OBJECTIVE: To evaluate and compare the efficacy of 2 rehabilitation strategies after arthroscopic acromioplasty: supervised physical therapy focusing on strengthening exercises of the rotator cuff and scapula stabilizers (PT-group) vs home-based movement exercises (H-group).
DESIGN: A randomized, single-blinded, clinically controlled study.
Patients: Thirty-six patients entered the study. Thirteen in the PT-group and 16 in the H-group fulfilled all the assessments.
METHODS: For 12 weeks following surgery, patients performed either supervised physical therapy or home exercises. Follow-ups were conducted periodically for 6 months after surgery to evaluate shoulder function, pain (Constant-Murley (CM) and Disabilities of the Arm, Shoulder, and Hand (DASH) scores), and health-related quality of life.
RESULTS: The PT-group exhibited significantly greater improvements in CM (p =0.02) and DASH (p = 0.05) scores. After treatment, the between-group mean difference in CM scores was 14.2 p (95% confidence interval 2–26). At the 6-month follow-up, the between-group mean difference in DASH scores was 13.4 p (95% confidence interval 0.1–23).
CONCLUSION: PT-supervised rehabilitation with strengthening exercises of the rotator cuff and scapula stabilizers seems to be superior to home exercises focusing on mobility for improving shoulder function after arthroscopic acromioplasty.
Key words: arthroscopic acromioplasty; exercise; rehabilitation; rotator cuff; subacromial impingement; physical therapy.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Theresa Holmgren, Department of Medical and Health Sciences, Div. of Physiotherapy, Linköping University, SE-581 83 Linköping, Sweden. E-mail: theresa. holmgren@liu.se.
Submitted December 22, 2010; accepted August 17, 2011
INTRODUCTION
Subacromial impingement syndrome (SIS), defined as shoulder pain due to impingement of soft tissue structures in the subacromial space, is one of the most common forms of shoulder pathology. SIS is present in 44–60% of all patients in primary care with shoulder pain (1, 2); it is associated with shoulder dysfunction, and patients are often unable to work full-time (3). The societal cost is high; patients with shoulder disorders account for 20% of all disability payments for musculoskeletal disorders (4). The first choice of treatment for patients with SIS is conservative, often including corticosteroid injection and/or various physical therapy (PT) interventions (5). When conservative treatment fails, arthroscopic subacromial decompression (ASD) is the standard surgical technique recommended for patients with SIS (6). Well-documented evaluations of the postoperative results have reported 70–80% success rates, regarding improved shoulder function and decreased pain (6–9). Surgery is often combined with postoperative rehabilitation, which probably contributes to these positive results, although studies specifically evaluating the efficacy of rehabilitation following surgery are scarce.
The intention of the surgical procedure is to remove the presumed structural pathology, while the aims of the rehabilitation programme are to restore shoulder function and to prevent recurrence. General post-ASD rehabilitation programmes have been described (10). However, few studies (11, 12) have evaluated and compared different exercise programmes after ASD, and many questions remain regarding which exercises are most effective, PT-supervised or home exercises, in addition to questions about dosage and progression during the rehabilitation period. To date, the evidence is inconclusive and further research is needed. The objective of this study was to evaluate and compare two postoperative rehabilitation strategies: physical therapist (PT)-supervised rehabilitation including progressive strengthening exercises for the rotator cuff and scapula stabilizers vs instructions for home exercises focused on improving mobility (the current practice in participating clinics at the time of study design). Evaluations were made regarding shoulder function, pain, health-related quality of life, and return to work after ASD.
PATIENTS AND METHODS
An observer-blind, randomized clinical trial was conducted.
Participants and setting
Between January 2003 and January 2006, patients were recruited from the orthopaedic departments of a university hospital and a local hospital located in two geographical areas of Sweden. Patients who were scheduled for ASD, ranging in age from 30 to 65 years, were recruited for this study. An orthopaedic surgeon set the following standardized criteria for surgery: a positive impingement test by Neer (local anaesthetic, 10 ml prilocaine in the subacromial bursa), a minimum of 6 months’ duration of pain, no results or unsatisfactory results after at least 3 months of physical therapy, and typical pain location (C5 dermatome). Before inclusion, a radiological examination was performed to differentiate SIS from other diagnoses.
