OBJECTIVE: The purpose of this study was to describe and analyse self-rated perceived functioning, disability and environmental facilitators/barriers with regard to disease severity, using the International Classification of Functioning, Disability and Health (ICF) checklist, in adults with myotonic dystrophy type 1.
DESIGN: Cross-sectional design.
SUBJECTS: Forty-one women and 29 men with myotonic dystrophy type 1.
METHODS: A modified ICF checklist was used for self-rating of perceived problems in 29 body-function categories, difficulties in 52 activity and participation categories, and facilitators/barriers in 23 environmental-factor categories according to the verbal anchors of the ICF qualifiers. Disease severity classification was based on the muscular impairment rating scale.
RESULTS: Of the persons with myotonic dystrophy type 1, 80% perceived problems of excessive daytime sleepiness, 76% of muscle power, and 66% of energy and drive functions, while over 59% perceived difficulties in physically demanding mobility activities. Disabilities in mobility, self-care and domestic life were more frequently reported by persons with severe disease. Support from the immediate family, medicines and social security services were perceived as facilitators for 50–60% of the participants.
CONCLUSION: Disabilities and important environmental facilitators in adults with myotonic dystrophy type 1were identified, and this clinically-relevant information can be used for developing health services for people with this condition.
Key words: myotonic dystrophy, neuromuscular diseases, classification, health-status measures, rehabilitation, physical therapy.
J Rehabil Med 2009; 41: 512–520
Correspondence address: Marie Kierkegaard, Department of Physical Therapy, R1: 07 Karolinska University Hospital, SE-171 76 Stockholm, Sweden. E-mail: marie.kierkegaard@karolinska.se
Submitted October 29, 2008; accepted February 20, 2009
INTRODUCTION
Myotonic dystrophy type 1 (DM1), with an estimated European prevalence of 5–20/100,000, is a slowly-progressive multisystem disease (1). It is inherited in an autosomally dominant pattern and with anticipation, i.e. progressively younger onset and increasing severity in successive generations in a family. The genetic basis is a mutation on chromosome 19 with an unstable expansion of a trinucleotide (CTG) repeat (2). Four forms are described; congenital, childhood, classic adult and mild adult. They are based on age at onset, clinical symptoms and CTG expansion size (1, 3).
As it is a multisystem disease, DM1 affects several body functions and structures. In the DM1 population, symptoms vary in both presentation and severity (1). Characteristic features are muscular weakness and wasting, and myotonia. Distal limb, facial and neck flexor muscles are affected first, but as the disease progresses proximal muscles become involved (4). A disease-specific rating scale, the muscular impairment rating scale (MIRS), has been developed for DM1 (5). The scale tallies with the usual distal-to-proximal progression of the muscular involvement and can be used to describe disease severity (5). Impairments in the ocular, cardiovascular, respiratory, digestive, metabolic and endocrine systems and in the central nervous system can also occur (1). Furthermore, disrupted life habits have been reported in mobility, domestic life, leisure and work (6). Nevertheless, information on self-perceived health aspects is limited and sparse (7).
One way to describe how people experience their health is to use the International Classification of Functioning, Disability and Health (ICF) (8). This classification system provides a common international language, a standardized coding system and a framework for describing health and health-related states from the perspectives of body, individual and society. In the ICF, “functioning” is an umbrella term indicating non-problematic or neutral aspects of health. “Disability”, on the other hand, indicates problems and summarizes body function and structure impairments, activity limitations and participation restrictions. Contextual factors, i.e. personal and environmental factors, influence both the health state and the health perception of individuals. In the ICF, environmental factors can be described as facilitators of, or barriers to, functioning (8).
