OBJECTIVES: To characterize a spinal cord injury (SCI) population from the 2008 Sichuan earthquake in China; to evaluate functional outcomes of physical rehabilitation interventions; to assess potential determinants of rehabilitation effectiveness; and to assess medical complications and management outcomes.
METHODS: A total of 51 earthquake victims with SCI were enrolled and underwent rehabilitation programming. Functional rehabilitation outcomes included ambulation ability, wheelchair mobility and activities of daily living (ADL) assessed with the Modified Barthel Index at the beginning and end of rehabilitation. Effectiveness of rehabilitation and the effect of other predictors were evaluated by mixed effects regression. Outcomes of medical complication management were determined by comparison of the incidence of respective complications at the beginning and end of rehabilitation.
RESULTS: Ambulation, wheelchair mobility and ADL were significantly improved with rehabilitation programming. Both earlier rescue and earlier onset of rehabilitation were significant positive predictors of rehabilitation effectiveness, whereas delayed onset of rehabilitation combined with prolonged time to rescue resulted in a lesser positive effect. Medical complications were managed effectively in 63% (pressure ulcers) to 85% (deep vein thrombosis) of patients during rehabilitation.
CONCLUSION: Earthquake victims with SCI may achieve significantly improved functional rehabilitation functional outcomes on a formal, institutional-based physical rehabilitation programme.
Key words: earthquake; rehabilitation effectiveness; physical functioning; spinal cord injury; physical rehabilitation; medical rehabilitation.
J Rehabil Med 2012; 44: 534–540
Correspondence address: Jianan Li, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 210029; E-mail: lijianan@carm.org.cn
Submitted January 8, 2012; accepted May 3, 2012
INTRODUCTION
Spinal cord injury (SCI) was one of the most severe disabling injuries sustained in the 2008 Sichuan earthquake, resulting in nearly 86,000 deaths and missing persons as well as 14,000 hospitalizations (1). An SCI was sustained by 13–15.2% of all patients admitted to the nearest tertiary care hospital (2).
A national rehabilitation team was formed, comprising rehabilitation professionals from institutional rehabilitation departments from other provinces and including several of the authors. Members of this team provided rehabilitation services to SCI patients and others in newly established rehabilitation departments of 3 hospitals within the most severely affected earthquake area, from approximately 2 months after the earthquake for as long as 2 years.
This study characterizes SCI victims of the Sichuan earthquake and assesses the effect of institutional, individualized physical rehabilitation programming on victims’ functional recovery. The specific aims of the study were: (i) to identify demographic and SCI characteristics of the affected population; (ii) to demonstrate the effectiveness of individualized physical rehabilitation programming performed in an institutional setting on SCI victims; (iii) to clarify the relationship of rehabilitation effectiveness to the timing of rescue and the beginning of rehabilitation programming, duration of rehabilitation programming, the level of the neurological deficit, and select demographic variables; and (iv) to report incidences of related medical complications and associated management outcomes.
This analysis is intended to serve as a reference for future large-scale natural disasters, particularly earthquakes.
METHODS
Design
This is a prospective cohort study measuring variables of interest at the beginning and end of an individualized, institutional physical rehabilitation programme.
Participants
A total of 54 SCI earthquake victims from 3 hospitals with large rehabilitation departments in the earthquake zone (West China Hospital, Chengdu, Jiangyou Orthopedic Hospital, Jiangyou and Mianzhu County Hospital, Mianzhu) were identified and enrolled and consents were obtained. Patients received an SCI evaluation prior to starting an individualized physical rehabilitation programme. Patients were evaluated at the conclusion of rehabilitation prior to discharge to the community. Three patients with medical co-morbidities including severe pressure sores and systemic infection were unable to complete the course of rehabilitation and were excluded; thus, 51 patients completed the study. Written informed consent was obtained from all participants and study approval was granted by the ethics committees of West China Hospital, Jiangyou Orthopedic Hospital and Mianzhu County Hospital.
INTERVENTION: Physical rehabilitation programming
Rehabilitation departments were established within 3 hospitals in the earthquake zone to manage patients with severe, disabling traumatic injuries including SCI. Institutional staffing included rehabilitation professionals from other hospitals with well-developed rehabilitation departments outside of Sichuan province (e.g. Nanjing, Guangzhou and Beijing) who had a degree in rehabilitation medicine and at least 2 years of clinical experience. The newly established rehabilitation departments received SCI patients primarily from tertiary medical centres across China, where they had been initially transported following the earthquake care since hospital care in the disaster zone was severely disrupted. Specialized SCI care was not available at most of these non-Sichuan hospitals.
