE group reported taking regular exercise (meaning aerobic exercise lasting more than 30 min at least 2 times a week). Walking and swimming were the most common forms of exercise in all patients. Most participants were in ACR functional class II and were taking non-steroidal anti-inflammatory drugs (NSAIDs), remittive agents and low-dose prednisolone (5–10 mg) (Table I). Throughout the study, most subjects did not change their medications. There was no significant difference in the use or change of medications between the 2 groups. Comparisons of all baseline data between the SAE and HAE groups showed no significant difference except for body height (Table I).Exercise programmes
| Table I. Baseline data for supervised aerobic exercise (SAE) and home aerobic exercise (HAE) groups |
| | SAE group (n = 15) | HAE group (n = 15) | p-value |
| Age, years, mean (SD) | 54.1 (8.3) | 51.2 (12.0) | >0.05 |
| BW, kg, mean (SD) | 55.0 (6.1) | 58.0 (6.7) | >0.05 |
| BH, cm, mean (SD) | 153.8 (3.7) | 158.3 (5.2) | <0.05 |
| Duration of disease, years, mean (SD) | 8.2 (9.8) | 7.9 (4.7) | >0.05 |
| ACR functional class (II/III) | 14/1 | 14/1 | >0.05 |
| Participation in regular exercise, n | 3 | 2 | >0.05 |
| Medications, n | | | >0.05 |
| Prednisolone | 8 | 7 | |
| NSAID | 15 | 11 | |
| Remittive agent | 15 | 12 | |
| ESR, mm/h, mean (SD) | 50.0 (31.2) | 45.7 (31.4) | >0.05 |
| CRP, mg/dl, mean (SD) | 1.66 (2.35) | 1.55 (1.72) | >0.05 |
| RF, IU/ml, mean (SD) | 331.8 (1063.2) | 174.2 (194.0) | >0.05 |
| BW: body weight; BH: body height; ACR: American College of Rheumatology; NSAID: non-steroidal anti-inflammatory drug; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; RF: rheumatoid factor; IU: International Unit; SD: standard deviation. |
The SAE programme (8 weeks, 3 times per week) was conducted by a physical therapist in co-operation with a physiatrist who had much experience in arthritis rehabilitation. An exercise session comprised 10 min stretching exercise, 10 min warm-up with cycle ergometer, treadmill or other exercise machine, 30 min pool exercise in water of temperature 32–33ºC, and 10 min cooling down. In terms of intensity, the primary objective was to allow the subject to attain a target heart rate of 50–80% V.O2 peak (peak oxygen uptake) for at least 30 min in an exercise session. The V.O2 peak was determined by a graded exercise tolerance test, performed by each subject before the exercise programme. Each exercise group consisted of 7 or 8 RA participants.
Each participant in the HAE group was instructed once by a physical therapist about the performance of a home exercise programme consisting of 10 min stretching, 10 min warm-up, and 30 min aerobic exercise with walking, bicycling, aerobic dance, or swimming, and 10 min cooling down. The therapist demonstrated the technique of stretch exercise of the major muscles in the trunk, upper limbs and lower limbs. The therapist also discussed the choices and the progression of aerobic exercise with each patient. The target intensity during aerobic exercise was approximately 50–80% of V.O2 peak, which was also determined before the exercise programme. The target intensity was suggested to be maintained for at least 30 min in each exercise session, but multiple short bouts of exercise were allowed, e.g. 3 separate 10-min exercise sessions. Home exercise was continued for 8 weeks, 3 times per week. Participants were instructed in the use of daily training logs for self-monitoring of the duration, intensity and frequency of exercise. The physical therapist called each patient every 2 weeks and checked the exercise log at the end of the 8-week programme. Compliance of the participants was assessed by actual exercise frequency divided by the predicted frequency (i.e. 24 times).
Data collection
Background information. A self-report data form was given to all participants in both the SAE and HAE groups. This data form contained questions about age, gender, height, weight, symptom duration, physical activity level, occupational activities, recreational activities, medications and health history.