The ICF is used both in clinical practice and in research for assessment, intervention and evaluation purposes (8). The ICF checklist (9) has been developed to facilitate the use of ICF in clinical practice and consists of a selection of 123 of the classification system’s approximately 1400 categories. While the ICF checklist is not a psychometric measure, an individual’s functioning and/or disability is classified using qualifiers on a 5-point ordinal scale. Usually the disability is classified or quantified by health professionals. However, knowledge of the patients’ own perception of functioning and disability, and of environmental facilitators or barriers, is of significant value and can assist in the development of health services. Thus, the aim of the present study was to describe and analyse self-rated perceived functioning, disability and environmental facilitators/barriers with regard to disease severity, using the ICF checklist, in adults with DM1.
METHODS
Participants
For recruitment of participants, all the major hospitals and private practitioners with neurological speciality in Stockholm County Council were contacted and informed about the study. This resulted in a list of 128 persons, mainly from the outpatient clinic at the Department of Neurology at the Karolinska University Hospital, Stockholm, Sweden. The inclusion criteria were: diagnosed DM1, 18 years of age or older, and living in the Stockholm County Council area. Twenty-one of the 128 persons did not fulfil the inclusion criteria (14 had other muscular dystrophies or myotonic disorders, 5 lived outside the area, one had died and one was younger than 18 years) and we failed to contact 4. Of the remaining 103 persons, 33 declined to participate, and thus 70 persons with DM1 were included. The diagnosis was genetically confirmed either in participants (n = 69) or in a first-degree family member (n = 1). The participants were grouped by DM1 form by 2 independent neurologists. Fifty-eight were classified as having adult-onset forms and 12 the childhood form.
The study was approved by the Regional Ethical Review Board in Stockholm, and all participants gave their signed informed consent before enrolment.
Measures and procedures
Disease severity was classified by the first author and was based on the disease-specific MIRS (5), an ordinal 5-point scale, where 1 is no muscular impairment, 2 minimal signs, 3 distal weakness, 4 mild-to-moderate proximal weakness and 5 severe proximal weakness. MIRS grades 1–3 were defined as mild and MIRS grades 4–5 as severe disease.
A structured interview was used to collect information on disease-related factors and demographic characteristics, i.e. contextual factors. Thereafter the ICF checklist, in a modified version (see Appendix I), was used for self-rating of functioning, disability and environmental facilitators/barriers according to the verbal anchors of the ICF qualifiers. The main modifications were that body-structure impairments were not rated and that additional categories in the domains mobility and self-care were added. Functioning or disability within activities and participation can be described either as a person’s capacity or, as in the present study, as performance. The latter indicates what a person does in his or her current environment, with assistive devices if needed. We used a single list for activities and participation domains and did not distinguish between activities and participation in the coding of functioning and disability. The categories of the modified ICF checklist were presented to each participant in colloquial language and, if necessary, the meaning of a category was explained in more detail. Participants were asked if they had any body-function problems, any activity and participation difficulties, and any environmental facilitators/barriers. Perceived problems in 29 body-function categories and difficulties in 52 activity and participation categories were rated by the participants with the following qualifiers: 0 = no problem/difficulty, 1 = mild problem/difficulty, 2 = moderate problem/difficulty, 3 = severe problem/difficulty and 4 = complete (sic) problem/difficulty. Twenty-three environmental-factor categories were rated either as perceived facilitators or barriers, using the following qualifiers: 0 = no facilitator/barrier, +1 = mild facilitator, +2 = moderate facilitator, +3 = substantial facilitator, +4 = complete facilitator, 1 = mild barrier, 2 = moderate barrier, 3 = severe barrier and 4 = complete barrier.
Statistical methods
Drop- out analyses were performed with a χ2 test for gender and with an unrelated t-test for age.
Descriptive statistics were used for disease-related and demographic characteristics. Each person’s total number of body-function disabilities and of activity and participation disabilities was calculated by adding up the categories that were rated as a problem or difficulty.
In the frequency presentation of self-ratings in all ICF categories, the 0–4 qualifier scale was transformed to a 3-graded scale (10). Categories for which less than 20% of the participants rated problems/difficulties/facilitators were considered of less relevance and are therefore not reported.
