OBJECTIVE: To investigate the associations between smoking and alcohol consumption, and long-term sick leave due to unspecific back or neck pain among employees in the public sector.
DESIGN: A 3-year prospective cohort study.
SUBJECTS: Approximately 9000 persons in the public sector in Sweden were invited to participate. Of these, 7533 answered a questionnaire and 6532 were included in the study, classified as having “good health for working”.
METHODS: New periods of sick leave > 28 days were consecutively reported from the employers or the occupational health service during a period of 3 years. Rate ratios were estimated by means of Cox proportional hazard regression model.
RESULTS: Smoking was associated with an increased risk of long-term sick leave due to unspecific back or neck pain. Compared with people who have never smoked, “ever smokers” had a higher risk (rate ratio = 1.8, 95% confidence interval: 1.3–2.4). Alcohol consumption tended to be associated with a decreased risk, but the results were not statistically significant.
CONCLUSION: Our results suggest that smoking is a risk factor for long-term sick leave due to unspecific back or neck pain. Moderate alcohol consumption tends to have a protective effect, at least among women in the public sector.
Key words: sick leave, back pain, neck pain, lifestyle, public sector.
J Rehabil Med 2009; 41: 550–556
Correspondence address: Eva Skillgate, Institute of Environmental Medicine, Karolinska Institutet, Box 210, SE-171 77 Stockholm, Sweden. E-mail: eva.skillgate@ki.se
Submitted February 7, 2008; accepted February 20, 2009
INTRODUCTION
Musculoskeletal pain, especially in the back and neck, is common and constitutes the main cause of persistent pain in the Swedish population (1, 2). Musculoskeletal complaints are also the main cause of sick leave and, since back or neck diagnoses comprise a large part of this group, they are of particular interest (3). A systematic review entitled “Sickness absence – causes, consequences and physicians’ sickness certification practice” was published in 2004 by the Swedish Council on Technology Assessment in Health Care (SBU) (4). The editors established that knowledge about the causes and consequences of sick leave was limited (5). The need to identify risk factors for long-term sick leave, in order to make effective prevention strategies, was stated in the report. Evidence about the risk factors for sick leave attributed to back and neck disorders often focuses on work factors (6). However, since the aetiology of sickness absence is multifactorial, it is also important to investigate other factors, such as smoking and alcohol consumption. Five studies of the impact of smoking on long-term sick leave due to back or neck pain met the quality standards for inclusion in the SBU-Review: 2 of medium (7, 8) and 3 of low quality (9–11). No study on the impact of alcohol consumption was included. In summary, smoking was not found to significantly increase the risk for sick leave due to back disorders (3). The need for more high-quality research on risk factors for sick leave due to back and neck pain, especially concerning women and the impact of lifestyle factors, was stated (5).
Some more recent studies have been published on the associations between smoking and alcohol consumption, respectively, and sick leave. Concerning smoking, 3 studies found a higher risk of sick leave due back pain (12–14). Some studies have found smoking to be associated with long-term sick leave regardless of diagnosis (15–17), and in one study smoking was found to be a predictor for long-term work disability among physically inactive persons (18). In summary, these studies suggest that smoking is a risk factor for sick leave due to back pain. Concerning the effect of alcohol consumption, some Swedish studies found that high alcohol consumption was related to an increase in sickness absence of any kind (19, 20) and one found no association between alcohol consumption and sickness absence (17).
Aim
The aim of this study was to investigate the associations between smoking and alcohol consumption, respectively, and long-term sick leave due unspecific back or neck pain among employees in the public sector.
METHODS
This cohort study was performed within the longitudinal study “Work and health in the public sector in Sweden” the HAKuL study, that was launched in 1999–2000 in 4 county councils and in local authorities in 6 municipalities, located in the southern, the middle and the northern parts of Sweden. In total approximately 9000 employees, not sick listed for more than 3 months in a row at baseline, were asked to participate. The main occupational groups in the study population were registered nurses, assistant nurses, home-based personal care workers in elderly care, employees at child care centres, administrative personnel, and teachers. In this study the term long-term sick leave was used to describe continuous absenteeism from work due to unspecific pain in the back or neck for ≥ 28 days in a row. All new spells of long-term sick leave periods were consecutively reported by the employer or the occupational health service during a period of 3 years from baseline. During the 3-year follow-up 177 persons had at least one spell of continuous sick leave due to back or neck pain for 28 days or more.
