OBJECTIVE: To investigate whether an online occupational postural and exercise intervention reduced patients’ overall risk status for chronicity in subacute non-specific low back pain compared with conventional treatment, and to determine whether changes in risk of chronicity correlate with changes in specific outcomes (i.e. Functional Status and QoL) for low back pain.
DESIGN: Prospective, single-blinded randomized intervention study.
SUBJECTS: University office workers with subacute non-specific low back pain (n = 100) were randomized 1:1 to an intervention group, who received an online occupational postural and exercise intervention, and a control group.
METHODS: Exercise and education materials used in the intervention were developed as an online resource, and included video demonstrations recorded in a laboratory. All sessions included exercises combining postural stability (for abdominal, lumbar, hip and thigh muscles) strengthening, flexibility, mobility, and stretching. Outcome measures included STarT Back Screening Tool (SBST), Roland Morris score, and European Quality of Life Questionnaire – 5 dimensions – 3 levels. At 9 months, SBST was analysed and compared with the baseline and controls.
RESULTS: Significant positive effects were found on mean scores recorded in the online occupational exercise intervention group for risk of chronicity (p < 0.019). A correlation between functional disability, health-related quality of life and risk of chronicity of low back pain was observed.
CONCLUSION: This study supports the potential utility of a real-time occupational internet-based intervention for preventing progression to chronicity of subacute non-specific low back pain among office workers.
Key words: occupational therapy; LBP; internet; chronic illness; rehabilitation.
J Rehabil Med 2012; 44: 581–587
Guarantor/corresponding author: Narcis Gusi, Faculty of Sports Sciences, University of Extremadura Avenue, Universidad s/n, ES-10071 Cáceres, Spain. E-mail: ngusi@unex.es
Submitted July 25, 2011; accepted February 13, 2012
INTRODUCTION
Non-specific low back pain (LBP) is one of the most common health problems encountered in primary care (1), with an estimated point prevalence of 33% among office workers (2). Evidence suggests that 80% of the total costs attributable to LBP are consumed by a relatively small group (10%) of patients who develop chronic symptoms (3). Chronic LBP is associated with lower self-reported health status, increased functional disability, and increased time off work (4). Prevention of chronicity is therefore a priority.
Research is increasingly focused on improving the effectiveness of secondary prevention interventions, through better identification of modifiable prognostic factors involved in the transition from acute back pain to chronic symptoms. While key prognostic factors are well documented (5), fewer studies report interventions specifically designed to tackle these risk factors (6, 7). Multidisciplinary interventions (based on functional exercise packages of advice and education) are effective in reducing disability and addressing the psychosocial factors known to be influential in the progression to chronic LBP (8). Recent online interventions have demonstrated the clinical effectiveness of using real-time workplace advice (including regular e-mail reminders) to help patients make healthy lifestyle choices, improve fitness levels and achieve an early return to work (9). In addition, the subacute phase of LBP has been recommended as an optimal secondary prevention intervention window (10). Treatment mediators are those factors that need to change following treatment to influence outcome (11). Fewer studies have reported on treatment mediators of LBP outcome than have investigated prognostic factors. A key message from the existing research is the importance of psychosocial factors, alongside physical factors (12). Although cognitive behavioural interventions exist to tackle chronic pain (13), there are no reports of real-time internet-based interventions focused specifically on secondary prevention of chronic LBP by targeting key modifiable prognostic indicators among office workers, to reduce costs and improve efficacy.
We therefore developed a new occupational intervention for workers with subacute LBP. The intervention consists of twocomplementary components; e-mail reminders sent to improve patient adherence; and an internet-based, physical secondary prevention intervention, focused on increasing physical exercise levels and providing postural education relevant to the workplace. Regarding the effectiveness of this intervention on health-related quality of life (HRQoL) and functional status of LBP, this trial tests the overall hypothesis that our model of occupational management for office workers with subacute LBP, delivered through an online, real-time intervention is feasible, safe and effective in improving physical function. In this respect, the aim was to investigate whether the intervention reduced patients’ overall risk status for chronicity compared with conventional treatment, and, if so, to determine which individual predictive factors were acting as the key treatment mediators for this risk reduction intervention. This study also tests the hypothesis that changes in risk of chronicity could correlate with changes in functional status and HRQoL.