Differences in disability with regard to disease severity were analysed using the Mann-Whitney U test and the Fisher’s exact test. The qualifier scale was dichotomized as no problem/difficulty (qualifier 0) and problem/difficulty (qualifier 1–4). Due to the large number of outcome variables, the level of significance was set to p ≤ 0.001.
In the description of different disabilities in relation to environmental facilitators, body-function categories were reduced to represent 8 domains, activity and participation categories to represent 9 domains, and environmental-factor categories to represent 3 domains. A domain was coded as a disability or facilitator if any of the categories within that domain was rated as a problem/difficulty or facilitator, respectively. All the analyses were performed using SPSS for Windows (release 15.0).
RESULTS
Forty-one women and 29 men with DM1, with a mean age of 45 years (standard deviation (SD) 13, age range 19–70 years) participated in the study. There were no significant differences in age or gender between the 33 persons who declined to participate and the 70 who participated. Disease-related factors and demographic characteristics, i.e. contextual factors, from the structured interview are presented in Table I. Thirty-seven were classified as having mild disease and 33 as having severe. The median number of self-rated disabilities was 10 (interquartile range (IQR) 6–13, range 1–18) for body-function categories and 10 (IQR 3–19, range 0–38) for activity and participation categories.
| Table I. Disease-related factors and demographic characteristics of persons with myotonic dystrophy type 1 (DM1) (n = 70). The total percentage may exceed 100 due to rounding to whole numbers |
| | n | % |
| Form of DM1 | | |
| Mild adult | 2 | 3 |
| Classic adult | 56 | 80 |
| Childhood | 12 | 17 |
| MIRS grade | | |
| 1 No muscular impairment | 3 | 4 |
| 2 Minimal signs | 13 | 19 |
| 3 Distal weakness | 21 | 30 |
| 4 Mild-moderate proximal weakness | 13 | 19 |
| 5 Severe proximal weakness | 20 | 29 |
| CNS-stimulant drugs | | |
| Modafinil/methylphenidate | 17/9 | 24/13 |
| Aids | | |
| ADL and/or orthotic aids | 42 | 60 |
| Mobility aids | 25 | 36 |
| Home adaptations | 31 | 44 |
| Personal care assistance | 18 | 26 |
| Education level | | |
| University | 19 | 27 |
| Civil status | | |
| Cohabiting with partner | 31 | 44 |
| Employment status | | |
| Working part-/full-time | 26 | 37 |
| MIRS: muscular impairment rating scale; CNS: central nervous system; ADL: activities of daily living. |
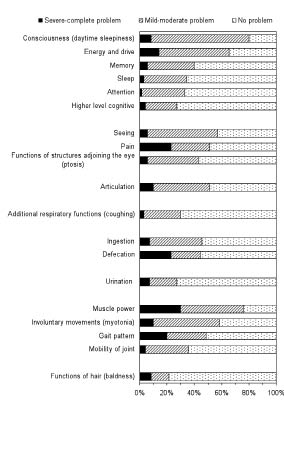
Body-function categories for which 20% or more of the persons with DM1 rated problems are presented in Fig. 1. Eighty percent perceived problems of excessive daytime sleepiness, 76% of muscle power, and 66% of energy and drive functions. Thirty percent rated severe or complete problems of muscle power functions, 23% of defecation functions and 23% perceived pain as a severe or complete problem.
Fig. 1. Body-function categories for which 20% or more of the persons with myotonic dystrophy type 1 (DM1) (n = 70) rated problems.
