OBJECTIVE: To assess the prevalence of impairments and evaluate the relationships between impairments, activity limitations and participation restrictions in people affected by leprosy living in The Netherlands.
DESIGN: A cross-sectional study.
SUBJECTS: Eighty-two people affected by leprosy living in The Netherlands.
METHODS: A postal questionnaire was performed. Impairments were inventoried with the Total Impairment Score. Activity limitations were assessed with the World Health Organization Disability Schedule II (WHODAS-II) and participation restrictions with the Impact on Participation and Autonomy (IPA) questionnaire.
RESULTS: A high prevalence of impairments was found (83%), mostly in hands and feet. Activity limitations were substantial, and highest for the WHODAS-II domains “household/work” and “getting around”. The severity of impairments correlated significantly with activity limitations. Eye and foot impairments independently contributed to the domains “household/work” and “getting around”, explaining 34% and 40% of variance. Poor or very poor participation (IPA) was reported by 13–32% of persons, mostly in the “autonomy outdoors” and “family role” domains. These domains were associated with activity limitations and hand impairments
CONCLUSIONS: People affected by leprosy in The Netherlands encounter limitations in activities and participation restrictions, which are related to the severity of impairments. The high prevalence of disability suggests rehabilitation care should be considered for a substantial proportion of people affected by leprosy.
Key words: activities of daily living; disabled persons; leprosy; personal autonomy.
J Rehabil Med 2010; 42: 536–543
Correspondence address: Frederik J. Slim, Department of Rehabilitation, Academic Medical Center, PO Box 22660, NL-1100 DD Amsterdam, The Netherlands. E-mail address: f.j.slim@amc.uva.nl
Submitted July 19, 2009; accepted March 20, 2010
INTRODUCTION
Like other European countries with former colonies, The Netherlands has inhabitants with longstanding impairments of leprosy. A large majority of people affected by leprosy living in The Netherlands originated from Surinam and Indonesia (1). Infiltration of Mycobacterium leprae into Schwann cells results in inflammation of the nerves, which can lead to a progressive loss of nerve fibre function (defined as neuropathy) mostly in the eyes, hands, and feet. Loss of sensory, motor, and autonomic nerve function results in loss of thermal, nociceptive, and pressure senses; muscle pareses; and dryness of the skin (2, 3). Nerve dysfunction can lead to more severe impairments, such as wounds, clawing and shortening of digits, and visual impairments that are often indicated as World Health Organization (WHO) grade 2 disabilities (4). These grade 2 disabilities are reported in up to 26% of newly detected leprosy patients (5). Leprosy is still a major public health problem in several leprosy endemic countries, with a worldwide prevalence of 212,802 patients at the beginning of 2008 (5).
As a consequence of impairments, people affected by leprosy may experience limitations in activities of daily living (2, 6). To date, there is little insight into the impact of leprosy impairments on daily activities and social participation. Most studies have been performed in leprosy endemic countries and have focused only on impairments (7, 8). An international, multicentre study (in Brazil, China, India, Israel and Nigeria), in which an activity limitation questionnaire was used, showed a consistent increase in activity limitations with age and increased level of impairments (9). Participation problems have been reported in leprosy endemic countries by a limited number of studies (6, 10–13). In China, participation restrictions were reported in up to 54% of patients (13).
Current care for leprosy patients at the Academic Medical Center (the main referral centre for leprosy patients in The Netherlands) focuses on the treatment of leprosy and the resulting impairments. To what extent persons affected by leprosy also experience limitations in activities and perceive participation restrictions is not well known, as these specific issues receive only limited attention in treatment protocols.
The aims of this study were: first, to describe the prevalence of impairments in a cohort of persons affected by leprosy living in The Netherlands; secondly, to investigate perceived limitations in activities and participation restrictions; and, thirdly, to study the relationship between impairments and perceived limitations in activities and restrictions in participation.
METHODS
Design and sample
After approval by the local ethics committee, a cross-sectional survey was used to collect information on persons affected by leprosy from the outpatient clinic of the Department of Dermatology at the Academic Medical Center in Amsterdam, The Netherlands. Inclusion criteria were: diagnosis of leprosy according to the Ridley and Jopling classification (1966), having attended the department between 1990 and 2008 (this period was chosen due to the availability of digital data and likelihood of contacting patients), and a minimum age of 18 years at the start of the study. A total of 205 persons affected by leprosy were identified and, after checking address details, questionnaires were sent to the 138 persons who could be located.