Exercise tolerance test. Open-circuit spirometry was used to measure the exercise tolerance of the subjects. The exercise tolerance test was performed on a bicycle ergometer with the participant in an upright position. Testing started with an initial load of 0 W, adding increments of 10–15 W/min until the appearance of symptoms or the participant’s request to stop. Systolic blood pressure (SBP) was monitored every 1 min. Electrocardiogram (ECG), heart rate (HR), and oxygen (O2) saturation were monitored continuously. A physiatrist was present during all testing. Expired gas was analysed by an automated system instrument (Vmax 29 Cardiopulmonary Exercise Testing Instrument, SensorMedics Corporation, Yorba Linda, CA, USA). Variables in the exercise tolerance test included HR, BP, oxygen uptake (V.O2), metabolic equivalent (MET), work, O2 pulse, and respiratory exchange ratio (RER) at peak cardiovascular response and at ventilatory threshold (VT). The primary outcome measure was V.O2 peak, which has been accepted as a criterion measure of aerobic capacity of a person (11).
Disease-related measures. Severity and extent of arthritis was assessed using the following measures: standardized joint examination, global pain intensity, ADL pain scale, grip strength, walking time, global self-assessment, global physician assessment, functional ability, psychological status, and laboratory tests. Changes in these measures could be regarded as secondary outcomes or adverse reactions due to exercise.
Total peripheral joint examination. The examination was performed by a rheumatologist, and the total number of swollen joints (0–54) and tender joints (0–56) were recorded.
Global pain intensity. It was assessed by visual analogue scale (VAS) for pain at the present time: a 10-cm horizontal line with the expressions “no pain at all” at the low end of the scale and “the most intense pain imaginable” at the high end.
ADL pain scale. The scale evaluates frequency (1–4, 1 = never, 4 = always) of pain experience in 8 activities of daily living (12). The total ADL score was the mean score for the 8 responses.
Grip strength. This was measured with a hand dynamometer in the dominant hand. The highest level of 3 trials was recorded.
Walking time. This was measured in seconds required to walk for 50 feet on an indoor course in a hallway as quickly as possible.
Global self-assessment. The assessment was evaluated by the subject herself about her overall condition, ranging from 0 to 10, indicating from the best (0) to the worst (10).
Global physician assessment. This was evaluated by a rheumatologist about his overall impression of the subject’s general condition, and also ranged from 0 to 10.
Health Assessment Questionnaire (HAQ) disability index. Functional ability was measured by HAQ disability index, which contains 20 questions that ask the respondent to report the degree of difficulty (0–3, 0 = no difficulty, 3 = unable to do) they have had in performing tasks in 8 functional domains in the past week (13).
Arthritis Impact Measurement Scales (AIMS). It is a multidimensional index (9 subscales) that measures the health status of subjects with arthritis (14). Because most subscales could be covered by previous measures, only the depression and anxiety components were recorded for measurement of the psychological status of the subjects.
Laboratory tests. C-reactive protein (mg/l), erythrocyte sedimentation rate (mm/h), and rheumatoid factor (international unit/ml) were measured for evaluation of disease activity.
Exercise tolerance test and all of the disease-related measures were performed twice, before and after 8-week exercise programmes in each subject. Throughout the study, the evaluators did not know the assigned group of each subject.
Data analysis
For demographic data, independent t-test or Mann-Whitney U-test (if distribution was non-normal) was used for continuous variables, and χ2 test or Fisher’s exact test was performed for categorical variables. For between-group comparison, independent-sample t-tests were conducted to investigate if there were any differences in the baseline data as well as the changed score between the baseline and the post-exercise data between the SAE and the HAE groups. When the assumption of normality or equality of variance was not met, Mann-Whitney U-test was performed instead. For within-group comparison, we used paired- sample t-test, or Wilcoxon signed-rank test if the assumption of normality was not met, to evaluate whether post-exercise data was significantly different from the baseline data in either the SAE or the HAE group. Based on 2 independent-sample groups (mean differences and their variances) with α = 0.05, 2 tails and sample size of each group being 15, powers were calculated. The power was sufficient for V.O2 peak (97.8%) and METpeak (peak MET response, 98.4%). Statistical analyses were performed using SPSS 15.0 for Windows. A value of p < 0.05 was used as an indicator of statistical significance.