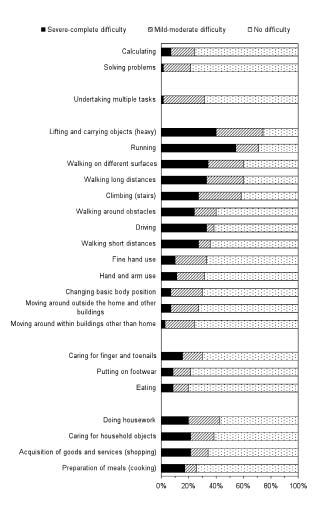
Activity and participation categories for which 20% or more of the participants rated difficulties are presented in Fig. 2. Between 59% and 74% perceived difficulties in physically demanding mobility activities, such as lifting and carrying heavy objects, running, walking on different surfaces or long distances, and climbing stairs. Fifty-four percent perceived severe-to-complete difficulty in running, 40% in lifting and carrying heavy objects and 34% in walking on different surfaces.
Fig. 2. Activity and participation categories for which 20% or more of the persons with myotonic dystrophy type 1 (DM1) (n = 70) rated difficulties.
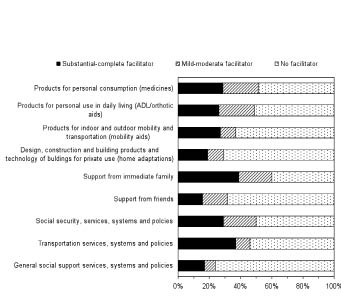
Environmental-factor categories rated by 20% or more of the persons with DM1 as facilitators are presented in Fig. 3. Between 50% and 60% perceived support from the immediate family, medicines, social security services, and aids for personal use in daily living, as facilitators. Thirty-nine percent rated support from the immediate family, 37% transport services, 29% medicines and 29% social security services as a substantial or complete facilitator. Categories that no-one rated as facilitators included support from health professionals and all categories from the domain attitudes. None rated the 23 environmental factors as barriers to functioning.
Fig. 3. Environmental-factor categories that 20% or more of the persons with myotonic dystrophy type 1 (DM1) (n = 70) rated as facilitators.
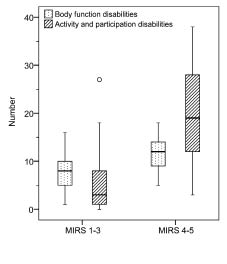
Persons with severe disease reported more disabilities than did those with mild disease (p ≤ 0.001); especially activity and participation disabilities, where the median value was 3 (IQR 1–9, range 0–27) for those with mild disease and 19 (IQR 12–29, range 3–38) for those with severe disease (Fig. 4). Differences in self-rated functioning and disability with regard to disease severity were found in 4 of 29 body-function categories and in 25 of 52 activity and participation categories (p ≤ 0.001), see Table II. Disability in neuromusculoskeletal and movement-related functions, and in mobility, self-care and domestic life domains, were more frequently reported by persons with severe disease. Between 60% and 100% of the participants with self-rated disabilities perceived environmental domains as facilitators (Table III). Twenty-one of 26 participants who reported use of prescribed central nervous system stimulants against excessive daytime sleepiness rated medicines as a facilitating environmental factor. Thirty-three of 42 persons who used aids to activities of daily living and/or orthotic aids, all 25 who had mobility aids, 20 of 31 who had home adaptations, and 17 of 18 who had personal care assistance rated these environmental factors as facilitators.
Fig. 4. Reported total number of body-function disabilities and of activity and participation disabilities with regard to mild (MIRS 1–3) and severe (MIRS 4–5) disease. The box-plots show median, quartiles and min-max non-outliers, and an outlier (o). MIRS: muscular impairment rating scale.