METHODS
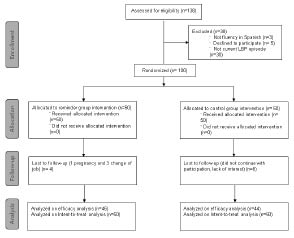
Fig. 1 shows the flow of participants through the study, which was a single-blind randomized controlled trial (ISRCTN40949689). The study was based in the 4 administrative offices of University of Extremadura, Spain. To ensure correct implementation of the protocol, a manual describing the study protocol was produced and made available to all researchers involved in the study. Before the study commenced, two technicians received two weeks training in all aspects of the study protocol. The study was performed in accordance with the Declaration of Helsinki, as revised in 2000 in Edinburgh, and was approved by the research ethics committees of the University of Extremadura.
Fig. 1. Participant flow diagram.
Participants
Participants with subacute non-specific LBP were recruited via the preventive medicine service of the university. An advertisement alerted potential participants to the project. Sub-acute non-specific LBP was defined as current LBP, with or without radiating leg pain, without any specific pathological conditions, and with a first or recurrent episode having lasted from 6 to 12 weeks. Inclusion criteria were as follows: a diagnosis of subacute LBP in the absence of any major neurological deficit; age between 18 and 64 years; physical inactivity (less than 2 exercise sessions of 30 min per week); a willingness to provide informed consent; being an employee; and a requirement to work more than 6 h per day on a computer workstation. Participants were excluded if they reported a diagnosed cause of backache; chronic backache; disc disease or any other major disease; or a lack of fluency in Spanish. A total of 138 individuals who fulfilled the criteria were invited via e-mail and telephone to participate in the study, and 38 were subsequently excluded. The remaining 100 patients were randomly allocated 1:1 to 2 groups: an online occupational exercise intervention group and a control group.
Treatments
The exercise and education reminders used in the treatment programme were developed as an online resource, and included video demonstrations recorded in a laboratory. The resources were loaded onto a dedicated section of the university preventive medicine service website. The physical exercise routine was designed and arranged by an experienced professional in physical activity and supervised by the clinical lead of the Preventive Medicine Service. All sessions included exercises combining postural stability (for abdominal, lumbar, hip and thigh muscles) strengthening, flexibility, mobility, and stretching. Mobility exercises were carried out using large movements of the joints associated with postural stability muscles. Flexibility exercises were carried out using a static work methodology. Strength exercises were carried out using progressive shortening:stretching speed:motion ratios (1:1, 1:2, 1:3, 2:1, 3:1) combined with slight isometric contractions of the muscles involved in the exercises. Finally, stretching exercises were carried out by moderate stretching of the muscles involved in the session. All the exercises were explained both by oral instruction and by written subtitles. The postural education reminders, addressing and promoting how best to sit at a computer and the adjustment and rearrangement of the office workstation layout, were designed by the university preventive medicine service clinician. Data on participation in the programme was collected automatically by registering access to the programme. The reasons why people abandoned the programme were also collected. Both the online occupational exercise intervention group and the control group had access to the usual routine care provided by the university preventive medicine service. This included a routine annual medical examination by the lead clinician of the preventive medicine service, and specific online information on self-care in the workplace.
Online occupational exercise intervention group. A short e-mail was sent every day with a reminder message (which did not change throughout the intervention) containing a link to the online “session of the day”. The sessions were structured in real-time, first playing a video of postural reminders (2 min), then a video of the exercise(s) for the day (7 min), followed by postural reminders once again (2 min). The videos were available Monday to Friday, weekly, for 9 months. Each participant was assigned a user name and password to access the system, and the treatment programme was explained to them. Participants were asked not to perform any formal physical activity routine during the training period.
Control group. The control group had access only to standard preventive medicine care.