RESULTS
The compliance with the exercise programme in the SAE group was 100%, while the HAE group had a mean compliance with exercise of 52% (SD 13), with a range of 32–75%.
For between-group comparison, there was no significant difference in the baseline data of exercise tolerance test between the SAE and HAE groups (Table II). For within-group comparison of variables of exercise tolerance test, significant improvement with regard to V.O2, MET, work, O2 pulse, and SBP at peak cardiovascular response and V.O2, MET at ventilatory threshold was found in the SAE group, but not in the HAE group (Table II). Statistically significant difference was observed for between-group comparison between the SAE and HAE groups with regard to changed score between the baseline data and the post-exercise data in V.O2, MET, work, O2 pulse, and SBP at peak cardiovascular response (Table II). Significantly statistical difference for between-group comparison was also detected in changed score of V.O2 and MET at ventilatory threshold. SAE induced mean improvements of 20%, 16% and 14% in V.O2 peak, peak workload, and O2 pulse, respectively.
| Table II. Comparison of the differences in the variables of exercise tolerance test between the baseline data and 8-week post-exercise data between supervised aerobic exercise (SAE) and home aerobic exercise (HAE) groups |
| Variables | SAE group (n = 15) | HAE group (n = 15) | p-value† |
| Baseline Mean (SD) | Post-exercise Mean (SD) | Baseline Mean (SD) | Post-exercise Mean (SD) |
| Resting state |
| HR, beats/min | 80.3 (17.6) | 80.7 (15.5) | 85.4 (18.0) | 82.9 (21.7) | >0.05 |
| SBP, mmHg | 134.7 (20.2) | 130.1 (22.7) | 126.9 (29.8) | 117.6 (16.1) | >0.05 |
| DBP, mmHg | 77.5 (9.2) | 74.4 (10.8) | 78.1 (12.2) | 72.9 (8.2)* | >0.05 |
| Peak response |
| V.O2, ml/kg/min | 14.6 (2.5) | 17.5 (3.2)* | 15.4 (4.0) | 14.5 (4.2) | <0.0001 |
| MET | 4.2 (0.7) | 5.0 (0.9)* | 4.4 (1.2) | 4.1 (1.2) | <0.0001 |
| Work, W | 85.1 (14.5) | 99.0 (20.2)* | 80.1 (21.0) | 82.3 (22.0) | <0.05 |
| O2 pulse, ml/beat | 5.6 (1.1) | 6.4 (1.3)* | 6.2 (1.6) | 5.9 (1.5) | <0.01 |
| HR, beats/min | 144.1 (17.2) | 150.3 (11.5)* | 144.4 (17.0) | 141.9 (15.9) | >0.05 |
| SBP, mmHg | 186.3 (22.4) | 199.9 (28.3)* | 175.7 (30.9) | 176.1 (28.4) | <0.05 |
| DBP, mmHg | 99.5 (18.8) | 92.5 (14.4) | 98.1 (14.2) | 90.6 (13.3)* | >0.05 |
| RER | 1.16 (0.10) | 1.14 (0.14) | 1.14 (0.06) | 1.13 (0.06) | >0.05 |
| Ventilatory threshold |
| V.O2, ml/kg/min | 9.4 (1.8) | 10.7 (1.9)* | 9.5 (3.9) | 8.9 (2.8) | <0.05 |
| MET | 2.7 (0.5) | 3.1 (0.5)* | 2.7 (1.1) | 2.5 (0.8) | <0.05 |
| Work, W | 46.8 (19.4) | 53.3 (19.6) | 47.4 (19.3) | 45.1 (14.0) | >0.05 |
| HR, beats/min | 114.2 (13.3) | 115.7 (14.6) | 120.2 (15.7) | 113.6 (16.6) | >0.05 |
| *p < 0.05 by paired-sample t-test or Wilcoxon signed-rank test for within-group comparison between the baseline data and post-exercise data. †p < 0.05 by independent-sample t-test or Mann-Whitney U-test for between-group comparison in changed score between the baseline data and post-exercise data. No significant statistical difference in baseline data for group-comparison between SAE and HAE groups was observed (by independent-sample t-test or Mann-Whitney U-test). HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; V.O2: oxygen uptake; MET: metabolic equivalent; RER: respiratory exchange ratio; SD: standard deviation. |
For all of the disease-related measures shown in Table III, there was no significant difference in baseline data between the SAE and HAE groups except for global self-assessment and global physician assessment. For within-group comparison, significant improvement after exercise was observed in global pain intensity, ADL pain scale, grip strength, walking time, and global self-assessment in the SAE group (p < 0.05). For the HAE group, there was significant exercise effect in global pain intensity, ADL pain scale, and walking time (p < 0.05). There were no significant within-group changes between baseline data and post-exercise data for number of swollen joints, number of tender joints, HAQ, AIMS-depression, AIMS-anxiety, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and rheumatoid factor (RF) in either the SAE group or the HAE group (p > 0.05). For all of the disease-related measures, there was no significant between-group difference regarding changed score between the baseline data and the post-exercise data.
