OBJECTIVE: To investigate the outcome of motor training programmes on arm and hand functioning in patients with cervical spinal cord injury according to different levels of the International Classification of Functioning, Disability and Health (ICF).
DESIGN: Systematic review.
METHODS: A search of the following databases: Medline, Cochrane, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, Physiotherapy Evidence Database (PEDro) and Database of Abstracts of Reviews of Effects (DARE) from 1976 to August 2008 was performed using the following MeSH terms: Spinal Cord Injuries, Quadriplegia, Rehabilitation, Physical Education and Training, Exercise, Patient-Centered Care, Upper Extremity, Activities of Daily Living, Motor Skills, Motor Activity, Intervention Studies, Clinical Trial. The methodological quality of the selected articles was scored with the Van Tulder Checklist. Descriptive analyses were performed using the PICO principle (Patient characteristics, Intervention, Comparison, Outcome & results) along the ICF function and activity level.
RESULTS: Twelve studies were included in the analyses. Overall, the methodological quality of the studies was acceptable, with a mean Van Tulder score of 9.58. Interventions included motor training programmes at the level of function, activity or a combined programme. Most studies reported improvements in arm and hand functioning at the level that was trained for.
CONCLUSION: Motor training programmes may improve arm and hand functioning at function and/or activity level in cervical spinal cord injured patients. However, no general conclusion based on a meta-analysis can be drawn due to the wide variety of approaches.
Key words: spinal cord injury, motor training, upper extremity, ICF, systematic review.
J Rehabil Med 2009; 41: 497–505
Correspondence address: Annemie I. F. Spooren, Zandbergseweg 111, NL-6432 CC Hoensbroek, The Netherlands. E-mail: aspooren@mail.phl.be
Submitted November 14, 2008; accepted April 7, 2009
INTRODUCTION
Persons with cervical spinal cord injury (C-SCI) demonstrate, in addition to the loss of function in the lower extremities and trunk, motor and sensory loss in the arms and hands. The level of functioning in these persons is, for the most part, determined by the impairments of the arm and hand. Both Hanson & Franklin (1) and Snoek et al. (2, 3) reported that restoration of arm and hand function is a major priority for persons with a cervical spinal cord injury.
To establish a good rehabilitation policy for arm and hand in patients with C-SCI, evaluation of, and insight into, the outcome of arm and hand, as well as insight into training programmes for arm and hand according to the different levels of the International Classification of Functioning Disability and Health (ICF) (4) are necessary.
Research on outcome and evaluation of arm and hand used to focus mainly on function level according to the ICF, termed “arm hand function” (AHF). Outcome at this level was described by evaluating, among other factors, muscle strength, neurological level and motor score (5–11). However, clinicians and patients are more interested in the performance of arm and hand activities, termed “arm hand skilled performance” (AHSP) (12, 13). They want to know what patients eventually will be able to do with their arms and hands. At the activity level a distinction is made between basic activities such as grasping and reaching and complex activities such as dressing oneself and eating (4). Unfortunately, there is a lack of instruments available to evaluate AHSP (14). Some studies described outcome on the level of complex activities as measured by the Functional Independence Measure (FIMTM), the Spinal Cord Independence Measure (SCIM) and the Modified Barthel Index (MBI) (11, 15–19). However, these measures did not give specific information on basic activities of arm and hand in persons with C-SCI. Recently, more research was performed on evaluation and outcome of AHSP on the level of basic and complex activities (12, 13, 20, 21). For example, the Van Lieshout Test (VLT) and the Grasp Release Test (GRT) have been designed to evaluate basic activities in persons with C-SCI (20, 22, 23) and they were found to be responsive in detecting changes over time in C-SCI (12). Spooren et al. (13) reported that monitoring the outcome of AHSP at the level of basic and complex activities during the whole rehabilitation phase may guide therapists in further optimizing therapy.
Besides evaluation and knowledge on outcome of AHSP, a comprehensive view of training programmes aimed at improving arm and hand functioning is crucial in assisting clinicians to optimize their patient’s capacities, for the following reasons: (i) because a small improvement in arm and hand functioning may induce a substantial increase in possibilities to perform tasks and an increased independence in daily activities. This, in turn, may lead to improved quality of life (2, 24, 25). Also, (ii) because patients need to relearn skills involving their upper extremities using different strategies than previously. Research showed that repetitive sensori-motor training is the best way to learn new skills (26–28).
