OBJECTIVE: It is known that patients in the intensive care unit show an enormous loss of muscle mass. Neuromuscular electrical stimulation is effective in enhancing strength and endurance in immobilized patients. The aim of this study was to evaluate the effects of neuromuscular electrical stimulation on muscle layer thickness of knee extensor muscles in intensive care unit patients.
DESIGN: Randomized, controlled, double-blind, pilot trial.
Patients: Thirty-three patients, male to female ratio 26:7, mean age 55 years (standard deviation 15).
METHODS: After enrolment in the study, intensive care unit patients (main diagnoses: polytrauma, cardiovascular diseases, transplantation, pneumonia, cancer) were stratified (based on the length of their stay in hospital) into 2 groups: 17 acute patients (< 7 days) and 16 long-term patients (> 14 days). Both groups were randomized to a stimulation group or a sham-stimulation group. Neuromuscular electrical stimulation was applied to knee extensor muscles for a period of 4 weeks (session time 30–60 minutes, 5 days/week). Ultrasound measurements were performed before and after the stimulation period to quantify muscle layer thickness of knee extensor muscles.
RESULTS: Only stimulated long-term patients (+4.9%) showed a significant (p = 0.013) increase in muscle layer thickness compared with sham-stimulated patients (–3.2%).
CONCLUSION: Neuromuscular electrical stimulation appears to be a useful adjunct to revert muscle wasting in intensive care unit long-term patients; however, larger studies with a larger sample size are needed to confirm these promising, but preliminary, results.
Key words: neuromuscular electric stimulation; muscle wasting; intensive care; diagnostic ultrasound; muscle layer thickness.
J Rehabil Med 2010; 42: 593–597
Correspondence address: Wolfgang Gruther, University Department of Physical Medicine and Rehabilitation – AKH, Währingergürtel 18–20, Vienna, AT-1090 Austria. E-mail: wolfgang.gruther@meduniwien.ac.at
Submitted July 15, 2009; accepted March 1, 2010
INTRODUCTION
Advances in the management of intensive care unit (ICU) patients have improved outcomes and survival rates for this patient population (1, 2). As more patients survive acute illness, long-term complications become more apparent, some possibly leading to major disability, longer stays in intensive care and protracted rehabilitation (3–8).
Muscle wasting is one of the common problems with which ICU patients are confronted (9–12). A recent study (13) discovered, by means of ultrasound measurements, that muscle mass loss in ICU patients is considerably higher than in all other patient populations, especially in the first 2–3 weeks (14–19).
Early physical and occupational therapy in ICU patients is a recent field of research and published data is as yet scarce (20, 21).
Percutaneous neuromuscular electrical stimulation (NMES) has become clinically established as a method to induce skeletal muscle growth as well as to enhance strength and endurance capacity for patients who are not able to perform active exercise; thus it could be a promising way to prevent muscle mass loss (16, 22–25). Two recent studies revealed promising results for short-term NMES on skeletal muscle metabolism and muscle layer thickness in critically ill patients (26, 27). The studies could not give any information about measurable changes in skeletal muscle mass or muscle strength in long-term ICU patients.
For the purpose of evaluating the muscle structure of human thigh and leg muscles, various equally accurate imaging techniques can be employed, for example computed tomography (CT), magnetic resonance imaging (MRI) or ultrasound (28–30); however, only ultrasound measurements have been tested in diverse patient populations and proven to be a valid and practical measurement tool to document muscle mass (e.g. muscle layer thickness) in the daily routine for ICU patients (13, 26, 31).
The pilot study presented here was conducted in order to evaluate the potency of NMES in: (i) retarding muscle mass loss when applied early for ICU patients; and (ii) reverting muscular atrophy in long-term ICU patients. A larger study was planned as a follow-up, including a power analysis based on the presented data if results seemed to be promising.
METHODS
All the procedures described in this study were approved by the local ethics committee (No. 037/2004), and informed consent was obtained from all patients or by proxy. The study was conducted at the ICU – Department of Anesthesiology and Intensive Care, General Hospital of Vienna, Medical University of Vienna.
Study design
Randomized, controlled, double-blind, pilot trial of NMES with Compex-Sport-P (Medi-Konzept GmbH, Wiesbaden, Germany) or sham stimulation.