Once cleared of medical complications requiring hospitalization in a different hospital department, patients received a SCI assessment including a detailed neurological examination by the rehabilitation team. Individualized physical rehabilitation programmes based on specific patient treatment goals were developed and implemented. The multidisciplinary rehabilitation team, comprised of physiatrists, therapists (physical, occupational and traditional modality), rehabilitation nurses, volunteers and other consulting medical specialists as needed, provided comprehensive management of SCI patients in the rehabilitation department for the remainder of their hospitalization (3). Provider responsibilities included overall medical management including co-morbidities and complications, execution of the rehabilitation programme with progress evaluations, and discharge planning.
Rehabilitation treatment programme modalities included range of motion (ROM) exercises, muscle strengthening, transfers, training in activities of daily living (ADL), and mobility training (including walker and wheelchair usage). Ultrasound, functional electrical stimulation, electrotherapy (i.e. high, medium, and low frequency stimulation), infrared, and lymphatic flow modalities were selectively applied. Traditional Chinese therapies including acupuncture and massage were also performed. Patients were educated in management of bladder and bowel continence, skin care, and self-exercise. Assistive devices including prostheses and orthoses were prescribed and provided if indicated. Most patients received rehabilitation therapy for approximately 3 months prior to discharge to the community.
Measurement
SCI was assessed by neurological examination of level of injury, and patients were divided into 4 groups by functional prognosis to allow comparison with the classification of SCI victims of the 2005 Pakistan earthquake used by Rathore (4): cervical (C8–C1); thoracic (T1–T10); thoracolumbar (T11–L1); and lumbosacral (L2–S5). The American Spinal Injury Association (ASIA) Impairment Scale (AIS; 5) was used to grade injury severity. Time to rescue, time to surgical stabilization, and time to rehabilitation intervention were identified primarily from hospital records.
Functional rehabilitation outcomes were evaluated as follows:
• Ambulation ability was categorized into independent walking (without an assistive device), walking with ankle-foot orthosis (AFO), walking with knee-ankle-foot orthosis (KAFO), and wheelchair dependence (6).
• Wheelchair mobility was dichotomized into independent handling of a mechanical wheelchair or dependent mechanical handling/powered propulsion based on performance of weight shifting on wheelchair, 2-way transfer to bed, and propulsion over flat ground skills (7).
• ADL independence was represented by Modified Barthel Index (MBI; 8) scores: 0–20 indicates total dependence; 21–60: severe dependence; 61–90: moderate dependence; 91–99: slight dependence, 100 no dependence). (Although MBI dependency scores were originally established in stroke patients and do not necessarily transfer to persons with SCI, reliability and validity of the MBI in SCI patients is good and this application of the instrument is standard practice in China (9, 10)). ADL independence was assessed at the beginning and end of rehabilitation programming.
Data on incidence and treatment outcome of medical complications, including pressure sores, pain, bowel and bladder dysfunction, urinary tract stones, respiratory and urinary tract infections, postural hypotension, autonomic hyperreflexia and deep venous thrombosis, were also collected. Bowel and bladder function were assessed in terms of continence and voiding ability.
Data analysis
Data analysis was performed with Stata 11. Descriptive results are provided for patient demographic and neurological injury data; timing of rescue, spinal surgical stabilization, and rehabilitation intervention; and for selected functional rehabilitation outcomes.
A mixed effects regression employing random intercepts for patients and hospitals was used to model rehabilitation effectiveness. Selected predictors were age, gender, neurological level (a single predictive dummy variable representing lesions above T7 was used to avoid statistical overfitting), time to rescue, time to beginning of rehabilitation, rehabilitation programming, and an interaction term multiplying time to rescue and time to rehabilitation for the second measurement point (otherwise set to zero). This estimation was repeated on 100 bootstrap samples to enhance the stability of estimation results due to the small sample size (11). These final results were used to predict MBI scores and 99% confidence intervals (CI) for the beginning and end of rehabilitation programming to demonstrate rehabilitation effectiveness. Moreover, we used the model estimates to predict MBI scores and Bonferroni-corrected 95% CI at the beginning and end of rehabilitation, respectively, for victims who were rescued from the rubble within 30 min or later and for persons who began rehabilitation within 3 months of the earthquake or later. The Stata command “margins” was used to obtain the prediction at group means of all other variables. Standard errors of the prediction were calculated with the delta method (12).