The study started with an extensive baseline questionnaire including questions on social situation, health, lifestyle and work factors. The questionnaire was distributed at the workplace or by normal post. Details of the assessment parameters are described elsewhere (15). The questions on alcohol and smoking used for this study are shown in Table I. The alcohol questions are derived from the AUDIT-questionnaire (21). The lifestyle part of the questionnaire also included questions on physical exercise habits, weight and height.
| Table I. Questions about alcohol consumption and smoking in the baseline questionnaire, and the distribution of the answers among all subjects in the cohort (n = 6532), and among cases (n = 177) |
| Questions | All, % (n) | Cases, % (n) |
| How often do you drink alcohol? (99% of responding subjects answered this question) |
| Never | 8 (508) | 13 (22) |
| Once per month or less often | 33 (2119) | 41 (71) |
| 2–4 times per month | 46 (3014) | 40 (69) |
| 2–3 times per week | 12 (746) | 6 (10) |
| 4 times per week or more often | 1 (88) | – |
| How many “drinks”* do you have on a typical day when you drink alcohol? (92% of responding subjects answered this question) |
| 1–2 | 60 (3584) | 59 (89) |
| 3–4 | 30 (1831) | 31 (47) |
| 5–6 | 7 (432) | 6 (9) |
| 7–9 | 2 (100) | 2 (3) |
| 10 or more | 1 (39) | 2 (2) |
| Do you smoke? (98% of responding subjects answered this question) |
| Yes, I am a daily smoker | 19 (1198) | 31 (53) |
| Yes, I smoke sometimes | 7 (480) | 7 (12) |
| No, I have stopped smoking during the last year | 2 (164) | 3 (5) |
| No, I have not smoked during the last year | 24 (1529) | 27 (48) |
| No, I have never been a smoker | 48 (3081) | 32 (55) |
| If yes, how many cigarettes per day on average? (96% of responding subjects who were current smokers answered this question) |
| 1–2 | 12 (194) | 11 (7) |
| 3–9 | 24 (387) | 14 (9) |
| 10–20 | 62 (934) | 73 (46) |
| > 20 | 2 (37) | 2 (1) |
| If yes, how many years have you been smoking in total? (98% of responding subjects who were current smokers answered this question) |
| 0–5 | 8 (132) | 2 (1) |
| 6–10 | 12 (206) | 9 (5) |
| 11–20 | 30 (483) | 26 (15) |
| 21–30 | 33 (533) | 45 (26) |
| > 30 | 17 (284) | 18 (10) |
| *Examples of “drinks”: 1 bottle of medium strong beer, 1/2 bottle of strong beer, 1 glass of wine, 1 small glass of dessert wine, 4–6 cl of spirits. |
With regard to smoking habits, subjects were classified into never smokers (people who reported that they had never smoked), ever smokers (daily smokers, those who sometimes smoke and those who had stopped smoking), ex-smokers (those who had stopped smoking) and current smokers. For current smokers, the amount of smoking was calculated and expressed as pack years. One pack year was regarded as the equivalent of, for example, 20 cigarettes smoked per day for one year or 10 cigarettes smoked per day for 2 years, etc. With regard to alcohol consumption, subjects were classified into different categories according to reported frequency and amount of alcohol consumption. By multiplying the frequency by the amount of alcohol consumption, the number of drinks per month was obtained. These values were classified into quartiles according to the distribution among the study subjects.
Health-related questions from the Nordic Questionnaire (22), the 36-Item Short Form Health Survey (SF-36) (23), and questions on sickness presenteeism (24) were included in the questionnaire. Physical and mental demands at work, related to the individual’s own capacity, were measured by questions from the Work Ability Index (WAI) Questionnaire (25). Socio-economic class was assessed by occupational grade, classified according to the International Standard Classification of Occupations (ISCO-88).
To be included in the present study, a subject was required to have “good health for working”, as defined by using a previously developed index (15), based on a combination of answers to questions on general health from the SF-36 health survey (23) and the answer to a question from the WAI Questionnaire (25). Those subjects with bad general health (a score ≤ 64 on the SF-36 general health scale) and who on the WAI Questionnaire reported it to be “unlikely” or “not certain” that they could continue their work for another 2 years, with regard to perceived health status, were classified as having “bad health for working”. These subjects were excluded from the analyses (n = 911), as were those who were on full-time sick leave for any reason on the day they answered the questionnaire (n = 90).