To determine the effects of NMES on acute and long-term ICU patients, the study population was stratified into 2 groups based on their immobilization period in the ICU. Two sub-units of the same ICU were chosen (same patient collective but separate locations) for recruitment of an acute patient group (the time between their arrival at the ICU and the beginning of the NMES therapy had to be less than 1 week) and a long-term patient group (the time between their arrival at the ICU and the beginning of the NMES therapy had to be longer than 2 weeks). The different starting point for the NMES therapy of the ICU patients was chosen because of the logarithmical progress of muscle loss, as discovered in a recent study (13). After splitting patients into an acute patient group (AP) and a long-term patient group (LP), randomization into a stimulation group (SG) and a sham-stimulation control group (CG) was performed.
Study population
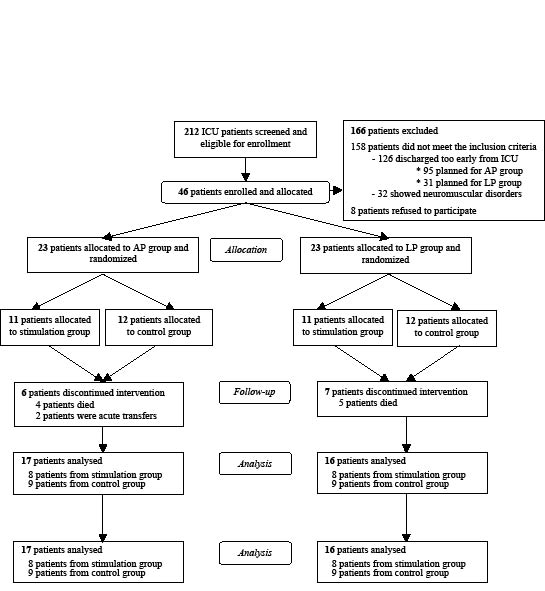
Forty-six patients (Table I and Fig. 1), men and women, all older than 19 years and with severe disorders, were enrolled in the study.
| Table I. Baseline characteristics of acute and long-term intensive care unit (ICU) patients |
| | Acute patient group | Long-term patient group |
| SG | CG | SG | CG |
| Sex male/female, n | 7/1 | 8/1 | 7/1 | 4/4 |
| Age, years, mean (SD) | 52 (10) | 48 (12) | 61 (10) | 64 (8) |
| Height, m, mean (SD) | 1.77 (0.08) | 1.8 (0.06) | 1.78 (0.08) | 1.67 (0.1) |
| Weight, kg, mean (SD) | 80 (15) | 88 (19) | 91 (17) | 79 (19) |
| Body surface, m², mean (SD) | 2 (0.2) | 2.1 (0.3) | 2.2 (0.3) | 1.9 (0.3) |
| Days before stimulation, mean (SD) | 3 (2) | 4 (2) | 33 (15) | 27 (15) |
| MLT at baseline, mean (SD) [range] | 28.9 (6.6) [20.6] | 32.9 (9.7) [23.1] | 18.4 (4.2) [13.6] | 18.6 (5.9) [15.7] |
| MLT after 4 weeks, mean (SD) [range] | 18.3* (3.2) [9.7] | 20.1† (5.4) [16.4] | 19.3‡ § (3.8) [12.4] | 18 (5.8) [16.1] |
| Individual differences (baseline – after 4 weeks), mean | –10.6 | –12.8 | 0.09 | –0.04 |
| % changes from baseline | –36.7 | –38.9 | 4.9 | –3.2 |
| Main diagnosis, n | | | | |
| Polytrauma | 3 | 4 | 2 | 1 |
| Cardiovascular disease | 2 | 2 | 1 | 1 |
| Transplantation | 2 | 1 | 2 | 2 |
| Pneumonia | 0 | 1 | 1 | 2 |
| Cancer | 1 | 1 | 2 | 2 |
| *p = 0.002, †p < 0.001, ‡p = 0.036, within-group comparison; §p = 0.013 between-group comparison. SD: standard deviation; SG: stimulation group; CG: control group; MLT: muscle layer thickness. |
Fig. 1. Trial profile. Consort E-flowchart.