Outcomes of medical complication management are represented in this study as treatment effectiveness, which was calculated as the percentage of patients with a complication at the beginning of rehabilitation who did not have the complication at the end of rehabilitation.
RESULTS
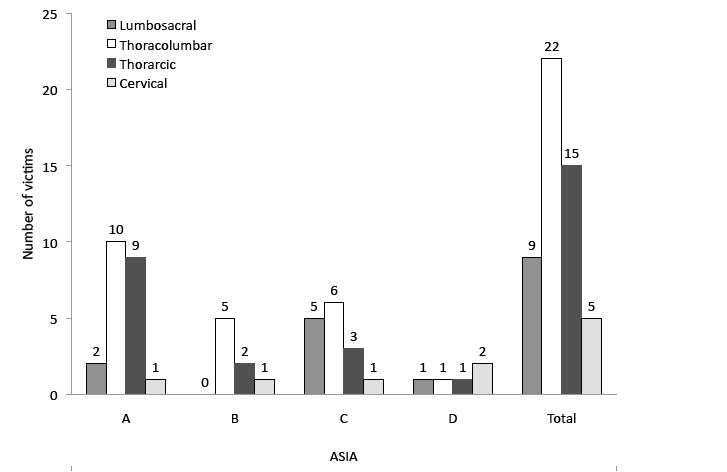
The mean age of the enrolled population was 38.5 years (standard deviation 9.6) (age range 11–77 years; with the majority of persons between 18 and 60 years of age (n = 38 (75%)). The male:female ratio was approximately 1:1.4 (n = 21 and n = 30, respectively). Of the 51 SCI cases, 43.1% (n = 22) were complete and 56.9% (n = 29) were incomplete injuries at the beginning of rehabilitation. Most patients had lesions at the thoracolumbar level (43%), with thoracic lesions accounting for the next highest incidence of injury (29%). Cervical lesions were least frequent (9%).
Fig. 1 shows patient AIS classification by level of lesion. Most patients with thoracic and thoracolumbar lesions were classified as AIS A, while lumbosacral lesions corresponded mostly to AIS C; the majority of cervical lesions were AIS D.
Fig. 1. Patient American Spinal Injury Association (ASIA) Impairment Scale (AIS) classification by level of lesion (victim totals). Note: one patient with conus medullaris symptoms could not be classified according to AIS.
Timing of rescue, spinal surgical stabilization and rehabilitation intervention
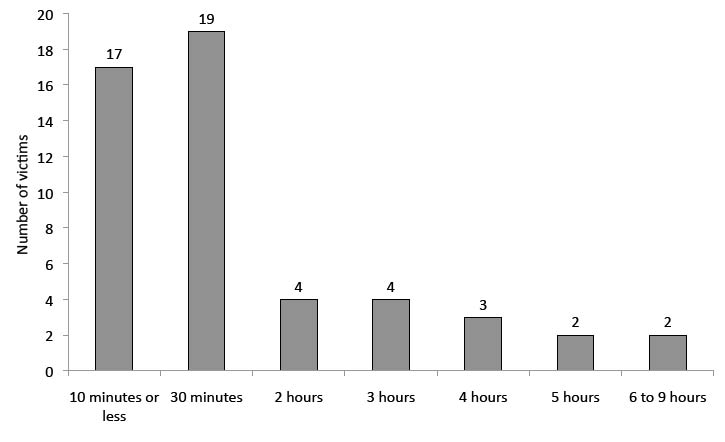
“Time to rescue” indicates elapsed time from the earthquake to extrication from disaster debris, as recorded on official responder and hospital records. Mean rescue time of our sample was 82 min (standard deviation (SD) 113), with a minimum of several minutes and a maximum of 9 h. Most victims were rescued from the debris within 30 min of the earthquake (n = 36; 70.6%) and all surviving victims within 9 h (n = 15) (Fig. 2).