| Table II. Disability (problem/difficulty) and functioning (no problem/difficulty) reported by persons with myotonic dystrophy type 1 (DM1) for which significant differences were found between mild (MIRS 1–3, n = 37) and severe (MIRS 4–5, n = 33) disease |
| | Disability | | Functioning | p-value |
| MIRS 1–3 n (%) | MIRS 4–5 n (%) | | MIRS 1–3 n (%) | MIRS 4–5 n (%) |
| Body functions |
| Respiratory muscle | 0 (0) | 11 (33) | | 37 (100) | 22 (67) | < 0.001 |
| Mobility of joint | 6 (16) | 19 (58) | | 31 (84) | 14 (42) | < 0.001 |
| Muscle power | 21 (57) | 32 (97) | | 16 (43) | 1 (3) | < 0.001 |
| Gait pattern functions | 9 (24) | 25 (76) | | 28 (76) | 8 (24) | < 0.001 |
| Activities and participation |
| Mobility | | | | | | | | | | |
| Changing basic body position | 1 (3) | 20 (61) | | 36 (97) | 13 (39) | < 0.001 |
| Lifting and carrying objects (heavy objects) | 20 (54) | 32 (97) | | 17 (46) | 1 (3) | < 0.001 |
| Hand and arm use | 3 (8) | 19 (58) | | 34 (92) | 14 (42) | < 0.001 |
| Walking short distances | 2 (5) | 23 (70) | | 35 (95) | 10 (30) | < 0.001 |
| Walking long distances | 12 (32) | 30 (91) | | 25 (68) | 3 (9) | < 0.001 |
| Walking on different surfaces | 10 (27) | 32 (97) | | 27 (73) | 1 (3) | < 0.001 |
| Walking around obstacles | 1 (3) | 27 (82) | | 36 (97) | 6 (18) | < 0.001 |
| Climbing (stairs) | 11 (30) | 30 (91) | | 26 (70) | 3 (9) | < 0.001 |
| Running | 17 (46) | 33 (100) | | 20 (54) | 0 (0) | < 0.001 |
| Moving around within buildings other than home | 1 (3) | 16 (48) | | 36 (97) | 17 (52) | < 0.001 |
| Moving around outside the home and other buildings | 1 (3) | 18 (55) | | 36 (97) | 15 (45) | < 0.001 |
| Using transportation | 0 (0) | 11 (33) | | 37 (100) | 22 (67) | < 0.001 |
| Driving | 7 (19) | 20 (61) | | 30 (81) | 13 (39) | < 0.001 |
| Self-care | | | | | | | | | | < 0.001 |
| Washing whole body | 0 (0) | 13 (39) | | 37 (100) | 20 (61) | < 0.001 |
| Drying oneself | 0 (0) | 10 (30) | | 37 (100) | 23 (70) | < 0.001 |
| Caring for hair | 0 (0) | 8 (24) | | 37 (100) | 25 (76) | 0.001 |
| Putting on clothes | 0 (0) | 12 (36) | | 37 (100) | 21 (64) | < 0.001 |
| Taking off clothes | 0 (0) | 12 (36) | | 37 (100) | 21 (64) | < 0.001 |
| Putting on footwear | 0 (0) | 15 (45) | | 37 (100) | 18 (55) | < 0.001 |
| Taking off footwear | 0 (0) | 10 (30) | | 37 (100) | 23 (70) | < 0.001 |
| Eating | 0 (0) | 14 (42) | | 37 (100) | 19 (58) | < 0.001 |
| Drinking | 0 (0) | 8 (24) | | 37 (100) | 25 (76) | 0.001 |
| Domestic life | | | | | | | | | | |
| Acquisition of goods and services (shopping) | 5 (14) | 19 (58) | | 32 (86) | 14 (42) | < 0.001 |
| Doing housework | 7 (19) | 23 (70) | | 30 (81) | 10 (30) | < 0.001 |
| Caring for household objects | 7 (19) | 20 (61) | | 30 (81) | 13 (39) | 0.001 |
| MIRS: muscular impairment rating scale. |
| Table III. Number of persons with myotonic dystrophy type 1 (DM1) (n = 70) with self-rated disabilities who perceived environmental domains as facilitators |
| | | Environmental domains |
| Disabilities n (%) | Products and technology n (%) | Support and relationships n (%) | Services, systems and policies n (%) |
| Body functions |
| Mental functions | 66 (94) | 51 (77) | 48 (73) | 44 (67) |
| Sensory functions and pain | 59 (84) | 45 (76) | 42 (71) | 42 (71) |
| Voice and speech functions | 39 (56) | 32 (82) | 31 (79) | 30 (77) |
| Functions of the cardiovascular, haematological, immunological and respiratory systems | 36 (51) | 28 (78) | 24 (67) | 26 (72) |
| Functions of the digestive, metabolic and endocrine systems | 45 (64) | 38 (84) | 35 (78) | 31 (69) |
| Genitourinary and reproductive functions | 19 (27) | 18 (95) | 13 (68) | 15 (79) |