DISCUSSION
Although exercise in patients with RA has been reported previously in Western countries (2, 6–9), this study is the first report on exercise in female Chinese patients with RA. Our study proved that the SAE programme was superior to the HAE programme with regard to improvement in the aerobic capacity of patients with RA. The mean baseline V.O2 peak in female Chinese patients with RA was about 15 ml/kg/min, and the mean baseline work was about 82.5 W (Table II); both data reflected a low level of aerobic capacity comparing with 22.0 ml/kg/min and 162 W reported in Western countries (15, 16). However, after an 8-week exercise, subjects in the SAE group had improved their aerobic capacity by approximately 20%. In previous reports, mean improvement of V.O2 peak after a conventional exercise programme (6–12 weeks, 3 times/week) usually reached 15–25% of pre-exercise value (6, 17–20). Our findings were consistent with those for the Western populations reported by previous studies.
Although between-group comparison showed no significant difference in changed score between baseline data and post-exercise data in all disease-related measures (Table III), significant within-group differences between baseline data and post-exercise data were found more in the SAE group than in the HAE group (5 items vs 3 items). The findings might also suggest that the SAE group had a better exercise effect than the HAE group.
In this study, the HAE group did not show an increment in V.O2 peak. Although RA patients in the HAE group were instructed about the exercise programme, the compliance with exercise was low (52%), and the target exercise intensity may not have been reached, which might explain the lack of V.O2 peak increase in the HAE group. On the contrary, the SAE programme provided recreation, the chance for socialization, and good-quality equipment for exercise (pools, treadmills, bicycles, and other exercise machines), all of which contributed toward a 100% compliance rate in the SAE group. Previous studies showed compliance for most organized exercise programmes are approximately 50% (or 39–65%) within 3–6 months, but could be over 90% (21–23); for home-based exercise, the compliance is variable, from 30% to 98% (24, 25). Factors favouring good compliance have been reported previously (25, 26). Although compliance in the HAE group was lower than that in the SAE group, the compliance of either group was compatible with the previous reports (21–25). In our study, if we could provide a better education programme and a better supervision system (e.g. more frequent telephone calls or using a computer control system), the compliance of the HAE group would be increased.
The safety of aerobic exercise and strengthening exercise in patients with RA has been reviewed previously (7, 27, 28). Most studies reported no change in disease-related measures. A few studies showed some decreases in disease activities measured by erythrocyte sedimentation rate, joint count and pain. De Jong et al. (29) also demonstrated no progression of radiological joint damage of the hands and feet in patients with RA by long-term high-intensity weight-bearing exercise.
However, in another study by the same authors, significantly more progression in large joint (especially shoulder and subtalar joints) damage after a long period of intensive exercise was shown in patients with greater baseline radiological damage (15).