Statistical analysis
In the analyses different categories of smokers were compared with never smokers, and different categories of alcohol drinkers were compared with subjects reporting low alcohol consumption. Hazard ratios (denoted as rate ratios (RR)) regarding risk of a first spell of long-term sick leave due to unspecific back or neck pain associated with smoking or alcohol consumption, respectively, were calculated by means of Cox proportional hazard regression model, together with 95% confidence intervals (CI). Person time was calculated from inclusion to the day of the first sick leave period of > 28 days for any reason, to the day of leaving the employment, or to the end of follow-up, whichever occurred first. The exact leaving day was known for 25% of those leaving their job. Those with unknown leaving date and those leaving the job between baseline and 18-month follow-up were given 9 months of person time and those leaving the job between 18 and 36 months follow-up were given 27 months of person time. Potential confounding factors assessed at baseline were introduced in the model, one at a time, and the amount of change in the coefficient of the exposure term was examined. If it altered by approximately 10% or more, the factor was considered a confounder and added to the regression model (26). Hazard ratios for smoking or alcohol consumption (in the same regression model) were adjusted for the following confounding factors: pain (much or very much pain/not much pain), socio-economic class (stratified into 3 skill levels, occupations requiring at least 3–4 years education after high school, skilled workers with vocational education and unskilled workers), and age (continuous). In addition the following factors were considered with regard to potential confounding (dichotomized): sex, living alone (with or without children), born abroad, low education, poor financial situation, pain from back or neck (22), health-related quality of life (23), at least one day of sick leave for any reason at least once during the preceding 12 months, sickness presenteeism for any reason at least once during the preceding 12 months (24), burn-out syndrome (27), sense of coherence (28), high demands and low control at work (job strain) (29), physically demanding work, no physical exercise, bad sleep and recuperation, high body mass index, snuff use, and geographical area. None of these confounded the relationship between alcohol and smoking, respectively, and sick leave; thus they were not included in the final model.
Assumption of proportional hazards for the exposures and confounding factors were examined by the method of Shoenfeldt’s partial residuals; there was no indication of violation of the assumption for any of the variables included in the regression models (30). Trend test for a dose-response relationship was performed by using the exposure classified in 4 categories in a Cox proportional hazard regression model (31). The correlation between smoking and alcohol consumption was assessed with Spearman’s rank correlation coefficient.
All calculations were performed using the statistical programme Intercooled STATA 9.
The study was approved by the ethics committee of the Karolinska Institute, Sweden.
RESULTS
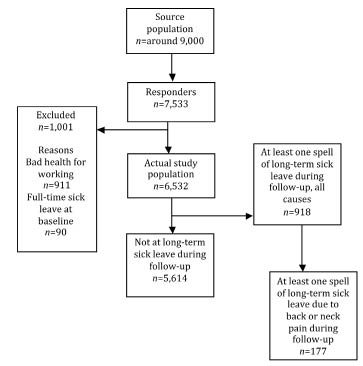
In total, 7533 out of 9000 men and women answered the questionnaire (84% response rate), and 6532 were included in the cohort, classified as having “good health for working” at baseline, and to be at risk for becoming long-term sick listed (not sick listed at baseline). Table I shows the distribution of answers to the questions about smoking and alcohol consumption in the cohort. Table II describes the characteristics of the participants in the cohort. Of the included persons, 82% were women and the mean age was 45 years. During the 3-year follow-up, 177 persons had at least one spell of continuous sick leave for ≥ 28 days due to back or neck pain (Fig. 1).