Protocol and assessments
Three different questionnaires were used to assess impairments, activity limitations and participation restrictions. A cover letter and all questionnaires were sent with a stamped, addressed envelope and a reply coupon to indicate whether a person was willing to participate. For those who did not return the questionnaires, 2 repeat mailings were sent in order to maximize the response rate. Respondents were instructed to answer the questionnaires themselves or to get help from others, if needed. Data were recorded as part of a larger, cross-sectional study on the consequences of leprosy impairments.
Leprosy impairments. This was assessed using a purpose-designed questionnaire, as an appropriate, self-administered instrument to assess leprosy-related impairments did not exist. Items of the Eye, Hand, Foot score form (EHF) (14) were translated into Dutch and transformed into a self-reporting questionnaire. This questionnaire was reviewed by 2 field experts and subsequently adapted after it was tested in a pilot study. Items assessed included eye, hand, and foot impairments caused by leprosy with a range of severity, including loss of sensibility, visual loss, impaired muscle strength, deformities of digits or toes, history of foot ulceration, and use of prescribed footwear (Appendix I). The respondents scored the presence (yes or no) of impairments (present or past) on eyes (6 questions), hands (12 questions), and feet (19 questions). The left or right side was disregarded. Based on these scores, eye, hand, and foot impairments were classified as none (score 0), mild (score 1), or severe (score 2) according to clinical criteria. A score of 0 was used for no visible deformity or impairments, which could also be considered as non-leprosy specific. Solitary reports of dry feet, skin cracks, callus, blisters, joint stiffness, impaired muscle strength, surgery, podiatry care, or visual impairments were considered as leprosy non-specific and scored as 0. A score of 1 was used for the presence of neuropathy (reported solitary or in combination) or the presence of a combination of primary impairments. Because we were aware of the limitations of self-reported data, a combination of primary impairments (which could also be considered as non-leprosy specific) was needed to score 1. A combination of at least 4 of these non-specific impairments in the absence of loss of sensibility was scored as 1. A score of 2 was given for visible deformity or damage. Secondary impairments (ulcers, burns, inflammation, eye lesions, shortening of digits, orthopaedic footwear, and amputation) reported solitary or in combination were scored as 2. This resulted in the impairments score (IS) for eyes, hands as well as feet (minimum 0, maximum 2). The maximum IS for eyes, hands, and feet were added up (minimum 0, maximum 6) in the Total Impairment Score (TIS). A TIS of 0 or 1 was considered as no or mild (non-leprosy) impairments, a TIS of 2 or 3 as moderate leprosy impairments, and a TIS of 4–6 as severe leprosy impairments.
Perceived limitations in activities of daily living. This was assessed with the Dutch version of the World Health Organization Disability Assessment Schedule II (WHO-DAS II). The WHO-DAS II is a validated, multidimensional questionnaire, which is applicable across cultures and is conceptually compatible with the framework of the International Classification of Functioning, Disability and Health (ICF) (15). The questionnaire includes 36 items, addressing 6 domains: understanding and communicating, household/work activities, self care, getting around, getting along with others, and participation in society. The domains “household/work activities”, “self care”, and “getting around” were considered as activity specific domains, and only data of these 3 domains and the total score was used. The domain “household/work activities” includes household and work items, and for participants without work this domain was only based on household activities. Items focused on difficulties in everyday life encountered within the last 30 days and were scored using a 5-point Likert-scale (“no difficulties” up to “extreme difficulties/not possible at all”). Raw scores were translated to a scale from 0 to 100, using an SPSS syntax (available through the WHO). Low values indicated good performance.
Perceived restrictions in participation and autonomy. This was examined using the Impact on Participation and Autonomy (IPA) questionnaire, which addresses 2 different aspects of participation. The first part of this validated, generic questionnaire is focused on individual’s perceptions of participation and autonomy using 31 items in 5 domains reflecting different life situations: autonomy indoors, family role, autonomy outdoors, social relations, and work/education (16, 17). The respondents graded their perceived participation and autonomy on a 5-point Likert-scale, where “0” indicated “very good” and “4” indicated “very poor”. For each domain, a standardized mean score was calculated (standardized mean equals the mean of the domain score divided by the number of items in the domain). Higher scores indicated greater restrictions in participation. Secondly, the IPA also measures the personal burden of perceived participation restrictions. The perceived problems with participation were assessed on 8 subscales (mobility, family role, self care, finances, leisure, social relations, helping and supporting, and work/education) and rated on a 3-point scale, where “0” indicated no problem and “2” indicated severe problems.