To validate the diagnosis of SIS, a research PT re-examined the patients approximately one week before the date of surgery. This examination included the Neer impingement sign, Hawkins-Kennedy impingement sign, painful arc, and Jobe supraspinatus test. Three positive tests were the criteria for inclusion in the study. Patients were excluded if they had clinically verified shoulder instability, problems in the cervical spine, general neck and shoulder pain, suspected polyarthritis, or symptoms of frozen shoulder, or if they were diagnosed with osteoarthritis of the glenohumeral joint, fracture, fibromyalgia, rheumatoid arthritis, or radiological-verified malignancies. If patients met the inclusion criteria they received verbal and written information about the study from the research PT after the examination.
This study was approved by the ethics committee in Linköping (DNR 02-37).
Trial registration. ClinicalTrials.gov, protocol number DNR02-37.
Randomization and interventions
All patients underwent a similar surgical procedure performed by 1 of 4 orthopaedic shoulder surgeons in the 2 hospitals. Standard antero-inferior arthroscopic subacromial decompression was performed. The surgeon removed part of the subacromial bursa, removed the under-surface of the acromion, and resected the attachment for the coraco-acromial ligament.
After ASD, the patients were consecutively randomized by the PT on the orthopaedic ward to 1 of 2 rehabilitation groups: PT-supervised rehabilitation (PT-group) or instructions for home exercises (H-group). The random allocation sequence was prepared beforehand by an independent PT who concealed equal numbers of treatment alternatives (20 for the local hospital and 40 for the university hospital) in opaque envelopes, which were then sealed, mixed, numbered, and given consecutively to patients directly after surgery.
For the first week after surgery, both groups received the same home exercise programme instructions from the PT at the orthopaedic ward corresponding to current praxis (Appendix I). This initial programme consisted of active supported and active exercises to increase the range of motion in the gleno-humeral joint and stimulate circulation in the muscles around the shoulder. There were 6 exercises (shoulder flexion, abduction, internal rotation, unilateral and bilateral external rotation as movement exercises, and scapula retraction), as well as correction of posture, each to be repeated 10 times, twice a day. Patients were informed that the exercises should be carried out only as long as they did not increase the pain. All patients received instructions that heavy lifting or performing leisure activities that involved lifting the arms above the shoulders were contraindicated for the first 4 weeks after surgery. The 2 rehabilitation strategies differed after the first week.
Exercises in the physical therapy group
Rehabilitation for the PT-group consisted of 4 phases starting after the first week of home exercises, as described below.
Phase 1 (week 2). Correction of posture with retraction and depression of the shoulders. Active supported external rotation, lying on the side. Active movement exercises: shoulder flexion, external rotation, and abduction in order to restore shoulder motion.
Phase 2 (week 3). Isometric strengthening of the rotator cuff muscles and the stabilizers of the scapula with external/internal rotation and abduction with the shoulder in neutral position (0º of shoulder abduction). Dynamic external rotation, performed through the range of motion against gravity, lying on the side. Posterior shoulder stretching.
Phase 3 (week 4–5). Dynamic strengthening exercises of the rotator cuff muscles and the scapula stabilizers (eccentric as well as concentric) using a rubber band and weights. All exercises with external loads were performed with the shoulder in a neutral position. Primary exercises: internal and external rotation, scapula retraction in rowing exercises, and elevation 0–45º in the scapular plane as well as scapula protraction in a press-up. Posterior shoulder stretching.
Phase 4 (week 6–8). Strengthening the rotator cuff and the scapular muscles using a rubber band and weights in different positions (shoulder in 45º of abduction and progression with 90º of abduction), while gradually increasing the load. Primary exercises: internal/external rotation, scapula retraction in rowing exercises and elevation 0–45º in the scapular plane, horizontal shoulder extension in prone as well as push-ups plus. Posterior shoulder stretching.
(Week 9–12). Progression of more complex exercises with increased load, e.g. bilateral external rotation with a rubber band combined with elevation. Exercises were individually designed for patients, taking work situation and leisure-time activities into consideration.
Four PTs, all working in primary care and each with at least 5 years of experience treating shoulder patients, were responsible for this supervised rehabilitation. Exercise sessions were carried out twice weekly for 8 weeks and took approximately 30 min each. Between the supervised rehabilitation sessions, patients were instructed to perform individually-adjusted daily home exercises that followed the phases of the rehabilitation programme. After the initial 8 weeks, patients were instructed to continue the exercises at home until the 3-month follow-up. If a patient was absent from more than 4 exercise sessions, they were regarded as non-compliant with the study protocol, resulting in a minimum of 12 exercise visits. For a more detailed description, see Appendix II.