| Neuromusculoskeletal and movement-related functions | 63 (90) | 49 (78) | 46 (73) | 43 (68) |
| Functions of the skin and related structures | 15 (21) | 12 (80) | 12 (80) | 9 (60) |
| Activities and participation |
| Learning and applying knowledge | 24 (34) | 19 (79) | 21 (88) | 20 (83) |
| General tasks and demands | 25 (36) | 21 (84) | 23 (92) | 22 (88) |
| Communication | 5 (7) | 4 (80) | 5 (100) | 4 (80) |
| Mobility | 60 (86) | 48 (80) | 47 (78) | 45 (75) |
| Self-care | 27 (39) | 26 (96) | 25 (93) | 26 (96) |
| Domestic life | 38 (54) | 35 (92) | 36 (95) | 35 (92) |
| Interpersonal interactions and relationships | 14 (20) | 12 (86) | 14 (100) | 13 (93) |
| Major life areas | 13 (19) | 11 (85) | 13 (100) | 12 (92) |
| Community, social and civic life | 6 (9) | 5 (83) | 6 (100) | 6 (100) |
DISCUSSION
The main finding in the present study was the identification of commonly occurring self-rated disabilities and environmental facilitators in persons with DM1.
The body functions for which over half our study sample perceived problems reflect impairments that are often-described symptoms of DM1 (1). Excessive daytime sleepiness was the most common impairment, with 80% perceiving problems to some extent, which is higher than previously reported (11–14). This could be due to different assessment methods. Whereas we described self-rated perceived problems, others have reported the proportion of persons scoring over a cut-off point in various standardized questionnaires. This might have led to an underestimation of the problem. The causes of excessive daytime sleepiness are not fully understood; however, a central mechanism has been proposed and psychostimulants are used to increase alertness. Given the extent of the problem, other non-pharmacological approaches might be worth considering, for example physical exercise. Daytime sleepiness is associated with low physical activity levels in patients with sleep apnoea (15), and in older adults (16). Participation in a tai chi exercise programme reportedly reduces daytime sleepiness in older adults (17). The effect of physical exercise on daytime sleepiness in persons with DM1 has not, however, yet been studied.
Impairments in muscle power were expected, and muscle weakness has been documented in several studies (4, 18, 19). However, even minor reductions could be rated as major problems, indicating that the perception of an impairment is relative and highly individual. Myotonia is a cardinal symptom of DM1 and occurs more frequently in mildly affected persons, reportedly as a problem of less extent (1). Nonetheless, our results show that 59% of the participants, including both those with mild and severe disease, perceived impairments. Knowledge of the individual’s perception of problems is therefore important, so that individually-tailored health services can be offered. Pain has been recognized as a common problem for many persons with slowly-progressive neuromuscular diseases (20), and the fact that 23% of our study sample perceived pain as a severe or complete problem emphasizes the importance of developing strategies for management of pain in clinical practice.
In agreement with previous findings, activity and participation difficulties were reported mainly in physically demanding mobility and domestic-life activities (6, 14, 21–23). That the most frequently reported disabilities seemed to be related to muscle strength indicates the need for interventions. The role of exercise in DM1 has been debated, since it is unclear how exertion affects the diseased neuromuscular system. Moderate-intensive strength training seems to do no harm (24), but further research is needed to establish whether exercise programmes are beneficial.