Statistical analysis
For the IPA and the WHO-DAS II, at least 75% of a domain needed to be completed for inclusion in the analysis. Missing items were excluded from scoring in both the numerator and denominator of both the IPA and WHO-DAS II scores. When questions related to work and education were not applicable they were left out of the analysis according to the instructions of the IPA and WHO-DAS II. Study group characteristics were analysed using descriptive statistics. Mean (standard deviation; SD) or median (25th and 75th percentile) scores were calculated for all IPA domains and for the WHO-DAS II sum score and 3 activity domains.
Associations between severity of eye, hand and foot impairments and the perceived limitations in the activity domains of WHO-DAS II scores were investigated using the Pearson’s correlation coefficient. The independent contribution of impairments to perceived activity limitations was explored using multiple linear regression analysis. Furthermore, the independent contribution of impairments and activity limitations to participation was explored using multiple linear regression analysis. Only the variables with a univariate p-value < 0.1 were entered in a multiple stepwise linear regression analyses. Residual analysis was performed to search for violations of necessary assumptions in multiple regression in terms of linearity, equality of variance, independence of error, normality, and influential data points (Cook’s distances). Statistical analysis was performed using SPSS version 16.0.2.
RESULTS
Participants
Ninety-eight persons affected by leprosy responded. Of these, 82 completed the questionnaires (response rate of 59%) and 16 were not willing to participate. Forty persons did not respond. Age was the only significant difference between the responders to the questionnaire and the non-responders (mean age 58.9 years vs 52.0 years, p = 0.007) (Table I). No significant difference was found in the distribution of leprosy type between responders and non-responders (Table I). The majority of both responders and non-responders had borderline tuberculoid (BT) or borderline lepromatous (BL)type leprosy. Forty-two percent of the responders had a partner (married/living together) and 54% were single (5% missing). Thirty-nine percent persons were employed and 55% were unemployed (6% missing). The responders had 12.2 years (SD 6.4) of education. Self-reported general health was good/very good in 39%, moderate in 40%, and poor/very poor in 12% of the responders (9% missing).
| Table I. Subject characteristics |
| Characteristics | Responders | Non-responders |
| Total, n | 82 | 54 |
| Age, years, mean (SD) | 58.9 (14.7) | 52 (14.2)* |
| Sex, male/female, n (%) | 51/31 (62/38) | 29/25 (54/46) |
| Leprosy classification, n (SD) TT BT BB BL LL AL PN missing | 7 (8.5) 31 (37.8) 0 (0.0) 30 (36.6) 8 (9.8) 3 (3.7) 1 (1.2) 2 (2.4) | 12 (22.2) 11 (20.4) 2 (3.7) 16 (29.6) 5 (9.3) 5 (9.3) 0 (0.0) 3 (5.6) |
| *p-value < 0.05. SD: standard deviation; TT: tuberculoid leprosy; BT: borderline tuberculoid leprosy; BB: mid-borderline leprosy; BL: borderline lepromatous leprosy; LL: lepromatous leprosy; AL: arrested leprosy; PN: pure neuritic leprosy. |
Leprosy impairments
Impairments (impairment score of at least 1) of the eyes, hands, and feet were reported by 41%, 68% and 82%, respectively, of the respondents (Table II). Combined hand and foot impairments were reported by 43.9% and combined foot and eye impairments were reported by 26.8% of the respondents. Combined hand and eye impairments were not reported, and combined eye, hand and foot impairments were reported by 1.2% of persons.