Although a large amount of clinical experience on training programmes is present, very little evidence on the effectiveness has been systematically reported. In general, reports on training programmes of persons with a C-SCI are focused mainly on increasing physical capacity and physical fitness expressed by peak oxygen uptake and peak power output (29–35). Research on arm and hand functioning is focused mainly on hand surgery (36–39), the use of functional electrical stimulation (40–42), neuroprostheses (43–45) or orthosis use (46, 47), i.e. focused on compensation of function loss. However, these approaches do not automatically lead to improved skilled performance. For the latter, extensive and repetitive sensori-motor training is needed (26–28, 48, 49), possibly in conjunction with the aforementioned, more technical, approaches.
Analogous to the outcome and evaluation of arm and hand functioning, in the past, training used to focus mainly on function level. However, recent developments on motor learning emphasize the importance of skill training at the activity level according to the ICF (27). Whereas the more technically oriented studies are, in general, less focused on the contribution of the motor programmes accompanying these technical approaches, an overview of results of isolated motor training programmes seems to be lacking.
The aim of the present study was to present a systematic review of intervention studies reporting on isolated motor training programmes at the ICF function and activity level to improve AHF or AHSP in persons with C-SCI. The studies will be described using the PICO principle (50), i.e. Patient characteristics, Intervention, Comparison, Outcome & results along the ICF level of “function” and “activity”.
METHODS
Search strategy
A computerized search was conducted on all English, French, German and Dutch articles in the following databases: Medline (PubMed), Cochrane, Cumulative Index to Nursing and Allied Health Literature (CINAHL), EMBASE, Physiotherapy Evidence Database (PEDro), and Database of Abstracts of Reviews of Effects (DARE). Studies were collected from 1976 up to August 2008. Reference lists of these articles and narrative reviews were also scanned for relevant publications.
We used Medical Subject Headings (MeSH) terms that included (“Spinal Cord Injuries” OR “Quadriplegia” NOT “Cerebral Palsy”) AND (“Rehabilitation” OR “Physical Education and Training” OR “Exercise” OR “Exercise Movement Techniques” OR “Physical Therapy Modalities” OR “Patient-Centered Care”) AND (“Upper Extremity” OR “Activities of Daily Living” OR “Motor Skills” OR “Motor Activity” OR words as “activities” OR “activity” NOT “Gait Disorders, Neurologic” NOT “Walking”) AND (“Intervention Studies” OR “Clinical Trial OR “Review Literature”).
Eligible studies
Studies were included when persons with C-SCI were involved in an intervention study or a clinical trial in which a motor training programme was used aimed at improving AHF or AHSP. Studies on functional electro-stimulation, neuroprostheses, surgery or new rehabilitation techniques, such as the use of robotics or virtual reality, were included only if a control group received a conventional motor training programme aimed at improving arm and hand functioning.
Ineligible studies
Animal and observational studies were excluded. Studies featuring orthoses or assistive devices, and physical fitness studies focusing on physical capacity outcome or cardio-respiratory functioning were also excluded. Two independent observers conducted data selection/extraction.
Methodological assessment
Two independent observers rated the methodological quality of the selected studies with the Van Tulder’s Quality assessment system. This scale scores the internal validity (maximum 11 points), the descriptive criteria (maximum 6 points) and the statistical criteria (maximum 2 points) of randomized controlled trials (RCT), but it can also be used to scale controlled clinical trials (51, 52). As patients and care providers are aware of the training they received or provided, the items “blinding of patients” and “blinding of care provider” of the internal validity score were considered to be not applicable. Therefore, the total quality assessment was based on 17 items. The inter-rater reliability of the individual items was tested using Cohen’s Kappa. The quality total Van Tulder score was obtained using the consensus method, i.e. the total score was calculated after any disagreement on item scores had been discussed and resolved.
Descriptive assessment
All the selected articles were subsequently analysed by two independent observers on the following items using the PICO principle (50): Patients (age, International Standards for Neurological Classification of Spinal Cord Injury (by lesion level and lesion completeness) (53), time after injury), Intervention (type, intensity, duration, frequency), Comparison and Outcome & results.
Furthermore, if no consensus on data selection and extraction, methodological and descriptive assessment was achieved between the two independent observers, a third independent observer made the final decision.