Exercises in the home exercise group
The H-group continued with the mobility-focused home exercises that both groups were initially instructed in after surgery until the 3-month follow-up, without any additional exercises or progression. Several weeks after surgery, the patients received one telephone call from the PT to encourage compliance. For a more detailed description, see Appendix I.
Outcome measures and follow-up
All primary and secondary outcomes were evaluated by one of the blinded research PTs. Evaluations were conducted before surgery (baseline) and repeated 1 week after surgery, as well as 1, 2, 3, and 6 months after surgery. The following data were documented at the inclusion visit: age, sex, duration of shoulder pain, earlier treatment, medication, occupation, and duration of sick leave. Workloads were assessed by the patients as belonging to 1 of 4 categories: (i) light load (e.g. computer work); (ii) moderate load (e.g. shop assistant); (iii) moderate to heavy load (static work, e.g. hair stylist); and (iv) heavy load (e.g. contruction worker).
To evaluate primary outcomes (shoulder function and pain), the shoulder-specific Constant-Murley Shoulder Assessment Score (CM score) was used (13). The CM score, recommended by the European Society for Surgery of the Shoulder and Elbow, is a value between 0 and 100; a higher score indicates better shoulder function. A previous study demonstrated that the intra-tester reliability of the CM score is high, while the inter-tester reliability was proven to be insufficient (14).
Secondary outcomes were: Disability of the Arm, Shoulder and Hand (DASH) score, which is an instrument developed by the American Academy of Orthopedic Surgeons to evaluate loss of function in the upper extremities (15). The DASH score is based on patient self-assessment with a value between 0 and 100; a lower score indicates better function. The measurement quality of DASH is high regarding reliability, validity, and responsiveness (16, 17). Gummesson et al. (18) concluded that the DASH score was sensitive enough to measure postoperative changes in disability over time in patients with upper extremity musculoskeletal disorders. At each follow-up, the visual analogue scale (VAS) was used to assess the patients’ pain intensity at rest, during arm activity, and at night. The VAS provides a continuous scale for magnitude estimation and consists of a straight line, with no pain (0) at one end and the worst imaginable pain (100) at the other end (19). The European Quality of Life–5 Dimensions (EQ-5D) was used to evaluate self-reported health-related quality of life (HRQoL). EQ-5D is a reliable and valid self-evaluation instrument developed by the EuroQol Group. The results of 5 questions are converted into an index, ranging from –0.59 to 1; a higher score indicates better HRQoL. The EQ-5D has been increasingly used in different clinical areas for patients with musculoskeletal diseases (20).
Data analysis and sample size
A sample size calculation was performed based on the CM score, which was the primary outcome measure. The calculation estimated that a total of 54 patients would be required to detect a 10-point mean group difference (11) with a variability of 13 points (β = 0.80, α = 0.05, 2-sided). Due to reorganization, the study was discontinued before the intended sample size was reached and only 36 patients were included in the study.
To compare independent variables between the 2 groups at baseline, the Student’s t-test was used for continuous data and the χ2 test for categorical data. Changes in continuous dependent variables over time were assessed by repeated measures analysis of variance (ANOVA). Four separate analyses were performed (CM-score, the DASH-score, the EQ-5D, and the VAS); within-subjects factor was time and the between-subject factor was treatment for all 4 analysis. Paired t-test with Bonferroni correction was used for post-hoc analysis. Statistical significance was defined as p < 0.05 for all tests. A change of ≥ 10 as previously suggested was considered to be a clinically relevant change in the CM score between groups (11). The statistical software package SPSS was used (version 17.0; SPSS, Inc., Chicago, IL, USA).