| Table II. Impairment score of eye, hand and foot in people affected by leprosy |
| Category | Score | Frequency n (%) |
| Eye | 0 1 2 | 49 (60.5) 12 (14.8) 21 (25.9) |
| Hand, missing n = 1 | 0 1 2 | 26 (32.1) 22 (27.2) 33 (40.7) |
| Foot | 0 1 2 | 16 (19.8) 18 (22.2) 48 (59.3) |
| Frequency of impairment score (0–2) for eyes, hands and feet: 0 = no impairments, 1 = mild impairments, 2 = severe impairments. |
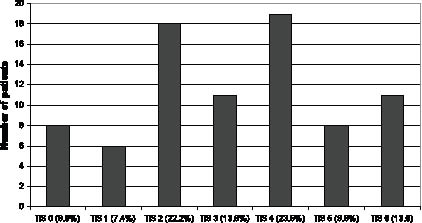
Almost half (47%) of the respondents had a TIS of 4 or more (Fig. 1), which was considered as severe impairments. Eighty-three percent had moderate to severe impairments (TIS ≥ 2). No differences were observed between males and females with regard to the frequency or severity of impairments (TIS) (data not shown).
Fig. 1. Distribution of the Total Impairment Score (TIS) in people affected by leprosy (n = 82). TIS: total sum score (TIS: minimum 0, maximum 6) of the maximum impairment score (range 0–2) for eyes, hands and feet. Data shows the number of patients (%) in the subgroups related to the severity of impairments (TIS).
Perceived limitations in daily activities
The median (p25/p75) of the WHO-DAS II standardized sum score was 26.6 (11.1/49.4). The median scores for the WHO-DAS II activity domains “household/work activities”, “self care”, and “getting around” ranged between 0.0 and 33.3. All 3 WHO-DAS II activity domains correlated significantly with eye and foot impairments, but not with hand impairments (Table III). A significant relation was found between the WHO-DAS II sum score and the severity of impairments TIS (r = 0.52, p < 0.01).
| Table III. Limitations in activities (WHO-DAS II) and the association with impairments |
| WHO-DAS II domains | Descriptive | Univariate association | Multivariate association |
| Median (P25/P75) | Mean (SD) | Eye impairments | Hand impairments | Foot impairments | Independent variable | B | SE | Change in Adj R2 | p |
| Household and work activities | 33.3 (0.0/79.6) | 39.8 (37.5) | 0.52** | 0.15 | 0.46** | Eye Feet | 17.5 14.6 | 4.5 4.9 | 0.27 0.07 | 0.000 0.004 |
| Self care | 0.0 (0.0/40.0) | 22.8 (30.7) | 0.24* | 0.07 | 0.26* | Feet | 11.2 | 4.3 | 0.07 | 0.011 |
| Getting around | 31.3 (3.1/68.8) | 36.5 (32.2) | 0.55** | 0.20 | 0.50** | Eye Feet | 15.5 14.5 | 3.7 4.0 | 0.30 0.10 | 0.000 0.000 |
| *p < 0.05; **p < 0.01.Data are shown as median (P25/P75) and mean (standard deviation (SD)) score for the 3 activity domains of the WHO-DAS II. Impairments = impairments score (0–2) of eyes, hands and feet.Univariate association: Pearson’s correlation coefficients between WHO-DAS II activity domains and impairments are shown. Multivariate association: the independent contribution of eye, hand and foot impairments on activity limitations (WHO-DAS II domains) using multiple stepwise linear regression analysis. Only impairment variables with a univariate p-value < 0.10 were entered in the model to obtain a set of mutually independent determinants. Analysis of results did not show violations of the necessary assumptions in multiple regression in terms of linearity, equality of variance, independence of error and normality. Change in adjusted R2 is the percentage of the variation of the dependent variable score (activity limitations) that is explained by each of the independent variables. Each percentage is adjusted for the variables that are already included in the model. Adjusted R2 (Adj R2) is adjusted for the number of independent variables in the model. SD: standard deviation; SE: standard error; WHO-DAS II: World Health Organization Disability Assessment Schedule II. |
The independent contributions of eye, hand and foot impairments to perceived limitations in the activity domains of the WHO-DAS II are shown in Table III. Eye and foot impairments were independent contributors to the WHO-DAS II domains “household/work activities” and “getting around”, explaining 34% and 40%, respectively, of the variation (Table III). Foot impairments added 10% and 7%, respectively, to the explained variance in these domains after inclusion of eye impairments in the model. Foot impairment was the only independent contributor to the “self care” domain (7%) (Table III). Hand impairments did not contribute to either of the models.