RESULTS
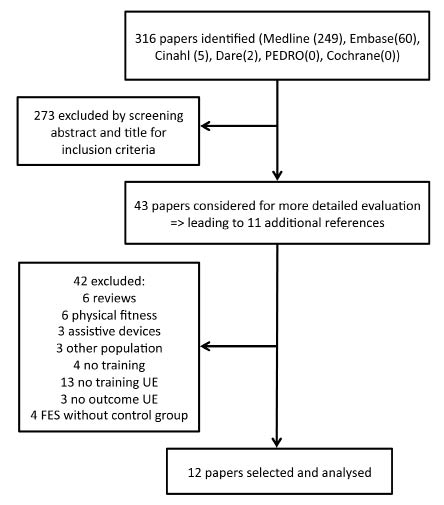
The process of selection of the studies is shown in Fig.1.
Fig. 1. Process of data selection. UE: upper extremities; FES: functional electrical stimulation.
Methodological quality assessment
Table I presents the Van Tulder score of the 12 studies included with the total score, the score of internal validity, the descriptive and the statistical score and the level of evidence according to the Dutch Institute for Healthcare Improvement (CBO) guidelines (see Appendix I).
| Table I. Van Tulder score |
| Reference | Total score | Internal validity score | Descriptive score | Statistical score | Level of evidence |
| Curtis 1999 (62) | 12 | 6 | 4 | 2 | B |
| Hicks 2003 (56) | 11 | 5 | 4 | 2 | B |
| Nawoczenski 2006 (58) | 10 | 5 | 3 | 2 | B |
| Seeger 1989 (63) | 8 | 4 | 2 | 2 | B |
| Needham-Shropshire 1997 (59) | 10 | 4 | 5 | 1 | B |
| Beekhuizen 2005 (54) | 12 | 6 | 4 | 2 | B |
| Beekhuizen 2008 (55) | 11 | 5 | 4 | 2 | B |
| Hoffman 2007 (65) | 8 | 4 | 3 | 1 | C |
| Klose 1990 (57) | 11 | 6 | 4 | 1 | B |
| Kohlmeyer 1996 (60) | 9 | 4 | 4 | 1 | B |
| Popovic 2006 (61) | 9 | 4 | 3 | 2 | B |
| Lugo 2007 (64) | 4 | 1 | 1 | 2 | C |
| Level of evidence: see Appendix I. |
There was a disagreement on the Van Tulder score regarding 12 of the 204 items, resulting in a mean Cohen’s kappa score from all the 17 items of 0.84. Using the consensus method, the mean Van Tulder score of all the included studies was 9.58 (standard deviation (SD) 2.23).
Nine studies (54–62) had a score of 9 or more, which was considered to represent an acceptable methodological quality, following Van Tulder, who suggested a quality cut-off point of 50% (51). Three studies (63–65) scored less than 9 points and were considered as having a low methodological quality.
Eight of 12 studies (54–56, 58, 61–64) scored the maximum on the statistical score with an overall mean of 1.67 (SD 0.49). The mean descriptive score was 3.42 (SD 1.08), in which Lugo et al. (64) and Seeger et al. (63) scored low. Adverse effects were reported only in the studies of Needham-Shropshire et al. (59) and Popovic et al. (61) and none of the studies included described a follow-up measurement. The mean internal validity score was 4.5 (SD 1.38). Only one RCT mentioned that treatment allocation was concealed (61). Internal validity further decreased due to the absence of “blinded assessment of outcome for intervention”, “intention to treat reports” and “mentioning of co-interventions”.
Although 8 of 12 included studies were RCTs (54–57, 59–62), none of them were double-blinded, and therefore they obtained a score B on the level of evidence according to the Dutch CBO guidelines.
Descriptive analysis
Main characteristics of the included studies are shown in Table II.
Patients
Eight studies (54, 55, 57, 59–61, 63, 65) included only persons with a C-SCI, one of which was a single case study (65) and 3 of which included only persons with a motor incomplete lesion (54, 55, 57). Four studies incorporated paraplegic and tetraplegic patients (56, 58, 62, 64), of which the studies by Nawoczenski et al. (58) and Curtis et al. (62) also included a small number of non-SCI wheelchair users. The latter 2 studies (58, 62) had only a low percentage of tetraplegic patients (< 10% and < 25%, respectively). Both Curtis et al. (62) and Lugo et al. (64) pooled the data from paraplegic and tetraplegic patients except when reporting the Wheelchair User’s Shoulder Pain Index (WUSPI) or the American Spinal Injury Association (ASIA) motor score and the motor FIM. The sample size of the studies varied between 1 and 45 persons, aged between 16 and 64 years. The time since injury fluctuated from 2 weeks to 25 years after injury.