Measurements
Both groups were evaluated at baseline and on completion of the 9-month intervention. Socio-demographic and health characteristics, including age, smoking habits and sex, were recorded. The questionnaires were administered by a trained technician (14) who was independent from the study team and blind to treatment allocation. A Spanish version of the Keele STarT Back Screening Tool (SBST) was used to evaluate the severity and the risk of chronicity of common LBP (15). The SBST has 9 items, selected as predictive of “poor prognosis” following a literature review and secondary analysis to identify strong independent predictors for persistent (chronic) disabling LBP. The predictive validity and external validity of the SBST have been reported, as has its reliability, with a Kappa of 0.79 (16). Two outcome measures for low back pain were used to assess the hypothesis that changes in risk of chronicity could correlate with changes in specific outcomes (i.e. Functional Status and QoL). In this sense the Roland Morris Questionnaire was used to assess the functional disability related to LBP (17), which has been previously validated in Spanish (18). Validity and reliability with an intraclass correlation coefficient (ICC) of 0.87 of this instrument has also been reported previously (18). It consists of a list of 24 items that reflect limitation in different activities of daily living, and has a score ranging from 0 (no disability) to 24 (maximum disability). Also, the European Quality of Life Questionnaire – 5 dimensions – 3 levels (EQ-5D-3L) (19) was used to assess HRQoL. The validity of this instrument has been reported, as has its reliability, with an ICC of 0.73 (20). Five domains, encompassing mobility, self-care, usual activities, pain/discomfort and anxiety/depression, plus an overall description of health status, can be assessed using the EQ-5D-3L utility index Time Trade Off (TTO) (21).
Sample size
Prior to the beginning of this trial, the sample size was estimated based on the Roland-Morris Disability Questionnaire desired change at 9 months. A difference of 2.5 points in Roland-Morris Disability Questionnaire change scores is considered to be a minimum clinically important difference in a Spanish population (22). A sample size of 62 patients (31 per group) would enable detection of a between-group difference of 2.5 Roland and Morris Disability Questionnaire points, given 80–90% power, a 5% (two-tailed) significance level, and a conservative standard deviation of 5 points (23). However, 100 patients were selected to allow for potential dropouts, estimated at 20%.
Statistical analysis
An intention to treat (ITT) analysis and a per protocol analysis were conducted. ITT analysis was performed to report the effects of the intervention on main outcome measure within the possibility of drop-outs after randomization, and was done under the “baseline carried forward” approach (assigning zero change from baseline as an end-point) (24). Variables were compared at baseline using Student’s t-test for independent measures in quantitative variables, and the χ2 test for qualitative variables. The distribution of the data was examined using the Kolmogorov-Smirnov test with the Lilliefors correction. After confirming that the distribution of all variables was parametric, the inter-group comparison of the quantitative study variables was performed with two-way analysis of variance (ANOVA) for repeated measures. The significance level was set at p < 0.05. In addition to the p-values, we provided detailed statistics including the mean and 95% confidence interval (CI) for better depicting the change within each intervention group from baseline to 9 months, and the treatment effect. The differences between pre- and post-test variables were used to describe the changes from baseline to 9 months. The differences between individual changes over 9 months in one group and these individuals’ changes in the other group were used to estimate the treatment effect in the case of quantitative variables. The mean and 95% CI of changes were calculated using Student’s t-test for independent samples in each. The null hypothesis of no difference in the proportion of prevention of risk of chronicity between the treatment conditions was evaluated by a χ2 test. To confirm or reject our hypothesis we also performed a post-hoc analysis. In this case, odd ratios (95% CI) were undertaken to assess the treatment effect. Number needed to treat (NNT) was calculated for the outcomes measures of this trial. Effect sizes were calculated for quantitative variables, to determine the magnitude of change, and Cohen’s coefficient was used to assess the change. A change from 0 to 0.2 was considered small, a change of 0.2–0.5 was considered medium, and a change of 0.5–0.8 was considered large. The strength of relationship between the risk of chronicity of pain, functional disability and HRQoL was investigated using a Pearson coefficient. To determine whether the intervention reduced patients’ overall risk status for chronicity we compared, using χ2, the proportions of patients in each group who, at 9-month follow-up, were low risk on the SBST. To determine which individual predictive factors were key treatment mediators for this risk reduction, a binary logistic regression was performed using changes within the 8 predictive factor items measured by the SBST to explore which items were most associated with low-risk outcomes. All tests were undertaken using SPSS version 19.0 (IBM).