Perceived restrictions in participation and autonomy
The standardized median score ranged between 1.0 and 1.3, indicating perceived participation between good (= 1) and fair (= 2) (Table IV). The highest number of persons reporting participation as poor/very poor was found in the domains “family role” (32%), “autonomy outdoors” (32%), and “work/education” (25%) (Table IV).
| Table IV. Standardized scores of the Impact on Participation and Autonomy Questionnaire (IPA): perceived restrictions in participation |
| | Standardized sum scores | Perceived participation |
| IPA domains | Median (P25/P75) [Range] | Very good and Good n (%) | Fair n (%) | Poor and Very poor n (%) |
| Autonomy indoors (n = 79) | 1.0 (0.0/1.6) [0.0–4.0] | 36 (45.6) | 30 (38.0) | 13 (16.5) |
| Family role (n = 79) | 1.1 (0.6/2.3) [0.0–4.0] | 29 (36.7) | 25 (31.6) | 25 (31.6) |
| Autonomy outdoors (n = 79) | 1.2 (0.6/2.4) [0.0–3.8] | 26 (32.9) | 28 (35.4) | 25 (31.6) |
| Social life and relationships (n = 78) | 1.1 (0.6/1.6) [0.0–3.7] | 28 (35.9) | 40 (51.3) | 10 (12.8) |
| Work and Education* (n = 40) | 1.3 (0.4/2.1) [0.0–4.0] | 14 (35.0) | 16 (40.0) | 10 (25.0) |
| *n = 40 patients indicated that this item was not applicable, and according to the instructions was left out of the analysis. IPA standardized median sum-scores for each domain range between 0 and 4. A score of 0 indicates very good, 1 good, 2 fair, 3 poor and 4 very poor participation and autonomy. Number of patients (%) per category is shown. |
Thirteen to 24% of the respondents experienced severe problems across different areas of participation (Table VI). Severe problems were most frequently reported in “work”, “mobility” (21%), “family role” (20%) and “self-care” (18%). The frequency of severe problems reported increased in relation to increasing severity of impairments in all 9 domains (Table V).
| Table V. Results of Impact on Participation and Autonomy Questionnaire (IPA): severe problems experienced |
| IPA domains | Total group n/total (%) | TIS 0, 1 n/total (%) | TIS 2, 3 n/total (%) | TIS 4–6 n/total (%) |
| Mobility | 16/77 (20.8) | 1/14 (7.1) | 5/25 (20.0) | 10/37 (27.0) |
| Family role | 15/77 (19.5) | 1/14 (7.1) | 2/26 (7.7) | 12/36 (33.3) |
| Self care | 14/76 (18.4) | 1/14 (7.1) | 2/25 (8.0) | 11/36 (30.6) |
| Finances | 12/76 (15.8) | 1/13 (7.7) | 2/26 (7.7) | 9/36 (25.0) |
| Leisure | 12/77 (15.6) | 1/14 (7.1) | 2/26 (7.7) | 9/36 (25.0) |
| Social relations | 11/76 (14.5) | 1/14 (7.1) | 3/26 (11.5) | 7/35 (20.0) |
| Helping & supporting | 10/75 (13.3) | 0/13 (0.0) | 3/26 (11.5) | 7/35 (20.0) |
| Work* | 10/42 (23.8) | 1/12 (7.1) | 4/17 (23.5) | 5/13 (38.5) |
| Education† | 4/31 (12.9) | 0/9 (0.0) | 1/13 (7.7) | 3/9 (33.3) |
| *n = 36 and †n = 39 patients indicated that this item was not applicable, and according to the instructions was left out of the analysis. Data shown are the number and percentage of patients reporting severe problems in various aspects of participation. Data is shown for the total group and in subgroups related to the severity of impairments (TIS). TIS: Total impairment score. TIS 0, 1: no or mild (non-leprosy) impairments, TIS 2, 3: moderate leprosy impairments, TIS 4–6: severe leprosy impairments. |
Three multiple linear regression models were constructed to explore the impact of eye, hand and foot impairments and activity limitations on different domains of participation. The 3 models were chosen on the basis of overlapping contents between participation domains and the 3 domains of activity limitations. The participation model for “autonomy indoors” showed that the activity domain “self care” (22% explained variance), eye impairments (12% added explained variables) and hand impairments (6% added explained variables) were independent contributors. Fifty-four percent of the variation of participation model “autonomy outdoors” could be attributed to the activity domain “getting around” (49%) and hand impairments (5%). For the participation model “family role” only the “household” and not “work activities” of the WHO-DAS II “activity” domain were appropriate for use in this study. Fifty-two percent of the variation of the participation domain “family role” could be attributed to activity domain “house activities”(45%) and hand impairments (6%) (Table VI). Foot impairments did not contribute to either of the participation models.