Forty-four (86.3%) patients received surgical spinal stabilization; only 7 of these underwent surgery within 5 days after the earthquake. Of the 7 cases that were treated conservatively, an unstable spine was diagnosed in one patient (who received a subsequent operation). Three of the remaining 6 patients had complete paraplegia.
Fig. 2. Time to rescue (victim totals).
Only one patient began rehabilitation therapy within the first month following injury. Twenty-one patients (41.2%) began programming within 2 months, 36 (70.6%) by 3 months, 48 (94.1%) within 4 months, and 3 began rehabilitation afterwards.
Functional rehabilitation outcomes: Ambulation ability, wheelchair mobility and activities of daily living independence
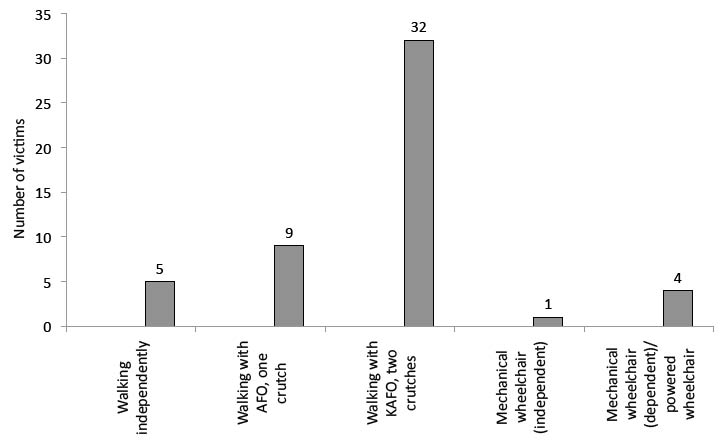
Forty-six patients (90%) resumed walking; 32 with KAFO (63%), 9 with AFO (18%) and 5 did not require orthoses (10%). The vast majority of patients (90.2%) who required use of a wheelchair (at least several times a day) could operate their wheelchair independently. Four cases (7.8%) who did not achieve wheelchair independence lacked sufficient hand function; two quadriplegics with cervical lesions, a patient with an amputated left arm, and another patient with a severe crush injury of the right hand (Fig. 3).
Fig. 3. Ambulation ability and wheelchair mobility (victim totals). AFO: ankle-foot orthosis; KAFO: knee-ankle-foot orthosis.
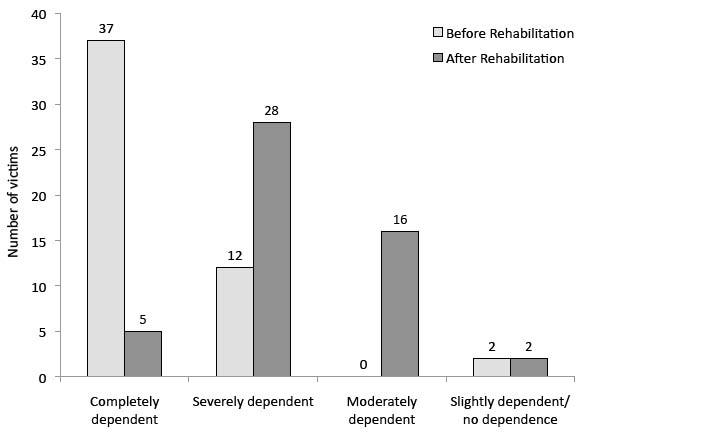
Patient unadjusted/raw MBI scores improved significantly, by a mean of 29 points (SD 16.9) during the course of rehabilitation programming. Three patients did not show any improvement; two of these had MBI values of 100 (scale ceiling) already on admission and the other was admitted 9 months post-injury (clinical focus of hospitalization was treatment of SCI complications). Based on MBI scores at the end of therapy, 18 patients (35.3%) achieved at least moderate ADL independence and 46 (90.2%) regained some self-care ability prior to discharge (Fig. 4). Five persons required full-time, attended care, including 2 complete cervical patients and 3 incomplete injury thoracolumbar cases with associated limb amputations, traumatic brain injury, and a crush injury of the hand. Bladder and bowel continence, toilet transfers, bathing, and climbing stairs were the main activity restrictions.
Fig. 4. Modified Barthel Index (MBI) dependence scores of the 51 spinal cord injury (SCI) patients before and after rehabilitation (victim totals).