AP: acute patients; LP: long-term patients; ICU: intensive care unit
Exclusion criteria were as follows: stay at the ICU shorter than 14 days, highly trained athletes (muscle layer thickness total > 10 cm), implantable cardioverter defibrillators, neuromuscular disorders, myopathy, paresis of the stimulated muscles, epilepsy, allergic reactions to the electrodes, peripheral oedemas counteracting NMES, heavy ischaemia of the lower extremities, obesity with a body mass index (BMI) > 30, incisions or open wounds on the leg that might be stressed.
Treatment
Patients received either verum treatment (NMES) or sham treatment. Each patient received 1 session a day, 5 sessions a week for a period of 4 weeks.
For the NMES stimulation we used Compex-P devices producing biphasic symmetric impulses with a 50 Hz frequency, a pulse width of 0.35 ms (stimulus regime: 8 s on/24 s off; 30 min/day in the first week, increased to 60 min/day in the second week) and a patient-adjusted intensity to ensure a maximum tolerable tetanic contraction of the M. quadriceps femoris. For sham stimulation the current was only increased until the patient could feel a tingling sensation and no muscle contraction was visible or palpable (27).
The device provided 4 output channels with the possibility to adjust intensity. It was effected via self-adhering surface electrodes (2” × 2” and 2” × 4”, Compex, Medi-Konzept GmbH). To stimulate the quadriceps muscle, the electrodes were placed bilaterally, medially and laterally, 3 cm proximal to the upper border of the patella and 5 cm distal to the inguinal fold.
Outcome measurement
To detect muscle wasting in ICU patients, muscle layer thickness of the quadriceps femoris muscle (M. vastus intermedius and M. rectus femoris) was measured by high-resolution real-time ultrasonography at well-defined points, as described in other studies (13, 14, 17).
Several measuring parameters have been described for documenting muscle mass with ultrasound (13, 17, 19, 32). In the study presented, muscle layer thickness of the M. quadriceps femoris was used to document muscle wasting because: (i) it is well-described (13–15, 17–19, 26) and easy to determine even in highly reduced muscle architecture; (ii) the M. quadriceps femoris is important in the remobilization process because it flexes the hip and extends the knee simultaneously (33) while standing up; and (iii) there is a proven relationship between strength and muscle thickness of the human quadriceps femoris muscle (32, 34, 35).
Muscle layer thickness of the M. vastus intermedius and M. rectus femoris was assessed bilaterally: (i) at the border between the lower and upper two-thirds; and (ii) in the middle of the distance between the anterior superior iliac spine and the upper pole of the patella, with the patient in the supine position and the legs relaxed lying flat in extension. Mean muscle layer thickness (MLT) was calculated by obtaining the mean of the 4 measurements (measuring point 1 and 2 on both legs). The coefficient of variation for a single muscle layer thickness measurement is close to the 3% obtained by other studies (15, 31). MLT measurement used in the 33 patients included in the study presented improves the coefficient to 0.25%.
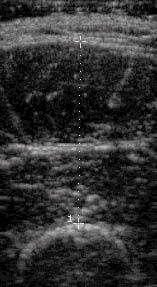
All the ultrasound examinations were performed on a portable ATL ultrasound system (HDI-1000), using a L7-4 transducer with a 5 cm linear array footprint (see Fig. 2), by a single operator who was blinded to the randomization and not involved in the further data analysis.
Fig. 2. Transverse image of the anterior aspect of the M. vastus intermedius and M. rectus femoris.
Statistical analysis
Data was analysed using Statistical Package for Social Sciences (SPSS 17 for Windows). Descriptive statistics were calculated and an unpaired t-test was used to compare the 2 groups (e.g. MLT in SG and CG). A paired t-test was used to compare variables at 2 time points (e.g. MLT measurement at baseline evaluation and at follow-up). The null hypothesis was rejected when p < 0.05.
The study presented was intended as a pilot study with a small study population sample and no intention-to-treat-analysis.
RESULTS
Forty-six patients were enrolled and 33 patients completed this pilot study. No patient withdrew their consent and no adverse events occurred.
Table I shows MLT total at baseline measurement and at the follow-up 4 weeks later, as well as muscle layer change between these 2 time-points, presented as individual differences. Between-group comparison between acute patients with NMES and their control group did not show statistically significant differences in MLT decrease (p = 0.457). In contrast, a significant difference in MLT (p = 0.013) was detected in the comparison of long-term patients with NMES and the CG.