In our study both the SAE and HAE groups showed no significant within-group change after exercise in the number of swollen joints, number of tender joints, HAQ, AIMS-depression, AIMS-anxiety, erythrocyte sedimentation rate, C-reactive protein and rheumatoid factor (Table III), which may also indicate that both exercise programmes were safe for patients with RA. The reason may be both the SAE and HAE programmes were low-impact aerobic exercise, and the patients recruited were in a stable condition without severe involvement of joints in the lower extremities. However, lack of change in HAQ, AIMS, etc. after exercise could be due to poor validity of the measurements, or to a “ceiling effect” artefact in the mildly disabled patients (27, 29, 30). The second reason may be short duration of intervention. If the exercise programme could be extended to 12 weeks or more, it might be able to detect the change in disease-related variables. Another possible reason may be small sample size. The statistical powers of HAQ and AIMS-depression were 10.2% and 5.17%, respectively, so type II error probably existed.
| Table III. Comparison of the differences in the disease-related measures between the baseline data and 8-week post-exercise data for both supervised aerobic exercise (SAE) and home aerobic exercise (HAE) groups |
| Variables | SAE group (n = 15) | HAE group (n = 15) | p-value‡ |
| Baseline Mean (SD) | Post-exercise Mean (SD) | Baseline Mean (SD) | Post-exercise Mean (SD) |
| No. of swollen joints (0–54) | 9.07 (10.40) | 8.40 (9.93) | 7.00 (4.42) | 6.13 (4.52) | >0.05 |
| No. of tender joints (0–56) | 16.80 (15.77) | 16.73 (15.91) | 14.87 (9.75) | 13.53 (9.46) | >0.05 |
| Pain (0–10) | 3.60 (1.88) | 2.70 (2.14)* | 2.70 (2.14) | 1.79 (2.42)* | >0.05 |
| Pain-ADL (0–3) | 0.96 (0.66) | 0.72 (0.58)* | 1.19 (0.57) | 0.84 (0.75)* | >0.05 |
| Grip strength, kg | 10.46 (2.66) | 12.00 (3.70)* | 12.27 (4.93) | 13.70 (5.37) | >0.05 |
| Walking time, sec | 12.47 (2.66) | 11.58 (2.17)* | 11.87 (2.11) | 10.90 (1.86)* | >0.05 |
| Global self-assessment (0–10) | 4.01 (1.90) | 2.67 (2.06)* | 2.44 (2.28)† | 1.47 (1.82) | >0.05 |
| Global physician assessment (0–10) | 2.75 (1.10) | 2.29 (0.95) | 1.71 (0.72)† | 1.53 (0.61) | >0.05 |
| HAQ (0–3) | 0.44 (0.42) | 0.36 (0.31) | 0.41 (0.37) | 0.32 (0.27) | >0.05 |
| AIMS-depression (1–6) | 1.73 (1.03) | 1.73 (1.10) | 1.67 (1.05) | 1.60 (1.12) | >0.05 |
| AIMS-anxiety (1–6) | 2.40 (1.72) | 2.07 (1.03) | 2.13 (1.30) | 1.93 (1.10) | >0.05 |
| ESR, mm/h | 50.00 (31.20) | 53.20 (30.60) | 45.70 (31.40) | 40.70 (31.20) | >0.05 |
| CRP, mg/dl | 1.66 (2.35) | 1.70 (2.71) | 1.55 (1.72) | 1.50 (1.80) | >0.05 |
| RF, IU/ml | 332 (1063) | 268 (887) | 174 (194) | 185 (368) | >0.05 |
| *p < 0.05 by paired-sample t-test or Wilcoxon signed-rank test for within-group comparison between the baseline data and post-exercise data. †p < 0.05 by independent-sample t-test or Mann-Whitney U-test for between-group comparison in the baseline data. ‡p < 0.05 by independent-sample t-test or Mann-Whitney U-test for between-group comparison in changed score between the baseline data and post-exercise data. Pain-ADL: pain in activities of daily living; HAQ: health assessment questionnaire; AIMS-depression: depression component of the Arthritis Impact Measure Scale; AIMS-anxiety: anxiety component of the Arthritis Impact Measure Scale; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; RF: rheumatoid factor; IU: International Unit; SD: standard deviation. |
Study limitations
Some limitations were, however, inherent in our study. First, the compliance of the participants in the HAE group was not controlled well to eliminate its influence on exercise effects. Secondly, the sample size of 15 in each group was relatively small, and the statistical powers for HAQ and AIMS-depression were low. More cases are needed for evaluation of change of functional ability and psychological status. Thirdly, we recruited females only for convenience of group exercise, so the results of our study may not be applicable to male subjects. Finally, the present study does not provide information on the long-term outcome of aerobic exercise, and thus we do not know if the exercise effects would be maintained or if side-effects would present after a long exercise programme. Despite the above limitations, our findings provide some evidence in favour of the SAE programme in female Chinese patients with RA.