| Table VI. Independent contribution of the individual impairments and activity limitations on participation (IPA) |
| Dependent variable | Independent variable(s) | Unique contribution |
| IPA domains | B | SE | Change in Adj R2 | p |
| Autonomy indoors | WHO-DAS II: Impairments: | Self care Eyes Hands | 0.012 0.345 0.311 | 0.003 0.101 0.101 | 0.23 0.12 0.06 | 0.000 0.001 0.003 |
| Family role | WHO-DAS II: Impairments: | House activities Hands | 0.020 0.373 | 0.02 0.373 | 0.45 0.06 | 0.000 0.001 |
| Autonomy outdoors | WHO-DAS II: Impairments: | Getting around Hands | 0.022 0.296 | 0.003 0.099 | 0.49 0.05 | 0.000 0.004 |
| WHO-DAS II: World Health Organization Disability Assessment Schedule II; IPA: Impact on Participation and Autonomy Questionnaire. The independent contribution of eye, hand and foot impairments and activity limitations (WHO-DAS II domains) on participation (IPA domains) using multiple stepwise linear regression analysis. WHODAS domains were chosen on the basis of overlap in construct with the dependent variable (IPA domains). Only impairment variables with a univariate p-value < 0.10 were entered in the model to obtain a set of mutually independent determinants. Analysis of results did not show violations of the necessary assumptions in multiple regression in terms of linearity, equality of variance, independence of error and normality. Change in adjusted R2 (Adj R2) is the percentage of the variation of the dependent variable score (participation restrictions) that is explained by each of the independent variables. Each percentage is adjusted for the variables that are already included in the model. Adjusted R2 is adjusted for the number of independent variables in the model. Impairments = impairments score (0–2) of eyes, hands and feet. SE: standard error. |
DISCUSSION
This study shows that daily life activities of people affected by leprosy living in The Netherlands are substantially diminished. Limitations in activities with respect to “mobility” and “household/work activities” were related to leprosy impairments of the eyes and feet. Almost a third of the persons affected by leprosy perceived their participation as poor to very poor, particularly in the domains “family role”, “autonomy outdoors”, and “work/education”. Participation restrictions with respect to family role and autonomy outdoors were related to activity limitations and hand impairments. Severe participation problems were most frequently reported by persons with severe leprosy impairments.
The mean WHO-DAS II sum score in the present study of 31.4 was substantially higher than the score of 12.9 found in healthy subjects and in patients with stroke, systemic sclerosis, and ankylosing spondylitis (range 18.5–23.9) (18–21). This indicates that people affected by leprosy perceive more activity limitations. A significant correlation was found between the severity of impairments (TIS) and activity limitations. The correlation found in this study (WHO-DAS II sum score, r = 0.52) appears to be higher than previously found in India (range r = 0.2 and r = 0.29) and lower than reported by the SALSA Collaborative Study Group (SALSA = Screening of Activity Limitations & Safety Awareness) (r = 0.65) (9, 22). However, different questionnaires were used in those studies, hampering comparisons.
We found that foot and eye impairments contributed significantly to activity limitations, particularly for the WHO-DAS II activity domains “getting around” and “house/work activities”. These findings are in agreement with a Nepalese study in which foot impairments were found to be associated with activity limitations related to the lower limb (6). Despite a high percentage of hand impairments, we did not find a correlation between hand impairments and activity limitations, in contrast to studies in Nepal, India and Israel (22–25). These studies used specific hand activity questionnaires, whereas the WHO-DAS II measures activity limitations in general and not hand activities in particular. The WHO-DAS II may therefore not be sensitive enough to activity limitations resulting from hand impairments. A future study comparing WHO-DAS II with the SALSA scale would be useful to further investigate this observation, since the SALSA scale includes specific items related to hand activities and hand dexterity.