Very few participants with mild disease and surprisingly few with severe disease perceived difficulties in self-care. This could be because performance, and not capacity, was rated. The use of aids or assistance in self-care activities was, however, not fully understood in our study, since the participants did not rate environmental factors in relation to activity and participation categories. On the other hand, the use of devices and techniques, aids or assistance, as well as a high level of satisfaction with self-care activities, have been reported in persons with muscular dystrophies, including DM1 (21), and in adults with DM1 only (6).
Only 3% of our study sample perceived difficulties in recreation and leisure pursuits, in contrast to reports from Gagnon et al. (6), who found that participation in the recreation category was restricted for at least 23% of their sample of 200 adult-onset DM1 participants. Direct comparisons might, however, be complicated, due to different assessment methods and to difficulties in addressing the role of participants’ choices and preferences in ratings. Reports of satisfaction with recreation and leisure activities are contradictory. Low satisfaction was observed in the study of Gagnon et al. (6), whereas Nätterlund & Ahlström (21) state that their study sample seemed satisfied. Even though many of their respondents with muscular dystrophies reported that they did not have a leisure activity, few wished for a improved situation (21). Whether persons with DM1 perceive activity limitations and/or participation restrictions in the domain community, social and civic life needs further study.
Integration of environmental factors in a person’s description of their health condition has been highlighted and is considered to play a central role (25). Our participants did not rate environmental factors as barriers. This is in contrast to the study by Gagnon et al. (14), in which 17–51% reported various types of environmental barrier to participation. The difference could lie in the varying provision of aids, assistance, government services, etc. between countries, or that we did not elicit the effect of a specific environmental factor on a specific activity. The fact that none of the persons with DM1 in our study rated support from health professionals, and less than 20% rated health services, systems and policies as facilitators, highlights possible areas for improvements in health services.
ICF codes without qualifiers have no inherent meaning according to the ICF (8). However, information on the validity, reliability and sensitivity of the qualifier measurement system is scarce. We have found only 5 studies, all exploring reliability, which reported low-to-moderate agreement (10, 26–29). Improved reliability was shown by Uhlig et al. (10) when the scale was reduced from 5 grades to 3. Consequently we used a 3-grade scale for descriptive purposes and dichotomized the categories for analysis.
The ICF checklist was altered on the basis of findings presented in the literature, clinical experience, and the fact that we were going to use it for self-assessment. However, redundant information was collected in the mobility and self-care domains and fewer categories should be selected for use in clinical practice. Specific core sets, i.e. lists of ICF categories considered relevant for describing a disease, have been formulated for other disorders (30, 31) and settings (32). Even if a DM1-specific core set was developed, a potential barrier to clinical use is the ICF language. We found that it was sometimes difficult to understand, and we had to translate categories into everyday language to be able to use the checklist. Maybe these difficulties can be overcome by developing specific ICF assessment tools or by “translating” existing outcome measures to ICF, for which linking rules have been developed (33). We agree with Stucki (34), that the ICF can be used to identify “what?”, but not “how”, to measure.
Assessment of human functioning, disability and health is a unique feature in physical and rehabilitation medicine, and is used to understand a person’s experience of disability, so that health services can be selected aiming at optimizing function (35). We have used the ICF checklist for self-assessment, and thus described functioning and disability from an individual’s point of view. That our participants showed such varied disabilities stresses the importance of comprehensive evaluations and implies that a multi-professional approach is needed for optimal care. The next step will be to describe and analyse how self-rated perceived function and disability, quantified by the ICF qualifiers, correlates with data from clinical examinations, functional assessments and established questionnaires. Such information could be used to identify rehabilitation strategies.
In conclusion, disabilities and important environmental facilitators in adults with DM1 have been identified, and this clinically-relevant information can be used for developing health services for people with this condition.
ACKNOWLEDGEMENTS
This research was supported by grants from the Swedish Association of Registered Physiotherapists, the Swedish Association of Persons with Neurological Disabilities, the Stockholm County Council and Karolinska Institutet (ALF project funding), Einar Belvén Foundation and AFA Insurance.
REFERENCES