In conclusion, our results showed that although female Chinese patients with RA had low V.O2 peak values, they could perform exercise to improve aerobic capacity without experiencing exacerbation of pain intensity, joint function, functional ability, psychological status, and other disease-related measures. Our findings also demonstrated that supervised aerobic exercise showed a good compliance and induced a significant improvement (20%) in aerobic capacity in patients with RA and was superior to home exercise.
ACKNOWLEDGEMENTS
This work was supported by grants from the Taiwan National Science Council and the Shin Kong Wu Ho-Su Memorial Hospital & Taipei Medical University. The authors acknowledge Professor Chang-Zern Hong for manuscript revision, Professor Yeh Ching-Ying, Miss Chyi-Huey Bai, Miss Hsin-Yi Lee for statistics assistance, and the kind co-operation of Mr Polin Wu, Miss Hui-Lien Chien, Miss Shu-Min Lin, Miss Pei-Hua Chen and co-workers in the Shin Kong Wu Ho-Su Memorial Hospital.
REFERENCES
1. Minor MA. Cardiovascular health and physical fitness for the client with multiple joint involvement. In: Walker JM, Helewa A, editors. Physical therapy in arthritis. 1st edn. Philadelphia: WB Saunders; 1996, p. 191–209.
2. Stenström CH, Minor MA. Evidence for the benefit of aerobic and strengthening exercise in rheumatoid arthritis. Arthritis Rheum (Arthritis Care Res) 2003; 49: 428–434.
3. Haugeberg G, Orstavik RE, Uhlig T, Falch JA, Halse JI, Kvien TK. Bone loss in patients with rheumatoid arthritis: results from a population-based cohort of 366 patients followed up for 2 years. Arthritis Rheum 2002; 46: 1720–1728.
4. Turesson C, Jarenros A, Jacobson L. Increased incidence of cardiovascular disease in patients with rheumatoid arthritis: results from a community-based study. Ann Rheum Dis 2004; 63: 952–955.
5. Gerber NL. Rehabilitation of patients with rheumatic disease. In: Kelley WN, Harris ED, Ruddy S, editors. Textbook of rheumatology. 1st edn. Philadelphia: WB Saunders; 1981, p. 1858–1859.
6. Ekblom B, Lövgren O, Alderin M, Fridström M, Satterström G. Effect of short-term physical training on patients with rheumatoid arthritis: a six-month follow-up. Scan J Rheumatol 1975; 4: 87–91.
7. de Jong Z, Vliet Vlieland TPM. Safety of exercise in patients with rheumatoid arthritis. Current Opin Rheumatol 2005; 17: 177–182.
8. Kettunen JA, Kujala UM. Exercise therapy for people with rheumatoid arthritis and osteoarthritis. Scan J Med Sci Sports 2004; 14: 138–142.
9. Van den Ende CHM, Vliet Vlieland TPM, Munneke M, Hazes JM. Dynamic exercise for treating patients with rheumatoid arthritis. Cochrane Database of Systemic Reviews. 2008; 1: CD000322.
10. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, et al. The American Rheumatism Association 1987: revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988; 31: 315–324.
11. American College of Sports Medicine. Guidelines for exercise testing and prescription. 7th edn. Philadelphia: Lippincott, Williams & Wilkins; 2005, p. 66.