| Table II. Characteristics of the participants in the actual study population |
| Characteristics | All (n = 6532) | Never smokers* (n = 3081) | Ever smokers† (n = 3371) | Never/Seldom alcohol‡ (n = 2627) | Alcohol users§ (n = 3848) | Cases of long-term sick leave (n = 177) |
| Women, % | 82 | 83 | 82 | 88 | 78 | 93 |
| Age, mean (SD) | 45 (10) | 44 (10) | 47 (9) | 45 (11) | 46 (10) | 48 (9) |
| Low education, % | 21 | 18 | 24 | 24 | 17 | 21 |
| Strained financial situation, % | 16 | 12 | 19 | 20 | 13 | 18 |
| Low socioeconomic class,% | 39 | 34 | 44 | 53 | 30 | 69 |
| Obese, % | 9 | 9 | 9 | 12 | 7 | 16 |
| Body mass index, mean (SD) | 25 (4) | 25 (4) | 25 (4) | 25 (5) | 25 (4) | 26 (4) |
| Daily smoking, % | 19 | – | – | 20 | 18 | 30 |
| Never or rarely drinking alcohol, % | 41 | 15 | 19 | – | – | 54 |
| Never exercising, % | 15 | 12 | 17 | 17 | 13 | 11 |
| Sick leave for any reason at least once the preceding 12 months, % | 60 | 59 | 61 | 59 | 60 | 74 |
| Sickness presenteeism at least once in the preceding 12 months, % | 74 | 72 | 76 | 72 | 76 | 86 |
| Bad general health (SF-36), % | 15 | 12 | 17 | 17 | 13 | 27 |
| Much or very much pain (SF-36), % | 20 | 17 | 22 | 22 | 18 | 40 |
| Pain or trouble from 5 body regions or more, % | 24 | 21 | 27 | 25 | 23 | 45 |
| Pain or trouble from neck, shoulder or upper back, % | 19 | 17 | 21 | 20 | 19 | 32 |
| Pain or trouble from lower back, % | 54 | 50 | 57 | 55 | 53 | 71 |
| Pain or trouble from neck, shoulder, upper back and lower back, % | 14 | 12 | 16 | 15 | 14 | 25 |
| *People who have never smoked. †Daily smokers, those who sometimes smoke and those who have stopped smoking. ‡People who drink alcohol once per month or less often. §People who drink alcohol twice per month or more often. SD: standard deviation; SF-36: 36-Item Short Form Health Survey. |
Fig. 1. Inclusion process and progress of subjects through the study.
Long-term sick leave due to back or neck pain was most common among assistant nurses and nursing assistants/medical orderlies. In these groups 5% had at least one spell of long-term sick leave due to back or neck pain in the 3-year follow-up period.
Smoking was associated with an increased risk of sick-leave due to unspecific back or neck pain (Table III). Compared with never smokers, the adjusted RR for ever smokers was 1.8 (95% CI: 1.3–2.4) and for persons with more than 20 pack years 2.2 (95% CI: 1.2–3.9). There was no significant dose-response relationship regarding smoking expressed as pack years and long-term sick leave due to unspecific back or neck pain (p = 0.08).
Alcohol consumption tended to have a protective effect against long-term sick leave due to unspecific back or neck pain, but the results were not statistically significant (Table IV). Participants who drank alcohol twice per week or more often had a lower risk than those who drank once per month or less often (RR = 0.4, 95% CI: 0.1–1.1). Consuming more than 10 drinks per month compared with consuming fewer than 2 drinks per month associated with a lower risk (RR = 0.5, 95% CI: 0.2–1.2). Compared only with never drinkers (people who never drink alcohol), alcohol users had a lower risk (RR = 0.6, 95% CI: 0.3–1.0) (not shown in Table IV). There was a dose-response relationship regarding alcohol consumption, expressed as drinks/month and long-term sick leave due to back or neck pain (p = 0.04).
| Table III. Rate ratios (RR) of long-term sick leave due to back or neck pain associated with different amounts of smoking, together with 95% confidence interval (95% CI) |
| Smoking exposures | Exposed cases♦ (n) | Exposed non-cases (n) | RR† (95% CI) | RR‡ (95% CI)* |
| Never smokers§ | 55 | 3026 | 1.0 | 1.0 |
| Ever smokers¶ | 118 | 3253 | 2.0 (1.5–2.8) | 1.8 (1.3–2.4) |
| Ex-smokersº | 53 | 1640 | 1.8 (1.2–2.6) | 1.8 (1.2–2.6) |
| Current smokers all◊ | 65 | 1613 | 2.2 (1.6–3.2) | 1.8 (1.2–2.6) |
| ≤ 10 pack years | 18 | 707 | 1.4 (0.8–2.5) | 1.2 (0.7–2.1) |
| 10.1–20 pack years | 21 | 391 | 2.8 (1.7–4.7) | 2.0 (1.2–3.3) |
| > 20 pack years | 16 | 291 | 3.1 (1.8–5.5) | 2.2 (1.2–3.9) |
| *Test for trend: p = 0.08. ♦ The sum of cases in the subgroups is less than 177 (the total number of cases in the study) due to internal drop-out. † Crude. ‡ Adjusted for alcohol drinking, pain, socio-economic status and when comparing pack years, also adjusted for age. § People who have never smoked. Reference group. ¶ Daily smokers, those who sometimes smoke and those who have stopped smoking. º Those who have stopped smoking. ◊ Daily smokers and those who sometimes smoke. |