Intervention
Different groups of interventions according to the ICF function and activity level can be distinguished, as is shown in Tables II and III.
| Table III. Intervention details |
| Reference | Intervention details | Training frequency |
| Curtis 1999 (62) | Shoulder exercise programme: 2 static stretching exercises (5 times each; 2 times/day); 3 resistance exercises: 3 sets of 15 repetitions (1 time/day) | 7 times/week for 6 months |
| Hicks 2003 (56) | Shoulder exercise programme: warm-up & stretching; aerobic training – arm ergometry (15–30 min at 70% max heart rate); resistance training (2 exercises/muscle group with 2 sets of 15 repetitions at 50% RM to 3 sets of 10–12 repetitions at 70–80% RM after 4 week- load reassessed every 6 weeks) | 90–120 min/day; 2 times/week for 9 months |
| Nawoczenski 2006 (58) | Shoulder exercise programme: home exercise programme: 3 stretching exercises; 3–4 strengthening exercises with elastic band (increasing resistance and repetitions; control with biofeedback at start and at 4 weeks) | ns min/day; ns times/week for 8 weeks |
| Seeger 1989 (63) | Conventional therapy: isotonic (full ROM) triceps; 8 contractions/min | 15–60 min/day; 3–5 times/week for 3 months: FES + 3 months: conventional |
| Needham-Shropshire 1997 (59) | Voluntary exercise: arm ergometer with speed 60 revolution per min | 4 times 5 min + 3 times 3 min rest/day; 3 times/week for 8 weeks |
| Beekhuizen 2005 (54) | Massed Practice: repetitive practice of tasks: 5 categories: gross upper limb movement, grip, grip with rotation, pinch, pinch with rotation (25 min training with 1 min rest – worst hand unless no contraction of thumb) | 120 min/day; 5 times/week for 3 weeks |
| Beekhuizen 2008 (55) | Massed Practice: repetitive practice of tasks: 5 categories: gross upper limb movement, grip, grip with rotation, pinch, pinch with rotation (25 min training with 1 min rest – worst hand unless no contraction of thumb) | 115 min/day; 5 times/week for 3 weeks |
| Hoffman 2007 (65) | Conventional therapy on upper body and hand (PT + OT: strengthening, NMES, compensatory strategies to tenodesis– 3 times/week; 2 h/day) + Massed Practice (bimanual: 5 categories: 20–25 min each) + somatosensory stimulation right hand | 120 min/day; 3 times/week + 120 min/day; 5 times/week for 3 weeks |
| Klose 1990 (57) | Physical Exercise Therapy (PT + OT): strengthening upper extremity, self-care, transfers, mat-mobility and wheelchair skills (complex activities) | ns min/day; 3 times/week for 16 weeks |
| Kohlmeyer 1996 (60) | Conventional therapy to upper extremity: strengthening, Passive ROM, orthotic intervention, functional activities (mainly basic activities) | 5 times 20 min/day; 5 times/week for 5–6 weeks |
| Popovic 2006 (61) | Conventional therapy to hand function (OT): muscle facilitation, task-specific training– repetitive functional training, strengthening, motor control training using resistance to increase strength, Electrical Stimulation, ADL, caregiver training (basic and complex activities) | 45 min/day; 5 times/week for 12 weeks |
| Lugo 2007 (64) | 2 phasic programme (± 2 weeks inpatients; up to 18 months outpatients) with 5 intervention periods described with therapy goals at the level of activity | ns min/day; ns times/week for 18 months |
| ADL: activities of daily living; FES: functional electrical stimulation; NMES: neuromuscular electrical stimulation; OT: occupational therapy; PT: physiotherapy; ROM: range of motion; RM: repetition maximum; ns: not specified. |
Function level. Three studies (56, 58, 62) focused on the shoulder, with training programmes consisting of stretching exercises combined with aerobic and/or resistance training in supervised sessions (56) or as a home exercise programme (58, 62). Seeger et al. (63) used an isotonic strengthening exercises programme and contrasted it with a programme in which Functional Electro Stimulation (FES) was added. Needham-Shropshire et al. (59) used a voluntary arm ergometry programme to compare with a neuromuscular stimulation-assisted arm ergometry programme.