Rehabilitation effectiveness
The results of the mixed effects regression (bootstrap estimation) are shown in Table I. Rehabilitation programming was the strongest predictor of significantly increased MBI scores. (“Rehabilitation programming” was a dummy variable constructed to measure the difference between MBI scores at the beginning and end of rehabilitation, and was referenced to the beginning of rehabilitation). Adjusting for all other factors, rehabilitation programming increased MBI by 34 points (95% CI 28–41). Greater age, female gender, and lesions above T7 correlated with lower MBI scores. A combination of prolonged times to rescue and rehabilitation corresponded to significantly decreased MBI scores.
| Table I. Mixed effects regression of Modified Barthel Index (MBI) on selected predictors |
| | B | SE | Beta | 95% CI | p |
| Age | –0.199 | 0.095 | –2.08 | –0.385 to –0.012 | 0.037 |
| Female | –9.637 | 3.849 | –2.50 | –17.182 to –2.092 | 0.012 |
| Lesion level above T7 | –17.358 | 4.792 | –3.62 | –26.750 to –7.966 | < 0.001 |
| Time to rescue (min) | –0.004 | 0.020 | –0.19 | –0.044 to 0.035 | 0.848 |
| Time to rehabilitation (days) | 0.026 | 0.072 | 0.36 | –0.115 to 0.168 | 0.716 |
| Rehabilitation programming | 34.408 | 3.428 | 10.04 | 27.690 to 41.126 | < 0.001 |
| Time to rescue × time to rehabilitation × rehabilitation programming | –0.006 | 0.003 | –2.06 | –0.001 to –0.00003 | 0.040 |
| Intercept | 37.605 | 9.111 | 4.13 | 19.746 to 55.464 | < 0.001 |
| B: unstandardized parameter; SE: standard error; Beta: standardized parameter; CI: confidence interval of B. Note: 102 observations; estimation repeated over 100 bootstrap samples; Baysean Information Criterion = 918.65. |
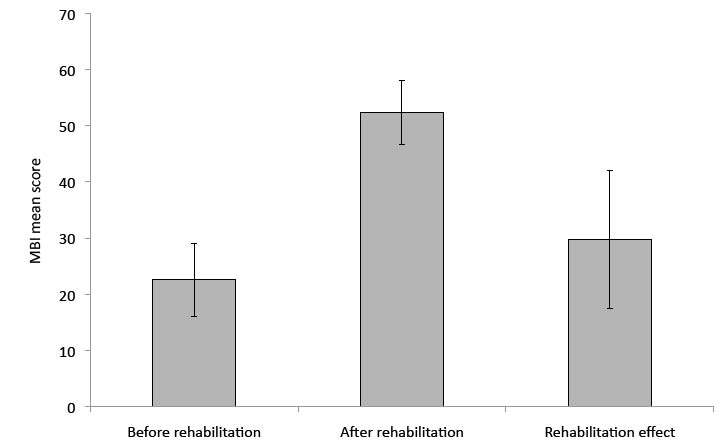
Fig. 5 shows the effectiveness of rehabilitation, as demonstrated by the increase in MBI scores using a marginal prediction, adjusted at means of the independent variables before and after rehabilitation, respectively (implying zero influence of the interaction of rescue time and time to rehabilitation at baseline). The adjusted MBI mean score at the beginning of rehabilitation was 23 (99% CI: 16–29) and 52.35 at the end of rehabilitation (99% CI: 47–58), yielding a predicted mean improvement of 30 points (99% CI: 18–42). This significant increase corresponds to a decrease in functional dependence from complete dependence to upper range severe dependence.
Fig. 5. Predicted average Modified Barthel Index (MBI) scores at the beginning and end of rehabilitation and the mean rehabilitation effect (absolute totals). Error bars represent 99% confidence intervals. Prediction is adjusted for age, gender, lesion level, time to rescue, time to rehabilitation, and the combined effect of time to rescue and time to rehabilitation.