RESULTS
One-hundred subjects were randomized (Fig. 1). There were no statistically significant differences between the intervention and control groups at baseline (Table I). No participants showed any significant adverse events related to the treatments, and compliance was high (92%) for the online occupational exercise intervention group. Of the 4 participants in the online occupational exercise intervention group who dropped out of the programme, 3 changed jobs and 1 stopped due to pregnancy. Six participants in the control group were lost through apparent lack of interest, with a total of 88% compliance achieved in the group.
| Table I. Baseline characteristics of participants in the study (n = 90) |
| Group | Control group (n = 44) Mean (SD) | Intervention group (n = 46) Mean (SD) | p |
| Age (years) | 45.50 (7.02) | 46.83 (9.13) | 0.44 |
| Sex (%) Male Female | 11.4 88.6 | 15.2 84.8 | 0.59 |
| Smokers, yes/no, % | 50/50 | 56.5/43.5 | 0.53 |
| Roland Morris Questionnaire score, points | 11.65 (2.14) | 12.28 (2.63) | 0.22 |
| TTO, points | 0.78 (0.08) | 0.75 (0.11) | 0.23 |
| SBST total score, points | 4.38 (1.67) | 4.36 (1.28) | 0.95 |
| SBST psychological score, points | 2.36 (1.03) | 2.28 (0.98) | 0.70 |
| p-values from t-test for independent measures or χ2 test. TTO: Time Trade Off; SBT: STarT Back Tool; SD: standard deviation. |
Effects of the intervention on the risk of chronicity prognosis factors
Table II reveals the comparative effects between groups on the main outcomes at 9 months. Significant positive effects were found on mean LBP severity scores recorded in the online occupational exercise intervention group (SBST 23% change; 2.12 NNT; 0.80 effect size; –1.01 [–1.790 to 0.118] treatment effect; p = 0.019). Significant reductions in the risk of chronicity of LBP, measured with SBST, were seen in the intervention group compared with the control group: 60.9% patients in the online occupational exercise intervention group were SBST low-risk at 9 months, compared with 27.9% patients in the control group (p < 0.01). The ITT analysis (data not shown) gave similar results to the efficacy analysis for all outcome measures of the current trial.
| Table II. Effects of 9-month of web-based intervention on risk of chronicity of non-specific subacute low back office workers (n = 90) |
| Outcomes measure | Baseline | Post-treatment | Treatment effect Mean (95% CI) or OR (95% CI) | p | Effect size |
| Control group (n = 44) Mean (SD) | Intervention group (n = 46) Mean (SD) | Control group (n = 44) Mean (SD) | Intervention group (n = 46) Mean (SD) |
| SBST total score, points | 4.40 (1.71) | 4.38 (1.48) | 4.38 (1.03) | 3.39 (1.39) | –1.01 (–1.790 to 0.118) | 0.019 | 0.80 |
| SBST psychological score, points | 2.36 (1.03) | 2.28 (0.98) | 2.31 (1.09) | 1.84 (0.86) | –0.39 (–0.993 to –0.215) | 0.201 | 0.47 |
| Risk of chronicity | | | | | | | |
| Low risk, yes, % | 31.8 | 23.9 | 27.9 | 60.9 | 3.38 (1.591 to 9.501)a | 0.005 | –– |
| Medium risk, yes, % | 54.5 | 65.2 | 57.5 | 34.8 | 0.40 (0.169 to 0.946)a | 0.059 | –– |
| High risk, yes, % | 13.7 | 10.9 | 14.8 | 4.3 | 0.28 (0.055 to 1.511)a | 0.122 | –– |
| aApplicable OR. p-values from analysis of variance (ANOVA) for repeated measures or χ2 to compare different between groups after 9-month web-based multi-factor programme. Item 1 is scored as positive if ”very much” or ”extremely” bothered is marked. Items 2–9 are positive if ”agree” is marked. Psychosocial subscale items are 1, 4, 7, 8 and 9. Patients are allocated to the high-risk group if the psychosocial subscale score is ≥ 4. The remaining patients are allocated to the low-risk group if the overall tool score is < 4 and to the medium-risk group if the overall tool score is ≥ 4; ––: not computable. SBST: STarT Back Screening Tool; OR: odd ratios (control group/reminder group); SD: standard deviation; CI: confidence interval. |
The 9 SBST items remained unchanged among the control intervention group, while the online occupational exercise intervention group showed significant positive effects in disability items 4 and 5, and fear item 6 (p = 0.017, 0.008 and 0.049, respectively). Post-hoc analyses confirm these results. There was a trend towards a decrease in all 9 SBST items in the intervention group (Table III). Table IV shows the Pearson correlation coefficients between main outcomes. A strong relation between functional disability, HRQoL, and risk of chronicity of LBP (except with psychological score) was observed. Our binary regression model demonstrated that the reduction in chronicity was primarily associated with changes in SBST disability and fear avoidance items resulting from the intervention. This resulted in a 51% change in the proportion who were low risk, with odds ratios of 0.166 (0.0638–0.431) (p < 0.001), 0.092 (0.027–0.313) (p < 0.001), and 0.302 (0.107–0.853) (p < 0.024), in the 4, 5 and 6 SBST items, respectively (Table V).