Activity level. In the studies of Beekhuizen & Field-Fote (54, 55) Massed Practice (MP) was used. MP training is an activity-based programme focused on continuous repetition of tasks in each of 5 categories (54), mainly training hand activities (category: grip, grip with rotation, pinch and pinch with rotation) and, to a lesser extent, upper extremity activities (category: gross upper extremity movement). Beekhuizen & Field-Fote (54, 55) contrasted the MP with 3 other training groups, i.e. a MP + Somatosensory Stimulation group (MP+SS), a SS group and a control group.
Combination of function & activity level. The single case study of Hoffman & Field-Fote (65) combined training on function and activity level in a programme consisting of a conventional exercise programme with bimanual MP and SS. Three other studies combined training on both levels. These studies used a conventional training programme to compare with a FES, a biofeedback or neuromuscular stimulation (NMS)-based training programme (57, 60, 61, 63), all aimed at improving arm and hand functioning. The conventional programme usually consisted of a combination of physiotherapy and occupational therapy. Klose et al. (57) combined strengthening exercises with functional exercises on activity level. The programme used by Kohlmeyer et al. (60) contained additionally passive range of motion (PROM) therapy and an orthotic intervention. In the study of Popovic et al. (61) traditional electro-stimulation and motor control exercises were added.
The study of Lugo et al. (64) differs from the other studies in that intervention was described in order of treatment goals on activity level, but neither explicit information as to the level of training that took place nor concrete description of type, modality or intensity of therapy was formulated.
In general, the length of the training programmes ranged from 3 weeks (54, 55) to 9 months (56), with the exception of 18 months in the study of Lugo et al. (64). Training frequency varied from 2 to 5 times a week, with durations of 15–120 min a day. Lugo et al. (64) and Nawoscenki et al. (58) reported neither training frequency nor therapy time; Curtis et al. (62), Klose et al. (57) and Popovic et al. (61) did not report therapy duration.
Outcome
Eleven studies described outcome at the level of function and 8 studies used outcome measurements at the level of activities, as shown in Table II.
| Table II. Descriptive analysis |
| Reference | TU | Patient (motor training group) | | Intervention | Outcome measurements | Results |
| Lesion level | I/Co (AIS) | Mean age, years (range) | Mean TSI, (range) | Sample size | Other groups: interventions | ICF level | Motor programme | ICF level | Motor outcome | Additional outcomes | ICF level | Motor training group |
| Curtis 1999 (62) | 12 | Tetra/para +others | I/Co | 34.5 | 14.9 years | 21 (7 tetra) | 21 (7 tetra): unknown | FU | Shoulder | FU | WUSPI | | FU | *Decrease shoulder pain |
| Hicks 2003 (56) | 11 | Tetra/para | I/Co | 36.9 (19–65) | 7.7 years (1–22) | 11 (6 tetra) | 12 (7 tetra): education | FU | Shoulder | FU | Muscle strength; pain | RHR; BP; RPE; QOL | FU | *Gains in upper body muscle strength and less pain |
| Nawoczenski 2006 (58) | 10 | Tetra/para (SCI+SB) | I/Co | 47.1 | 17 years | 21 (3 I tetra) | 20 (0 tetra) asympt: no intervention | FU | Shoulder | FU + ACT (partly) | WUSPI; SRQ | Satisfaction score | FU + ACT (partly) | *Reduction pain and improved function measured by SRQ |
| Seeger 1989 (63) | 8 | Tetra (C4-C6) | ? | 34 (22–46) | 8.7 years (1.5–25) | 7 | Crossover: + FES | FU | Arm | FU | Max. force (myometer) | ROM; arm circumferences | FU | No clinically or statistically difference |