RESULTS
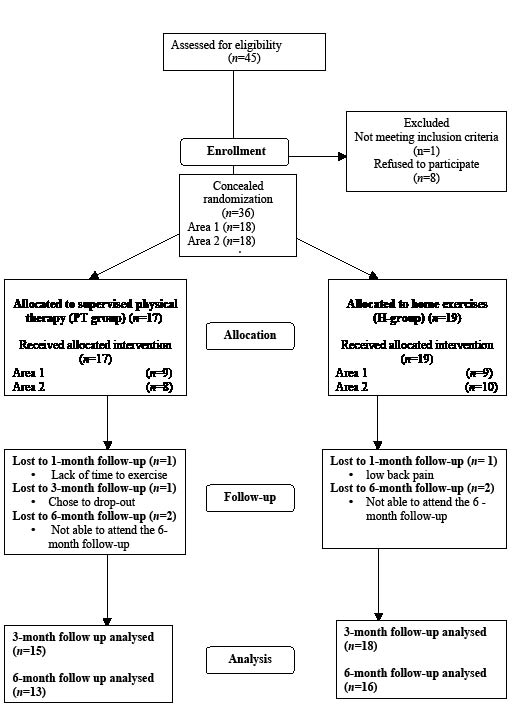
Forty-five patients were scheduled for ASD; 1 was excluded at re-examination due to a frozen shoulder and 8 declined to participate. In total, 36 patients entered the study, 29 of whom completed all required follow-up (Fig. 1). Of the 3 who did not complete the 3-month follow-up, 2 dropped out of the study due to lack of time after the first follow-up. One patient had low back pain and could not continue after 4 weeks. Another 4 patients did not attend the 6-month follow-up, and gave no reasons (Fig. 1). There were no differences in the background variables, except that the PT-group had a higher percentage of dominant affected shoulders compared with the H-group (Table I); nor were there any significant differences in outcome measurements between the groups before surgery (baseline) or one week after surgery (Table II). The work load, assessed by the patients, was similar between the 2 groups (Table III). Background variables for both groups are presented in Table I. Mean scores for all outcome measures and the between-group mean difference at each follow-up, are presented in Table II. The distribution of work load and the number of patients returning to work in both groups are presented in Table III. Patients from the 2 hospitals were equally distributed in the 2 treatment groups. All patients in the PT-group were regarded as compliant with the study protocol and had a minimum of 12 supervised exercise visits.
Fig. 1. Participant flow through the randomized clinical trial.
| Table I. Background variables presented for the supervised physical therapy group (PT-group) and for the home exercise group (H-group), respectively. All in numbers if not stated otherwise |
| | PT-group (n = 15) | H-group (n = 18) | Statistical analysis |
| Gender, men/women, n | 7/8 | 10/8 | NS, Pearson χ2 |
| Age, years, mean (SD) | 51 (10.2) | 55 (7.2) | NS, Student’s t-test |
| Duration of shoulder pain before surgery, months, mean (SD) | 38 (35) | 23 (25) | NS, Student’s t-test |
| Dominant shoulder affected, n (%) | 14 (86) | 7 (44) | p = 0.001, Fischer’s exact |
| Sick-leave before surgery, yes/no, n | 9/6 | 11/7 | NS, Fischer’s exact |
| Duration of sick leave, months, mean (SD) | 18 (33) | 17 (11) | NS, Student’s t-test |
| SD: standard deviation. |
| Table II. Outcome measurements between the supervised physical therapy group (PT) and the home exercise group (H) before and after surgery |
| | Baseline | | 1 week | | 1 month | | 2 months | | 3 months | | 6 months |
| PT n = 15 | H n = 18 | | PT n = 15 | H n = 18 | | PT n = 15 | H n = 18 | | PT n = 15 | H n = 18 | | PT n = 15 | H n = 18 | | PT n = 13 | H n = 16 |
| Outcome measurements |
| CM score | 47 (19) | 45 (20) | | 28 (14) | 30 (21) | | 51 (15) | 45 (21) | | 62 (13) | 54 (21) | 63 (11) | 49 (20) | | 73 (16) | 59 (23) |
| DASH score | 36 (14) | 38 (19) | | 45 (14) | 44 (22) | | 29 (10) | 32 (19) | | 22 (10) | 30 (20) | 16 (10) | 27 (22) | | 12 (11) | 25 (22) |
| EQ-5D | 0.63 (0.26) | 0.52 (0.26) | | 0.55 (0.21) | 0.56 (0.26) | | 0.71 (0.20) | 0.61 (0.24) | | 0.69 (0.16) | 0.65 (0.26) | 0.82 (0.14) | 0.63 (0.28) | | 0.84 (0.19) | 0.74 (0.26) |
| VAS rest | 22 (20) | 29 (27) | | 14 (16) | 17 (19) | | 13 (17) | 9 (14) | | 3 (6) | 6 (14) | 5 (10) | 3 (6) | | 5.5 (9)a | 5.4 (10)a |