| Table III. Effects of 9-month of web-based programme on SBST 9-item scores (n = 90) |
| Outcomes measure | Baseline | Post-treatment | p | OR (95% CI) |
| Control group (n = 44) | Intervention group (n = 46) | Control group (n = 44) | Intervention group (n = 46) |
| SBST global-related items (low risk) | | | | | | |
| Referrer leg pain (item 2) | 43.2 | 47.8 | 45.5 | 39.1 | 0.544 | 0.771 (0.334–1.784) |
| Co-morbid pain (item 3) | 40.9 | 45.7 | 36.4 | 37.0 | 0.953 | 1.026 (0.435–2.419) |
| Functional disability (item 5) | 61.5 | 63.0 | 68.2 | 43.5 | 0.008 | 0.308 (0.127–0.748) |
| Functional disability (item 6) | 56.8 | 52.2 | 54.5 | 34.8 | 0.049 | 0.444 (0.190–1.058) |
| SBST psychosocial-related items (medium/high risk) |
| Bothersomeness (item 1) | 22.7 | 26.1 | 25.0 | 23.9 | 0.905 | 0.943 (0.360–2.466) |
| Fear avoidance (item 4) | 72.7 | 73.9 | 70.5 | 45.7 | 0.017 | 0.352 (0.148–0.840) |
| Catastrophizing (item 7) | 52.3 | 50.0 | 50.0 | 43.5 | 0.535 | 0.769 (0.335–1.764) |
| Anxiety (item 8) | 43.2 | 52.2 | 47.7 | 47.8 | 0.993 | 1.004 (0.439–2.296) |
| Depression (item 9) | 45.5 | 39.1 | 38.6 | 23.9 | 0.132 | 0.499 (0.201–1.239) |
| Values expressed as percentage (%) of agreement. p-values from χ2 test to compare different between groups after 9-month intervention. SBST: STarT Back Screening Tool; item 1: question 1 of SBT; item 2: question 2 of SBT; item 3: question 3 of SBST; item 4: question 4 of SBT; item 5: question 5 of SBST; item 6: question 6 of SBST; item 7: question 7 of SBST; item 8: question 8 of SBT; item 9: question 9 of SBT; CI: confidence interval; OR: odds ratio (control group/intervention group). |
| Table IV. Correlation between severity of pain, risk of chronicity of pain, self-reported functional disability and self-reported health-related quality of life after treatment among office workers suffering by subacute non-specific low back pain (n = 90) |
| Outcomes measures | dSBST total score | dSBST psychological score | dRoland Morris | dTTO | dLow risk | dMedium risk | dHigh risk |
| dSBST total score | 1.000 | 0.699** | 0.299** | –0.212* | –0.776** | 0.449** | 0.474** |
| dSBST psychological score | | 1.000 | 0.111 | –0.117 | –0.525** | 0.114 | 0.631** |
| dRoland Morris | | | 1.000 | –0.612** | –0.361** | 0.247* | 0.159 |
| dTTO | | | | 1.000 | 0.239* | –0.151 | –0.126 |
| dLow risk | | | | | 1.000 | –0.807** | –0.236* |
| dMedium risk | | | | | | 1.000 | –0.384** |
| dHigh risk | | | | | | | 1.000 |
| *Correlation significant at 0.01 level; **correlation significant at 0.001 level. Pearson’s correlation coefficients. dSBST total score: STarT Back Screening Tool score total score difference after treatment; dSBST psychological score: STarT Back Tool psychological score difference after treatment; dRoland Morris: Roland Morris questionnaire score difference after treatment; dTTO: time trade-off points differences after treatment; dLow risk: low risk differences after treatment; dMedium risk: medium risk differences after treatment; dHigh risk: high risk differences after treatment. |
| Table V. Binary logistic regression of change in low risk of chronicity of low back pain after 9 months of web-based intervention (n = 90) |
| | –2 Log likelihood = 68.43; Cox & Snell R2 = 0.36; Nagelkerke R2 = 0.52 |