| Needham-Shropshire 1997 (59) | 10 | Tetra | I/Co | 24 | 4 years | 11 | 12: NMS (8 week); 11: NMS (4 week) + arm ergometry (4 week) | FU | Arm ergometry | FU | MMT | | FU | Small increase in MMT |
| Beekhuizen 2005 (54) | 12 | Tetra (C5-C7) | I (C/D) | 45 (37–63) | 4.8 years (1–12.8) | 5 | 5: MP+SS | ACT | MP | FU + ACT | Pinch; WMFT; Jebsen | Stimulus intensity; MEP | ACT | *Increase in Jebsen in MP group |
| Beekhuizen 2008 (55) | 11 | Tetra (C4-C7) | I (C/D) | 34.6 (21–64) | 4 years (1–12.8) | 6 | 6: SS; 6: SS+MP; 6: 2 test sessions | ACT | MP | FU + ACT | Pinch; Jebsen; WMFT | MEP; monofilament test | ACT | *Increase in hand functioning (Jebsen) in MP group |
| Hoffman 2007 (65) | 8 | Tetra (C6) | I (B) | 22 | 1 years | 1 | No | FU + ACT | Conventional + MP | FU + ACT | MMT; Jebsen; Chedoke Arm and hand activity inventory | Sensory function; TMS | FU + ACT | Increase in strength. Functional hand skills |
| Klose 1990 (57) | 11 | Tetra (C4-C6) | I | (18–45) | > 1 years | 10 | 10: biofeedback + PET; 10: biofeedback + NMS; 9: NMS + PET | FU + ACT | PET | FU + ACT | MMT; MBI | EMG | FU + ACT | *Increase in MMT and MBI |
| Kohlmeyer 1996 (60) | 9 | Tetra (C4-C6) | I/Co | 43 | 3 weeks | 10 | 10: FES; 13: biofeedback; 10: FES + biofeedback | FU + ACT | Conventional | FU + ACT | MMT; function score evaluation | | FU + ACT | Improvement in MMT and functional score (pooled data 4 groups) |
| Popovic 2006 (61) | 9 | Tetra (C3-C7) | I/Co | 53 (24–70) | 76.2 days (15–243) | 9 | 12: + FES-therapy | FU + ACT | Conventional | ACT | FIM; SCIM; REL test | Consumer perception | ACT | Functional improvement |
| Lugo 2007 (64) | 4 | Tetra/para | I/Co | 32.6 | 3 days (1–80) | 42 (14 tetra) | No | ACT + FU? | Goals | FU + ACT | ASIA motor score; motor FIM | | FU + ACT | Increase in ASIA motor score; *functional increase (FIM) |
| ABCD: AIS (ASIA (American Spinal Injury Association) Impairment Scale-score); ACT: activity level; BP: blood pressure; C: cervical; Co: complete; FES: functional electrical stimulation; FIM: Functional Independence Measure; FU: function level; I: incomplete; ICF: International Classification of Functioning, Disability and Health; Jebsen: Jebsen Handfunction Test; MBI: Modified Barthel Index; MEP: motor evoked potentials; MMT: Manual Muscle Testing; MP: massed practice training; NMS: Neuromuscular Stimulation; para: paraplegia; PET: physical exercise therapy; QOL: quality of life; REL: Rehabilitation Engineering Laboratory Handfunction Test; RHR: resting heart rate; ROM: range of motion; RPE: rating perceived exertion; SB: spina bifida; SCI: spinal cord injury; SCIM: Spinal Cord Independence Measure; SRQ: Shoulder Rating Questionnaire; SS: somatosensory stimulation; tetra: tetraplegia; TMS: Transmagnetic Stimulation; TSI: time since injury; TU: Van Tulder score; WMFT: Wolf Motor Function Test; WUSPI: Wheelchair User’s Shoulder Pain Index; *statistically significant; ?: not specified. |
Function level. Eight studies evaluated muscle strength either of the shoulder (56), the arm (57, 59, 60, 63) or the hand (54, 55, 57, 60, 65) or as a ASIA motor score (64). In the studies focused on the shoulder, pain was used as an outcome measure (56, 58, 62). Other measures at function level were the range of motion (ROM) (63), monofilament sensory test (54, 55, 65) and arm circumferences (63).
Activity level. The Wolf Motor Function test (WMFT) (54, 55), the Jebsen hand function test (54, 55, 65), the Rehabilitation Engineering Laboratory Hand Function Test (REL) (61), the Function Score evaluation (60) and the Chedocke Arm and hand activity Inventory (65) were used to measure basic activities. Complex activities were reported using the FIMTM (61, 64), SCIM (61) and parts of MBI (57). General functioning related to the shoulder was measured using the Shoulder Rating Questionnaire (SRQ) (58).