Within-group comparison showed a statistically significant decreased MLT after 4 weeks in acute patients with NMES (p = 0.002) as well as in their control group (p < 0.001). In long-term patients, MLT increased significantly with NMES (p = 0.036), but remained unchanged in the control group (p = 0.162).
DISCUSSION
To summarize, both AP groups (verum NMES treatment and sham treatment) showed a significant loss of muscle mass. The LP group stimulated with NMES showed a significantly higher MLT in contrast to the LP controls.
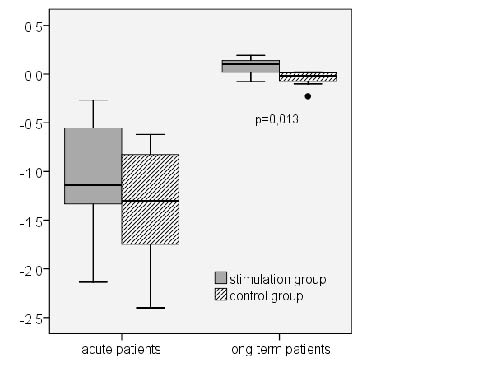
The promising findings of Strasser et al. (27) and Gerovasili et al. (26), applying short-term NMES for critically ill patients, could be affirmed for the long-term group but not for the acute patient group (26, 27). In long-term patients, NMES showed significant positive results (p = 0.013) (Fig. 3). In 6 of our 8 patients measurable muscle growth could be found. In the control group MLT stayed at the baseline level or showed slight, but not significant, muscle mass loss and was similar to levels described in recent studies (13). Recently admitted ICU patients treated with NMES showed a slightly, but not significantly, lower decrease of MLT compared with the control group (see Table I). In relation to the enormous rates of muscle wasting (~40%) in acute patients, with or without NMES, it is questionable whether the observed differences are clinically relevant, even if significant changes are shown in a larger follow-up study.
Fig. 3. Absolute difference (cm) in muscle layer thickness in stimulated patient and control groups (minimum value; 25th, 50th, 75th percentiles; maximum value).
In the pilot study presented, the observed loss of MLT was considerably higher than in all other patient collectives or healthy subjects in bed rest experiments, examined using ultrasound (13–19). Related to these data, the enormous rates of muscle wasting in ICU patients cannot be explained by bed rest at the ICU alone, rather it appears also to be a consequence of the patient’s disease and its treatment.
Establishing a study-setting in an ICU in order to be able to observe ICU patients over several weeks is difficult because of the high turn-over, hospital bed allocation and morbidity of ICU patients, especially when not only patients with high survivability are included. Most of the initially eligible patients (126 of 166) had to be excluded because their anticipated discharge from the ICU was sooner than the minimal required stay at the ICU of at least 14 days, and 13 of the 46 patients who were included could not complete the study and had to be excluded (see Fig. 1); however, distribution in the 4 patient groups was equal and the drop-out rate was similar to that in the study by Gerovasili et al. (26).
The pilot study presented here is not able to provide any information about muscle strength in ICU patients because measurement of strength is not feasible in sedated ICU patients or a suitable way to document muscle wasting in ICU patients. However, there is a proven relationship between strength and the muscle layer thickness of the human quadriceps femoris muscle (32, 34, 35).
Although this is a pilot study with a small number of patients, these preliminary findings indicate that NMES, with a protocol as used in this study, could be an effective adjunct in the ICU therapy to reverse muscle wasting in long-term patients and can support exercise therapy. Larger studies with a larger sample size and different stimulation protocols are needed to confirm these preliminary data.
Further research should: (i) aim to identify the main factors affecting muscle wasting in ICU patients; (ii) include short-term and long-term ICU patients; and (iii) investigate further effects of NMES in critically ill patients after ICU discharge in adjunction to physiotherapy. Special rehabilitation methods for ICU patients need to be developed in order to slow muscle wasting.
ACKNOWLEDGEMENTS
We would like to thank Dr R. Völker (Medi-Konzept GmbH) for supporting our study with COMPEX Sport-P devices and electrodes. This pilot study was performed at the Joint and Bone Center (Center for Diagnosis, Research and Therapy of Musculoskeletal Disorders), Vienna Medical University.
REFERENCES