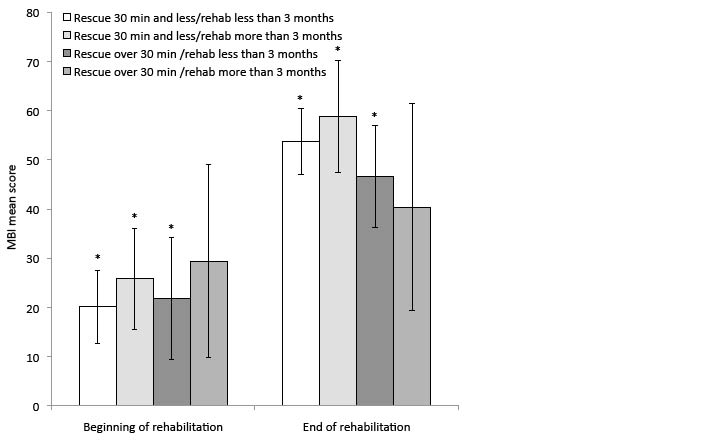
Fig. 6 shows the combined predicted effect of time to rescue and time to the beginning of rehabilitation on rehabilitation effectiveness. Significant improvement in MBI scores during institutional rehabilitation is achieved by groups who were rescued from the rubble in 30 min or less and/or who received rehabilitation treatment within 3 months after the earthquake. The group that began rehabilitation more than 3 months after the earthquake and whose members were not rescued within 30 minutes of the earthquake had the lowest scores and did not show significant improvement. Nonetheless, a small treatment effect is also visible in this group.
Fig. 6. Predicted mean Modified Barthel Index (MBI) scores at the
beginning and end of rehabilitation programming for different combinations of time to rescue and time to rehabilitation (absolute totals). (Error bars represent 95% Bonferroni corrected confidence intervals.) Prediction is adjusted for age, gender, lesion level, and the interaction of time to rehabilitation × time to rescue × rehabilitation. *Significance at p < 0.05 for the difference in MBI scores before and after rehabilitation.
Medical complications and management outcomes
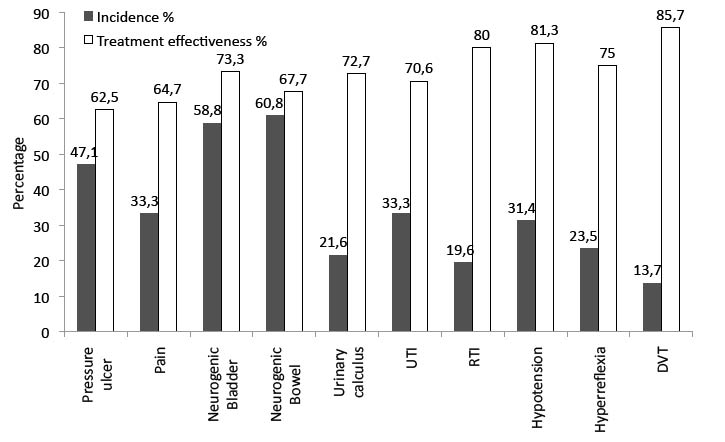
The most common complications were bowel and bladder dysfunction (60.8% and 58.8%, respectively). The significant majority of these patients achieved continence by clinical criteria. All patients with thoracic spine injuries or below learned to manage their bowel and bladder functions independently. Pressure ulcers occurred in nearly half of the sample, more than one-third of which had not healed by the end of rehabilitation. Urinary calculi and infections were common. Pain, respiratory infections, postural hypotension and autonomic hyperreflexia occurred primarily in patients injured at the thoracolumbar level and above (Fig. 7).
Fig. 7. Incidence of medical complications and treatment effectiveness of management outcomes (percentage). Treatment effectiveness is defined as the percentage of patients with a respective complication at the beginning of rehabilitation who completed rehabilitation without the complication. UTI: urinary tract infection; RTI: respiratory tract infection; DVT: deep vein thrombosis.
DISCUSSION
Most victims in this series of 51 SCI survivors of the 2008 Sichuan earthquake had either thoracolumbar or thoracic AIS A injuries at the beginning of rehabilitation. Relatively fewer cervical injuries can possibly be explained by victims not surviving the initial trauma or avoidance of upper spine injury by using defensive arm and hand posturing. By analogy, the high incidence of thoracolumbar and thoracic injuries is presumably due to blunt trauma from falling debris sustained in a protective standing or a sitting position during daytime, working hours. This spinal injury pattern corresponds to that reported in previous earthquakes (4, 13).