Almost one-third of the people affected by leprosy perceived their participation (IPA) as severely restricted (poor to very poor) in the present study, although the standardized mean score of perceived restrictions in participation was lower than reported in patients with neuromuscular disease, stroke, spinal cord injury and rheumatoid arthritis (17). Because the leprosy infection occurred many years earlier, people had the time to adapt to the increasing impairments and limitations in activities. This adaptation is known as the “response shift” and may contribute to the mildness of the perceived restrictions in participation and autonomy (26). Furthermore, up to 21% of the persons affected by leprosy experienced severe problems with participation in the present study. The severity of participation problems consistently increased with the severity of impairments. Twenty to 33% of the persons with severe leprosy impairments, experienced severe problems with participation, which is lower than reported in studies from Nepal and China with participation restrictions in 40% and 54% of people affected by leprosy, respectively (10, 13). This difference in participation restrictions may be related to several factors, such as environmental differences, which may be less demanding in The Netherlands, and differences in stigma levels, which are lower in The Netherlands compared with Nepal and China (10, 13, 27).
Activity limitations were found to be major determinant of participation restrictions, together with hand impairments. This was shown for the participation domains family role and autonomy outdoors. Activity limitations in combination with eye and hand impairments independently contributed to autonomy indoors. These results indicate that the pathway to participation restrictions runs largely through activity limitations. This suggests that the role played by stigma (as an environmental factor) to participation restrictions may not be so large in the studied population as previously thought. However, it is striking that hand, but not foot, impairments were related to participation restrictions, as the participation domains included items related to both hand and feet. This suggests that stigma contributes towards participation restrictions, as hand impairments are more visible in a social environment than foot impairments. In future studies the role of environmental factors, such as stigma in the pathway to participation restrictions, should be explored further.
The prevalence of impairments in our study seems rather high, although differences in methods of assessment preclude reliable comparisons with other studies. In our study, there are a high number of people affected with BL and BT type leprosy, who have a higher risk of developing impairments (8). Also, many of our former patients came to The Netherlands in search of better medical treatment and may have already been severely affected by leprosy at the time of immigration. Furthermore, the use of self-reporting questionnaires in the current study, compared with impairments scored by health workers (often used in other leprosy studies), could have resulted in an overestimation of impairments.
These results indicate that people affected by leprosy living in non-endemic countries are considerably disabled. People reported a high prevalence of impairments, perceived substantial limitations in activities, and the majority perceived their social participation as restricted. The stigma related to leprosy may lead to delay in seeking timely medical treatment (28), subsequently leading to more (severe) impairments (29). Stigma may also lead to a delay in reporting limitations in activities and participation restrictions. An exploratory study showed (fear of) stigma among people affected by leprosy in The Netherlands, especially within their own community and not so much in Dutch society (27). People may also have insufficient knowledge of the possibilities provided by rehabilitation care in The Netherlands and therefore do not seek help.
Although the number of participants included in the current study is smaller than other leprosy surveys, one of the strengths was the inclusion of treated and clinically stable former leprosy patients throughout the whole clinical spectrum of leprosy. This made it possible to study the long-term consequences of the disease. Most previous studies have focused on impairments and only a few have investigated either the limitations in activities or restrictions in participation of people affected by leprosy (6, 9–13, 22–25). To our knowledge, this is the first study investigating the consequences of leprosy on the 3 ICF domains (body structure/functions, activity and participation) within the same group of people affected by leprosy. Furthermore, in contrast to most studies, the present study mainly used self-reporting questionnaires instead of interview-based questionnaires. Self-reporting questionnaires avoid the risk that the interpersonal setting of an interview might limit disclosure of experiences that were emotionally distressing. We acknowledge that the impairment questionnaire has been only partially validated.
In conclusion, a substantial proportion of people affected by leprosy living in The Netherlands perceive limitations in activities and participation restrictions. To improve daily life activities and social participation, these people may benefit from multidisciplinary rehabilitation treatment. Since impairments are important contributors to limitations in activities and participation restrictions, interventions such as footwear, bodily aids and devices to compensate for these impairments should be considered together with psychological counselling for stigma.
ACKNOWLEDGEMENTS
This study was financially supported by the Netherlands Leprosy Relief/Nederlandse Leprastichting.
The authors wish to thank Dr J.W. Brandsma and Dr. W.H. van Brakel for evaluating the impairments questionnaire and Dr. A. Beelen for technical advice on the questionnaires used, data processing and statistical analysis.
REFERENCES