| Table IV. Rate ratios (RR) of long-term sick leave due to back or neck pain associated with different amounts of alcohol consumption, together with corresponding 95% confidence intervals (95% CI) |
| Alcohol consumption | Exposed cases♦ (n) | Exposed non-cases (n) | RR† (95% CI) | RR‡ (95% CI)* |
| Frequency |
| Once per month or less often§ | 93 | 2534 | 1.0 | 1.0 |
| Twice per month or more often | 79 | 3769 | 0.6 (0.4–0.8) | 0.8 (0.5–1.2) |
| 2–4 times per month | 69 | 2945 | 0.6 (0.5–0.9) | 0.9 (0.6–1.3) |
| Twice per week or more often | 10 | 824 | 0.3 (0.2–0.6) | 0.4 (0.1–1.1) |
| Amount |
| Quartile 1§ (< 2 drinks/month) | 69 | 1812 | 1.0 | 1.0 |
| Quartile 2 (2–4 drinks/month) | 53 | 2066 | 0.7 (0.5–1.0) | 0.8 (0.5–1.2) |
| Quartile 3 (5–10 drinks/month) | 34 | 1228 | 0.7 (0.5–1.1) | 0.8 (0.4–1.3) |
| Quartile 4 (> 10 drinks/month) | 14 | 1126 | 0.3 (0.2–0.6) | 0.5 (0.2–1.2) |
| *Test for trend: p = 0.04. ♦The sum of cases in the subgroups is less than 177 (the total number of cases in the study) due to internal drop-out. †Crude. ‡Adjusted for daily smoking (ever/never) pain, and socio-economic status. §Reference group. |
There was no correlation between smoking and alcohol consumption (–0.05).
DISCUSSION
This study found that smoking was associated with an increased risk of long-term sick leave due to unspecific back or neck pain and, more surprisingly, that alcohol consumption tends to have a protective effect. The increased risk associated with smoking is inconsistent with the results from the Swedish systematic review from 2004 (3), but in line with more recently published studies (12–14, 18). The difference from the Swedish review may be explained by the thorough analyses in the present study, where smoking was the main exposure and several potential confounders were considered. The study subjects included in the Swedish review were mainly men employed by manufacturing industries (3), whereas this study mainly included female employees in the public sector.
The tendency to a decreased risk associated with alcohol consumption in this study has not, to our knowledge, been shown previously. In some previous studies, alcohol consumption was associated with an increased risk of long-term sick leave in general (19, 20), and one study found no associations (17). The risk associated with alcohol consumption may differ between men and women and between different diseases. Additional analyses stratified by sex suggest a protective effect among women as well as among men in the present study, even though the numbers of men were too low for valid analyses. The study population did not include many high consumers, which precludes studying the effect of heavy drinking. The results apply only to the levels of alcohol consumption that were reported in this population. In the discussion of the possible positive effect of moderate alcohol consumption on long-term sick leave due to unspecific back or neck pain, it is of importance not to forget the negative effects of alcohol consumption on other health conditions.
Since the absolute risk of long-term sick leave due to back or neck pain is not high among the exposed or unexposed, the risk differences (RD) are low. For instance the RD for ever smokers in comparison with non-smokers is 1.8%. However, we consider the differences to be of importance for public health.
The study design and the large number of potential confounders taken into consideration increase the validity of this study. However, residual confounding cannot be excluded. There is discussion about whether general health is a confounder or an intermediate between exposure and the outcome sick leave. In this study, there were no systematic differences between the results when adjusting or not adjusting for general health (Tables III and IV); thus we did not adjust for general health.
Although there is a potential risk of misclassification of the outcome, this is probably of minor importance, since cases were consecutively reported independently, both by the employer and the occupational health services.
The selection of participating county councils and local authorities was not random, since the investigation is part of the longitudinal HAKuL study, including demanding interventions at the workplace and rehabilitation of people on long-term sick leave. However, the participating county councils and local authorities are of different sizes and are located in different parts of Sweden, and the majority of the different occupational groups in the county councils and local authorities are represented in the cohort.