Comparison
As to the comparison of the interventions, 8 RCTs (54–57, 59–62), one controlled trial (58), one cross-over design study (63) and two studies without a control group (63, 65) were found.
In several studies the reviewed motor training programme served as a control intervention to contrast with other interventions, such as the use of (Functional) Electrical Stimulation (59–61, 63), biofeedback and/or NMS (57), SS (55) or MP with SS (54, 55). For these studies, the results of the groups receiving isolated motor training will be analysed in the next section.
Training effects
Five studies used a function level oriented training programme, but only 4 of these reported outcome measures at the level of function. The 3 studies related to shoulder problems demonstrated a significant improvement in pain (either in relation to a control group (56) or in relation to time (58, 62)). Hicks et al. (56) also demonstrated increased muscle strength in comparison with a control group using a 2 times a week exercise programme lasting for 9 months. Nawoszenski et al. (58) reported an improved functioning expressed by reduced shoulder pain, increased satisfaction and increased score on the shoulder rating scale. The voluntary arm ergometry training study by Needham-Shropshire et al. (59) demonstrated a slight (but not statistically significant) increase in muscle strength. The isotonic exercise programme, used in the study of Seeger et al. (63), did not lead to statistically significant changes in maximum voluntary force (even changes in the FES group were not clinically significant).
The studies with motor training programmes at activity level have outcome measurements both at the level of function and activity (basic activities of hand and upper extremity). The MP group in the pilot study of Beekhuizen & Field-Fote (54), demonstrated a statistically significant increase on the Jebsen Hand function test, but not on the WMFT and the pinch grip force. These findings were confirmed in the larger RCT in which the MP group demonstrates a significant improvement in hand functioning (as measured by the Jebsen hand function test) compared with the control group, but not on the upper extremity functioning (as measured by the WMFT) and the pinch grip force at function level compared with the control group (55).
As to a motor training programmes at the level of function and activity, the conventional therapy used by both Klose et al. (57) and Kohlmeyer et al. (60) demonstrated a functional improvement and an increase in muscle strength over time. They compared isolated motor training with motor programmes adding other specific therapies, such as FES, Biofeedback or NMS, but no superiority of any specific therapy was found (57, 60). Popovic et al. (61) demonstrated a functional improvement over time, in which the group receiving conventional therapy tended to make less improvement than the FES group (although this difference was not statistically significant). The latter did not report outcome at the level of function. The combination of bimanual MP with SS and conventional therapy in the study of Hoffman & Field-Fote (65) led to an increase in the performance of functional hand skills (as measured by the Jebsen Hand Function Test and the Chedoke arm and hand activity inventory), in muscle strength and in sensory function.
The study of Lugo et al. (64) featuring a set of standardized therapy goals, showed an increase on the ASIA motor score (function level) and on the motor FIM (activity level) from onset of rehabilitation to 18 months after the start of the rehabilitation.
DISCUSSION
In general, the results of this systematic review demonstrate a limited number of studies related to isolated motor training of arm and hand functioning in persons with C-SCI, including a wide variety of types of patients, training, methodology and outcome parameters. The studies included revealed that an improvement in arm hand function or arm hand skilled performance is possible with training in the acute and chronic phases. This conclusion is at level 2 according to the Dutch CBO guidelines. However, no follow-up results are reported in any of the studies reviewed.
Although randomized control trials with evidence level A2 are preferred to prove the effect of motor training, no RCT at this level was found. In addition, the number of intervention studies on arm and hand functioning in persons with C-SCI is limited anyhow and might be explained by several factors. Firstly, patients with C-SCI have, among the total population with SCI, the most secondary problems leading to frequent drop-out, reduced compliance and fewer adherences to trial training specifications. Secondly, these patients are difficult to match due to the complexity of the pathology and the many determinants that have to be taken into consideration (24). Thirdly, ethical prerequisites often make it difficult to put together a control group and many patients often prefer to participate only in the (experimental) intervention group (24). Fourthly, both in SCI and non-SCI, arm and hand functioning is a complex issue (66). It encompasses a wide variety of highly non-cyclic movements, which are not always easy to objectify, especially at the activity level (14). Changes in AHSP are often very small and most test batteries are not responsive enough to detect these small changes. However, recent developments on the evaluation of AHSP in persons with C-SCI have led to improvements in objectifying rehabilitation outcome, sparking further research in this domain (12, 20, 21).