| Coefficient | SE | Wald Statistic | OR (95% CI) | pa |
| dFear avoidance (item 4) | –1.797 | 0.487 | 13.592 | 0.166 (0.0638–0.431) | < 0.001 |
| dFunctional Disability (item 5) | –2.386 | 0.625 | 14.588 | 0.092 (0.027–0.313) | < 0.001 |
| dFunctional Disability (item 6) | –1.197 | 0.530 | 5.107 | 0.302 (0.107–0.853) | 0.024 |
| Constant | –1.927 | 0.451 | 18.217 | 0.146 (0.060–0.353) | < 0.001 |
| ap-values from χ2. dLow risk: low-risk differences after treatment; item 4: question 4 of STarT Back Screening Tool difference after treatment; item 5: question 6 of STarT Back Screening Tool difference after treatment; item 7: question 7 of STarT Back Screening Tool difference after treatment; OR: odds ratio; CI: confidence interval; SE: standard error. |
DISCUSSION
This is the first study to analyse the effects of a real-time, occupational, internet-based intervention on the prevention of chronicity of non-specific LBP among office workers. To our knowledge, it is also the first instance of monitoring of the risk of chronicity and the change in prognostic factors after treatment using the SBST. The main findings of this study were that this intervention was effective to reduce the risk of progression to chronicity among office workers with subacute non-specific LBP. Other internet-based interventions using real-time e-mail reminders have been conducted, with the aim of increasing the quality of patients’ lifestyles. However, to our knowledge, there are no other internet-based studies using a physical intervention conducted at the workplace that are designed to prevent the chronicity of non-specific LBP among office workers.
At 100 patients, our sample size might appear small; however, we completed the trial with numbers within the estimated sample size needed to demonstrate clinically significant effects with the methods used. Also, the timing and nature of this intervention was in accordance with current clinical guidelines, which recommend multidisciplinary interventions (based on functional exercise combined with postural education) to improve physical function, and include psychosocial factors, which have been determined as risk factors in the transition from (sub)acute to chronic LBP (8). It is also potentially possible to reach a large population of office workers with non-specific LBP to prevent the chronicity of the ailment using the chosen mode of delivery of the interventions (25).
The high level of adherence observed in the intervention group may have been due to the target of our occupational intervention for secondary prevention of LBP (26). Also, the short sessions used in this trial could explain the high level of adherence. In this regard, previous research suggests that exercise programmes of short duration are preferable for employees and employers. Thus, reaching positive outcomes in low back pain patients (27). A major determinant of the high retention of the intervention could be the use of e-mail reminders sent to improve patient adherence. This is consistent with another study, in which a high level of adherence to activities designed to promote healthy lifestyles in asymptomatic office workers was achieved through the use of intervention e-mails at the workplace (9).