| VAS activity | 57 (23) | 54 (26) | | 42 (23) | 42 (22) | | 28 (22) | 28 (22) | | 21 (21) | 25 (19) | 13 (22) | 19 (18) | | 3.1 (9)a | 19 (21)a |
| VAS night | 47 (23) | 37 (31) | | 26 (25) | 26 (31) | | 26 (24) | 19 (27) | | 14 (21) | 12 (18) | 10 (17) | 16 (26) | | 2.6 (5.6)a | 19 (34)a |
| Differences between groups |
| CM score | 2.9 (–12 to 18) | | 2.2 (–15 to 11) | | 6.0 (–7 to19) | | 8.1 (–5 to 21) | 14.2 (2 to 26) | | 13.7 (–2 to 28) |
| DASH score | 1.8 (–15 to 11) | | –1.2 (–13 to 15) | | –3.0 (–8 to14) | | –8.6 (–3 to 20) | –11.1(–2 to 24) | | –13.4 (0.1 to 27) |
| EQ–5D | 0.1 (–0.1 to 0.32) | | 0.01 (–0.19 to 0.17) | | 0.1 (–0.06 to 0.27) | | 0.04 (–0.13 to 0.20) | 0.19 (0.02 to 0.35) | | 0.1 (–0.07 to 0.28) |
| VAS rest | 7.1 (–24 to 10) | | 3.2 (–16 to 9) | | 3.2 (–8 to 14) | | 3.7 (–11 to 4) | 3.0 (–4 to 8) | | 0.19 (–9 to 9)a |
| VAS activity | 2.8 (–15 to 20) | | 0.4(–16 to 15) | | 0.01 (–16 to 16) | | 4.3 (–19 to 10) | 5.3 (–20 to 9) | | 16 (–29 to –3.5)a |
| VAS night | 10 (–10 to 30) | | 0.4 (–20 to 19) | | 6.8 (–11 to 25) | | 7.0 (–12 to 17) | 7.6 (–21 to 9) | | 2.5 (–9 to 14)a |
| aVAS assessed at the 6-month follow-up: H-group n = 14 and PT-group n = 11. CM score: Constant Murley Shoulder Assessment score 0–100 in which 100 is the best shoulder function; DASH score: Disabilities of the Arm Shoulder and Hand score 0–100 in which 0 is the best shoulder function. EQ-5D index 1– (–0.59), in which –0.59 is the lowest health-related quality of life. Pain VAS (visual analogue scale) 0–100 mm, in which 100 is the worst imaginable pain. |
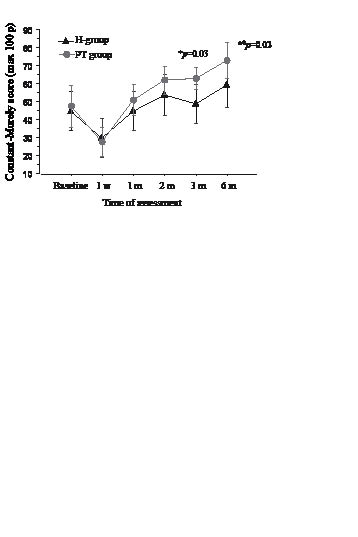
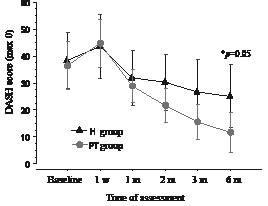
The PT-group had a significantly larger improvement over time in the CM score (p = 0.02); as presented in Fig. 2, they improved from 47.4 at baseline (preoperatively) to 72.8 at the 6-month follow-up, compared with the H-group, which improved from 46.0 to 59.1 (Table II). After completing the treatment period, the between-groups mean difference in CM score was 14.2 p and the PT-group had a significantly larger improvement (p = 0.03) (Fig. 2). The PT-group also had a significantly larger improvement over time in the DASH score (p = 0.05); as presented in Fig. 3, they improved from 36 at baseline (preoperatively) down to 12 at the 6-month follow-up, compared with the H-group which improved from 38 to 25 (Table II). At the 6-month follow-up the between-group mean difference in DASH score was 13.4 p and the PT-group had a significantly larger improvement (p = 0.05). There was no statistical difference in EQ-5D between the groups over time (p = 0.20), both improved. However, at the 3-month assessment there was a significant difference (p = 0.02) between the 2 groups in favour of the PT-group. Both groups reported significantly decreased pain over time (VAS) during rest (p < 0.005), arm activity (p < 0.005), and at night (p < 0.05), but there was no significant difference between the 2 groups (Table II). After 3 months, 10 out of 15 patients in the PT-group had returned to full-time work, compared with 6 out of 18 patients in the H-group. At the time of the 6-month follow-up, one additional patient in each group had returned to work (Table III).