Next to the limited number of studies related to arm hand functioning in C-SCI, the studies included in this review demonstrate a wide variety in approach. The studies included are very diverse regarding population, time since injury, methodology, training programme and outcome parameters, making any meta-analysis on the results of the studies extremely difficult.
Most studies reviewed demonstrate an improvement in arm and hand functioning at function and/or activity level. But, as different training modalities, training levels and outcome measurements were targeted in different studies, one cannot draw definitive conclusions about the superiority of training programmes.
However, some considerations should be taken into account. In the past much attention was paid to the ICF function level, with training, evaluation and outcome targeted at this level. More recently, patients’ performance at activity level and participation level has substantially gained interest, both in medical treatment as well as in research (26). As to the description of motor training programmes, the function level oriented training programmes were mainly better described regarding training modalities. In contrast, the content of training programmes at the level of activity and the reported conventional therapy programmes were often rather inexplicitly formulated, with the exception of the MP training in the studies of Beekhuizen & Field-Fote (54, 55) and Hoffman & Field-Fote (65). More detailed information on training modalities at activity level, would contribute to better understanding of rehabilitation programmes.
As to outcome of motor training programmes, in general improvement in functioning was reported regarding the level that was trained on. In the studies that contrasted and/or combined training programmes and outcome measurement on different ICF levels, no automatic transfer of effects from one to the other level or generalization was observed. For example, in the studies of Beekhuizen & Field-Fote (54, 55), an improvement in hand activity is reported in the MP group (training focused mainly on hand activities), but no improvement is demonstrated on pinch force (function level). In addition, no improvement in upper extremity activity, as measured by the WMFT, was demonstrated (54, 55). For the MP combined with SS group (training on activity and function level) an additional improvement on function level was reported (55). These results suggest the importance of the specificity of the training, not only for a certain ICF level but also for certain activities, which is in accordance with general principles of training and motor learning (27, 28, 49, 67).
The combination of the specificity of the training and the complexity of arm and hand functioning, including a wide variety of different activities, may lead to the question as to which activities should be prioritized to be trained as it is impossible to train them all. A solution can be found in a client-centred approach taking into account patients personal needs and wishes (68, 69). This approach guides therapists to better decision-making and therapy planning.
According to principles on motor learning, a good training programme should be aimed at establishing a transfer from the trained skills or improved functions into daily life (48) in such a way that the improvement may persist. However, none of the included studies reported a follow-up result. Therefore, it cannot be concluded that these programmes induced a better arm hand functioning in daily life. A client-centred approach, in which patients’ individual needs are trained might accommodate the former principles. Training patients’ individual goals related to arm and hand functioning may facilitate the carry-over into daily life and may further optimize rehabilitation outcome. Future research should focus on this.
In the present study the outcome of motor training programmes aimed at improving arm and hand functioning are reviewed according to different ICF levels. Several of the studies included reported motor training programmes in combination with other therapy modalities, such as FES, biofeedback, NMS and SS. In the study incorporating FES, biofeedback and NMS no significant difference was found between different groups (57, 59–61, 63). In contrast, in the studies reporting on SS, groups receiving SS demonstrate significantly more improvement for some outcome measures (55). However, it is beyond the scope of the present review to infer on final conclusions regarding the effectiveness of the additional therapy modalities. One should be aware that, although such other therapy modalities can be used in conjunction with a motor programme, future research is needed to obtain more insight into the possibilities and the underlying mechanisms of such interventions.
One final consideration is that, although the ultimate goal of training programmes on arm and hand functioning is to facilitate reintegration of patients at the ICF level of participation and to improve quality of life, none of the studies included made a transfer from function or activity level to participation level. Such approaches would be truly comprehensive.
CONCLUSION
This review demonstrates that motor training may improve arm and hand functioning in C-SCI persons at the function and activity level according to the ICF. In view of the complexity of arm and hand functioning and the need for specificity of training, clinicians and therapists should aim at improving individual goal-setting. Furthermore, researchers and clinicians should aspire to perform long-term follow-up measurements, as these results may provide better insight into the translation of improved outcome into better arm hand functioning in daily life.
REFERENCES