12. Callahan LF, Brooks RH, Summey JA, Pincus T. Quantitative pain assessment for routine care of rheumatoid arthritis patients, using a pain scale based on activities of daily living and a visual analog pain scale. Arthritis Rheum 1987; 30: 630–636.
13. Fries JF, Spitz PW, Kraines RG, Holman HR. Measurement of patient outcome in arthritis. Arthritis Rheum 1980; 23: 137–145.
14. Meehan RF, Gertman PM, Mason JH. Measuring health status in arthritis: the arthritis impact measurement scales. Arthritis Rheum 1980; 23: 146–152.
15. Munneke M, de Jong Z, Zwinderman AH, Ronday KH, van Schaardenburg D, Dijkmans BA, et al. Effect of a high-intensity weight-bearing exercise program on radiologic damage progression of the large joints in subgroups of patients with rheumatoid arthritis. Arthritis Rheum 2005; 53: 410–417.
16. Minor MA, Hewett JE. Physical fitness and work capacity in women with rheumatoid arthritis. Arthritis Care Res 1995; 8: 146–154.
17. Lyngberg KK, Harreby M, Bentzen H, Frost B, Danneskiold-Samsøe B. Elderly rheumatoid arthritis patients on steroid treatment tolerate physical training without an increase in disease activity. Arch Phys Med Rehabil 1994; 75: 1189–1195.
18. Baslund B, Lyngberg KK, Anderson V, Halkjaer Kristensen J, Hansen M, Klokker M, et al. Effect of 8 weeks of bicycle training on the immune system of patients with rheumatoid arthritis. J Appl Physiol 1993; 75: 1691–1695.
19. Harkcom TM, Lampman RM, Banwell BF, Castor CW. Therapeutic value of graded aerobic exercise training in rheumatoid arthritis. Arthritis Rheum 1985; 28: 32–39.
20. Davis JA, Frank MH, Whipp BJ, Wasserman K. Anaerobic threshold alterations caused by endurance training in middle-aged men. J Appl Physiol 1979; 46: 1039–1046.
21. Häkkinen A, Sokka T, Hannonen P. A home-based two-year strength training period in early rheumatoid arthritis led to good long-term compliance: a five-year follow-up. Arthritis Rheum 2004; 51: 56–62.
22. Moff H, Noreau L, Parent E, Drolet M. Feasibility of an eight-week dance-based exercise program and its effects on locomotor ability of persons with functional class III rheumatoid arthritis. Arthritis Care Res 2000; 13: 100–111.
23. Bradley LA. Adherence with treatment regimens among adult rheumatoid arthritis patients: current status and future directions. Arthritis Care Res 1989; Suppl 2: S33–S39.
24. Mayoux-Benhamou A, Giraudet-Le Quintrec JS, Ravaud P, Champion K, Dernis E, Zerkak D, et al. Influence of patient education on exercise compliance in rheumatoid arthritis: a prospective 12-month randomized controlled trial. J Rheumatol 2008; 35: 216–223.
25. Stenström CH. Home exercise in rheumatoid arthritis functional class II: goal setting versus pain attention. J Rheumatol 1994; 21; 627–634.
26. American College of Sports Medicine. Guidelines for exercise testing and prescription. 7th ed. Philadelphia: Lippincott, Williams & Wilkins; 2005, p. 167.
27. Van den Ende CHM, Vlift Vlieland TPM, Munneke M, Hazes JMW. Dynamic exercise therapy in rheumatoid arthritis: a systematic review. Br J Rheumtol 1998; 37: 677–687.
28. Häkkinen A. Effectiveness and safety of strength training in rheumatoid arthritis. Curr Opin Rheumatol 2004; 16: 132–137.
29. de Jong Z, Munneke M, Zwinderman AH, Kroon HM, Ronday KH, Lems WF, et al. Long-term high-intensity exercise and damage of small joints in rheumatoid arthritis. Ann Rheum Dis 2004; 63: 1399–1405.
30. Gardiner PV, Sykes HR, Hassey GA, Walker DJ. An evaluation of the health assessment questionnaire in long-term longitudinal follow-up of disability in rheumatoid arthritis. Br J Rheumatol 1993; 32: 724–728.