Fig. 2. The mean Constant-Murley score presented with 95% confidence interval at each follow-up, baseline (pre-operative) 1 week, 1, 2, 3 and 6 months after surgery in both groups respectively. Higher score, better shoulder function. *Significant at 3-month endpoint. *aSignificant over time (analysis of variance (ANOVA)). m: months; w: weeks.
Fig. 3. Mean Disabilities of the Arm, Shoulder, and Hand (DASH) score presented with 95% confidence interval at each follow-up, baseline (pre-operative), 1 week and 1, 2, 3 and 6 months after surgery in both groups respectively. Lower score, better shoulder function. *Significant at 6-month endpoint. m: months; w: weeks.
| Table III. Distribution of the patients considering work load in relation to the total number of patients returning to work after 3 and 6 months in the supervised physical therapy group (PT-group, n = 15) and in the home exercise group (H-group, n = 18), respectively |
| Work load (assessed by the patients) | PT-group (n = 15) n | H-group (n = 18) n | Patients returning to work after 3 and 6 months (n) |
| PT-group | | | | H-group |
| 3 months | | 6 months | | 3 months | 6 months |
| Light load | 1 | 6 | 1 | | 1 | | 4 | 4 |
| Moderate load | 6 | 3 | 3 | | 4 | | 1 | 1 |
| Moderate to heavy load | 0 | 2 | 0 | | 0 | | 0 | 1 |
| Heavy load | 8 | 7 | 6 | | 6 | | 1 | 2 |
DISCUSSION
The objective of this study was to compare two rehabilitation strategies for patients who underwent ASD as a treatment for SIS. One strategy involved PT-supervised rehabilitation that was focused on progressive strengthening exercises for the rotator cuff and scapula stabilizers. The other strategy consisted of providing instructions for home exercises, which focused on improving mobility. The results of this study indicate that the PT-supervised rehabilitation produced greater improvements in shoulder function. Progressive rehabilitation was considered to be well-tolerated in the PT-group, since their experienced level of pain was no greater than that of the H-group during the rehabilitation period.
During the design of this study, the praxis of the orthopaedic clinics participating in the study was that, after ASD, patients were instructed to perform home exercises focused on increasing shoulder mobility. We thought that a new rehabilitation strategy should be designed to include two other important components: strengthening exercises for the rotator cuff and strengthening exercises for the scapula stabilizers. This concept is supported by both earlier and later studies evaluating conservative treatment for patients with SIS (21–25), as well as by systematic reviews reporting positive effects of these exercises in patients with SIS (26–29). Some studies have suggested that exercise programmes are as effective as surgical treatment (25, 30). Since weaknesses of the rotator cuff and scapula stabilizers may be additional impinging factors due to increased humeral migration (31–33), exercises to strengthen the rotator cuff and scapula stabilizers seem appropriate also after ASD to avoid recurrence. Since the start of this study, the praxis of the participating hospitals has been adjusted to often include PT-supervised rehabilitation focusing on strengthening exercises for the rotator cuff and scapula stabilizers. The implementation of these strategies is not yet fully supported by evidence.
The results presented in this study are contradictory to those of Andersen et al. (11), where no differences were found between groups when comparing home exercises with PT-supervised exercises in patients 6 months after ASD. The CM score was used as the primary outcome measurement with a 10-point difference between the groups regarded as clinically relevant, but they only observed a difference of 1 point in favour of the home exercise group at the 6-month follow-up. The current study resulted in a larger mean difference (13 points) in the CM score in favour of the PT-group, at the 6-month follow-up. Andersen et al. (11) proposed that their results might have been influenced by the low intensity of their supervised exercise programme, but presentation of the details of the exercises was lacking. One major difficulty faced when comparing patient outcomes after exercises and surgery is that the post-operative treatment is rarely described in detail.