The SBST was developed to help clinicians objectively measure the severity of the domains screened by the 9-item tool (determined as predictive factors of persisting disabling back pain), and determine the risk of chronicity of LBP (16). This tool has been adapted for use among the general Spanish population (15). There was statistically significant improvement in the SBST total score at 9 months in the active intervention group compared with the controls. This shows that participants in the internet-based intervention decreased their risk of chronicity compared with those allocated to standard treatment. In our study, intervention group participants, compared with control group participants, were more likely to experience enhanced progression to a low risk of back pain chronicity. Recovery rate, defined in terms of transition to a low risk of chronicity of pain, was 77% higher in the intervention group compared with the control group. Physical therapy, a common treatment for LBP, was taken as part of a multidisciplinary intervention, because activity is a keystone of early intervention and rehabilitation (28). However, there are controversial results across the scientific literature on the value of physical therapy at an early juncture. For example, a systematic review concluded that exercise therapy was ineffective (moderate evidence) and that several other physical therapy techniques had limited effectiveness (29). One possible discriminating factor may be whether the intervention is an active or a passive treatment. Indeed, working on the patient’s apprehension about keeping active may be a key point (30). Another systematic review addressed the strong evidence that most specific exercises programmes designed to prevent LBP are ineffective in isolation (31). In any case, research suggests that there is limited evidence supporting the use of exercise to prevent LBP episodes in the workplace (27). There is a need to know, therefore, whether adequate, timely physical therapy in combination with psychosocial tasks has value as a secondary prevention (7). In this regard, our results suggest that a real-time internet-based physical intervention could prevent chronicity of LBP. These results are in agreement with some previous research showing improvements in back pain-related outcomes when exercise is combined with other modalities, such as cognitive behaviour intervention (7), functional movements, relaxation, or the integration of coping skills (32). The relatively large effects found in this study regarding the prevention of chronicity are supported by other studies that employed multidisciplinary management of LBP. These include combinations of cognitive behavioural interventions and exercise to prevent chronicity of LBP among patients in the subacute phase (6, 33). There were no differences in the psychological score of SBST between groups after treatment in our study, which was possibly due to the fact that treatment mediators associated with this part of the instrument were not strongly affected at baseline in our subjects (11). On the other hand, in previous studies carried out in patients with subacute non-specific LBP, significant correlations between risk of chronicity, self-reported functional disability, and health-related quality of life were reported (34, 35); these results are in accordance with our data when the correlation coefficients between these variables are taken into account.
To better explain the results regarding the transition to low risk of chronicity after treatment, we performed a binary logistic regression within the SBST items 4 (fear avoidance), 5 and 6 (functional disability). A change over time in favour of the active intervention group has already been observed for these items. Within these results, the variance between the two groups in the proportion who transitioned to a low risk of chronicity was 51%, which is in favour of active intervention group participants. The findings of our physical intervention are in accordance with other studies that have shown other interventions to be effective in decreasing the risk of chronicity by improvements in prognostic factors of persistent LBP, such as fear avoidance using a multidisciplinary-based intervention (36) or disability using a graded-based exercise intervention (37). These results could be explained in part by the design of our intervention, where we introduced a graded exercise series (with variation in the intensity of the exercises) in order to decrease fear-avoidance beliefs and disability values reported at baseline in our subjects, and thus increase the effectiveness of our intervention in reducing the risk of chronicity (11). George and colleagues (37) performed a randomized trial comparing standardized physical therapy with or without the inclusion of graded exercises designed to reduce pain-related fear. A significant interaction between elevated fear-avoidance beliefs and treatment outcome was reported, suggesting that the baseline level of fear-avoidance beliefs was a treatment effect modifier for physical therapy incorporating graded exercises (38). However, further research is needed to identify relevant psychosocial baseline findings that can direct the choice of treatment strategies to improve clinical outcomes.
We acknowledge some limitations in this study. First, this intervention was delivered in the Preventive Medicine Service of the university: only one setting was used, and we do not know if this intervention would be feasible and effective in other settings. However, the scientific literature shows that specific medical counselling seems to be a key element in the delivery of interventions to enhance inactive people’s physical activity (39). Secondly, we did not take into account factors that may affect feasibility, such as participant satisfaction, context, and dose received (40). However, we experienced a high level of compliance, which led us to suppose that these factors have a positive influence on the level of feasibility found in our study. The external validity of our study must also be considered. This study was conducted in a predominantly white, urban, south European community; therefore, it may not be possible to generalize the outcomes to workplace programmes in all communities. Cross-cultural analyses on this are warranted. Further studies are also needed to compare the efficacy of our internet-based programme in different patient populations affected by back pain (e.g. chronic patients), and to examine its cost-effectiveness as a public health strategy for preventing persistent LBP in the workplace and its associated costs.
In conclusion, this study supports the feasibility and potential utility of a real-time occupational web-based intervention for preventing progression to chronicity of subacute non-specific LBP among office workers. The current study provides new insights that could help private and public office environment managers in the prevention of negative consequences of non-specific LBP in subacute phases.
ACKNOWLEDGEMENTS
The present study was supported by the University of Extremadura (Quality of Life Research Group and Occupational Preventive Medicine) and Government of Extremadura and European Union Regional Development Funds for research groups (GR10127).
Conflicts of interest. None to declare.
REFERENCES