Persons with “bad health for working” and persons on full-time sick leave for any reason at baseline were excluded from the cohort, since exposures predicting long-term sick leave could have been changed due to impaired health status, which would hamper the interpretation of observed associations. However, additional analyses including those with “bad health for working” changed the associations only marginally.
Is there causality? That is, does smoking cause sick leave and does alcohol consumption prevent sick leave due to back or neck pain? The prospective study design, in which the exposures are measured before the occurrence of the outcome, indicates a causal relationship, and the consideration taken to a relatively large number of confounders strengthens the validity of the associations. Do the observed associations between smoking or alcohol and long-term sick leave also apply to the presence of back or neck pain? Is the outcome “sick-leave due to back and neck pain” a severe form of back or neck pain, or are other factors than the actual back or neck health status of more importance for the associations between smoking and alcohol consumption, respectively, and long-term sick leave due to back or neck pain found in this study? In Sweden employees are required to present a medical doctor’s certificate for sick leave longer than 7 days. Most persons with back or neck pain work despite their pain, but sometimes persons with back or neck pain see a medical doctor either to obtain their opinion about whether their work will aggravate the symptoms, or to explain that the pain is not consistent with their work. Through the written medical certificate, the doctor certifies not only that a condition is present, but also that the condition results in limited capacity for work.
It is likely that back or neck pain is an important part of the outcome “sick leave due to back or neck pain”, and therefore it is of interest as to what evidence there is for the association between smoking or alcohol consumption and the risk of back or neck pain. In one review no association was found between alcohol consumption and low back pain, but well-designed specific alcohol/low back pain centred studies were considered lacking (32). In a study from Iceland, women with probable alcohol abuse working in nursing homes had significant medical problems, including pain syndromes, but that was not reflected in more sick leave (33). Smoking has been found to be associated with non-specific back pain, sciatic pain, and neck pain in some studies. Croft et al. (34) found no association between smoking and alcohol consumption, respectively, and neck pain in a longitudinal study. Tubach et al. (14) found no associations between heavy smoking and low back pain, but between heavy smoking and sick leave due to low back pain in the same study, indicating that risk factors differ between low back pain and sick leave due to low back pain. IJzelenberg et al. (35), who found that risk factors differ between musculoskeletal complaints and musculoskeletal sickness absence, also found this. Work-related factors largely determined the occurrence of low back pain and upper-extremity complaints, whereas individual factors predominantly determined sick leave due to musculoskeletal complaints. In the present study, there were significant crude associations between smoking and back or neck pain at enrolment (prevalence ratio (PR) = 1.3, 95% CI: 1.1–1.5), and no association between alcohol consumption and back or neck pain (PR = 0.9, 95% CI: 0.8–1.1) (analyses based on figures in Table II). What is causing the sick leave, apart from back or neck pain, is not known, but it is likely that tradition and socio-economic factors are of importance. Given that the adjustment in the analyses for socio-economic class is valid, we would, in summary, emphasize that the associations between smoking and alcohol, respectively, and long-term sick leave due to back or neck pain found in this study are more related to the pain in back or neck, than to socio-economic factors.
The mechanisms by which smoking or alcohol consumption may influence sick leave due to back or neck pain are not known. The mechanism explaining the increased risk of smoking on back or neck pain might be explained by a decreased circulation in the tissues in the spine from nicotine (36, 37), causing ischaemic pain, decreased function and degeneration of the connective tissues and muscles. The mechanism explaining a possible protective effect of alcohol consumption on back or neck pain might be explained by an anti-inflammatory effect that has been shown in a study of mice. Low but persistent ethanol consumption delayed the onset and halts the progression of collagen-induced arthritis by interaction with innate immune responsiveness (38). Another possible mechanism might be the general relaxing effect that alcohol can have on people, and which probably affects the muscles in the back and neck.
In summary, we believe that the associations found in this study are valid, even though there is a risk of residual confounding, and though the causal chains are complex, precluding strong statements about causality.
In conclusion, our results suggest that smoking is a risk factor for long-term sick leave due to unspecific back or neck pain among employees in the public sector, and that moderate alcohol consumption tends to have a protective effect.
ACKNOWLEDGEMENTS
The authors would like to thank Marianne Ekdahl for her work with the data collection and Stefan Stark for his statistical advice. Financial support for this study was provided by AFA Insurance Co., and Sweden and Health Care Science Postgraduate School, Karolinska Institutet, Sweden.
REFERENCES