Hultenheim Klintberg et al. (12) recently compared 2 post-ASD supervised rehabilitation programmes, a traditional programme and a more progressive programme. They reported no significant differences between the 2 groups regarding shoulder function or pain after 6 months. However, CM scores improved significantly in both groups, and a mean of 72 was reached after 6 months, which corresponds to the 6-month score reached by the PT-group in the current study. Haahr et al. (25) compared undefined physical therapy with surgery in patients with SIS. The surgery group received one session of PT instruction for home exercises, which was similar to the H-group instructions in our study. The results showed that their surgery group reached a mean CM score of 53 at the 1-year follow-up, which is in line with the mean reached by the H-group in the present study. This suggests that instructions for home exercises, focusing on mobility, are not sufficient, and that strengthening exercises for the rotator cuff and scapula stabilizers need to be added in order to reach optimal shoulder function after ASD.
Exercise protocols after subacromial decompression that are described in the literature (10, 11, 34, 35) often have a more protective regime than that used in the PT-group in our study. In the study by Andersen et al. (11), strengthening exercises were not started until 6 weeks after surgery. The authors suggested that a more progressive programme would not be tolerated and might counteract and extend the rehabilitation period. In the present study, dynamic strengthening exercises for the rotator cuff and the scapula stabilizers began as early as 4 weeks after surgery. No increased pain was reported in the PT-group that performed the progressive exercises, indicating that the progression of load was well-tolerated and the subacromial tissues were probably not negatively stressed. The study by Klintberg et al. (12) featured a rehabilitation programme with a similar design and progression to our supervised rehabilitation. They also reported that patients tolerated the progression, further supporting the early postoperative activation of the rotator cuff.
In the current study both groups reported significantly increased pain and decreased shoulder function 1 week after surgery, due to the postoperative acute phase. One month after surgery, the pain levels had improved and were significantly lowered compared with the baseline in both groups. This is probably due to the surgical removal of the structural pathology. One month after ASD, shoulder function was also back to preoperative levels and continued to improve after this point. This improvement was also similar in both groups and was most likely a response to the ASD. Starting at 3 months after surgery, the PT-group began to show significantly greater improvement in functional status compared with the H-group, and this effect may have been due to specific components of the PT-supervised rehabilitation.
Sick leave is a common problem among patients with shoulder problems (4). In this study, a larger proportion of patients in the PT-group returned to full-time work after 3 months; however, the data is insufficient to conclude that a more progressive programme promotes a faster return to work. Future studies with a larger sample size is needed to clarify whether a more progressive rehabilitation programme could affect the duration of sick leave and the percentage of patients returning to work, as well as recurrence rates.
One limitation of this study is that the 2 groups received uneven attention; the PT-group had more consultations than the H-group. It is possible that this might have influenced the results in favour of the PT-group. The positive results observed in the PT-group are likely due to a combination of placebo, attention, and the specific treatment effect. Many follow-ups were performed, which could have compensated for this uneven attention. In connection with these follow-ups, patients in the H-group had the opportunity to discuss their exercise programme with an independent PT and to ask questions. Also, all the patients received 1 telephone call after 2 weeks, with the purpose of encouraging them to perform their home exercises. As well as the additional contact with the PT-group, there was also a substantial difference in content between the 2 rehabilitation strategies. This was intentional, since the standard practice at participating clinics was to provide instructions for home exercises, which we thought was insufficient for effect on shoulder function. The purpose of this study was to evaluate the use of a more comprehensive and progressive programme, including specific strengthening exercises for the rotator cuff and scapula stabilizers. The difference in shoulder function, but not in pain intensity between the groups supports to some extent that ASD decreases the pain regardless of the rehabilitation being used, and suggests that rehabilitation including strengthening exercises is important for restoration of more optimal shoulder function, 6 months after surgery. Further research is needed to clarify to what extent the positive effect reflects the impact of PT supervision.
Although the results should be interpreted with some caution due to the small sample size, the current study indicates that, with regard to shoulder function and pain in patients after ASD, PT-supervised rehabilitation focusing on strengthening exercises for the rotator cuff and scapula stabilizers is superior to instructions for home exercises with a focus on increasing mobility. Since this progressive, PT-supervised rehabilitation programme was well-tolerated, it could be safely implemented for patients after ASD. Additional randomized clinical trials are needed to validate these findings.
REFERENCES