This study showed that institution-based, individualized physical rehabilitation programming in SCI patients was effective in improving functional rehabilitation outcomes including ambulation ability, wheelchair mobility and ADL independence. These findings generally agree with an earlier qualitative report of improved outcomes in SCI patients treated in hospitals under physiatrist supervision, compared with hospitals without involvement of physiatrists, following the 2005 Pakistan earthquake (14). However, comparison studies of higher methodological quality, showing improved functional outcomes due to rehabilitation intervention in natural disasters, are not available (15).
Rehabilitation programming was the strongest predictor (as reflected by a significant increase in MBI scores) of improved functional rehabilitation outcomes, which was manifest by decreased functional dependency. Less reliance on family members and other caregivers reduces the burden of care and is associated with decreased physical and psychological disability, as well as improved quality of life for persons with SCI (16). A significant majority of SCI survivors in this study population resumed walking with aids, and nearly all of those who required the use of a wheelchair could operate it without assistance by the end of rehabilitation. However, most were discharged back to mountainous, rural areas with poor roads, inaccessible public transportation, and non-inclusive homes. Home adaptations and other environmental barrier modifications complemented by community-based rehabilitation programming are needed to provide the medical and additional services and supports needed for optimal community reintegration (17).
Mountainous terrain, poor roads, and disaster debris, as well as lapses in coordination, including disrupted communication slowed medical team response, rescue, and hospital referral in the most severely earthquake-affected areas (18, 19). In another series of Sichuan earthquake victims with spinal injuries including SCI, several of whom sustained critical, co-morbid conditions including crush syndrome with acute renal failure (requiring evacuation to nearby West China Hospital for stabilizing care instead of a distant tertiary hospital), mean extrication time was 12.2 h (20). Mean rescue time was only 1.3 h in our sample; however, this was due primarily to less severe injuries. Longer time to rescue combined with longer time to rehabilitation in our study, resulted in the lowest MBI scores with no significant improvement in rehabilitation effectiveness. This finding corresponds to previous studies, in which rehabilitation effectiveness was found to be inversely related to time to rescue and time to rehabilitation (21, 22). Significant improvement in MBI scores with rehabilitation was, in fact, achieved by groups that were rescued from the rubble within 30 min and/or received rehabilitation no later than 3 months after the injury; the group that was rescued and began rehabilitation relatively later showed the smallest improvement. These findings are consistent with common assumptions about neural plasticity and optimal windows of opportunity for rehabilitation (23).
Study subjects experienced a relatively high incidence of medical complications on enrolment due, in part, to lack of preventive rehabilitation measures and formal rehabilitation programming practiced at the transferring hospitals (24). Injuries were also exacerbated by difficult conditions during the lengthy transfer between facilities. Patients also received less intensive rehabilitation therapy at the study hospitals while being treated in other departments for their severe injuries prior to transfer to the rehabilitation department.
Training for neurogenic bowel and bladder, the most common complications, was successful in most cases. Although the pre-study incidence of pressure sores was higher than that noted in other research with Chinese SCI patients (25, 26), few new sores occurred after the beginning of rehabilitation programming and most ulcers were healed with basic wound care by the end of rehabilitation. Wound contamination prior to rescue, inadequate wound care at field medical stations, long-distance transport to initial tertiary hospitals (and later to study hospitals) in compromised body positions, and poor nutrition probably contributed. Pressure sore prevention in SCI patients during disaster deserves greater emphasis, since treatment is not complicated, while medical co-morbidities are significant.
Urinary tract infection is, in general, the most common secondary complication in SCI patients (27) and one-third of patients in this study were affected. Adequate water intake, appropriate antibiotic usage, and proper intermittent clean catheterization technique effectively treated our population. Pain is a significant complication in SCI patients due to its perceived effect on quality of life and relationship to biopsychosocial factors (28). Pain improvement in our population can be attributed to the practice of effective protocols by hospital staff. Treatment effectiveness was highest for deep vein thrombosis which also had the lowest incidence. This finding agrees with other research (4) and was probably due to rehabilitation department admission well beyond the 7–10-day high-risk, post-injury period (29).
This study was limited by its small sample size, which precluded consideration of additional predictive variables, such as AIS classification in the mixed regression analysis. Furthermore, the effect of spontaneous neurological recovery on rehabilitation effectiveness cannot be determined in this observational study due to lack of a control group. Unobserved inter-institution variability in rehabilitation programming was controlled by introducing random intercepts for the different hospitals. In addition, a number of potential confounders were statistically adjusted for in the predictive model. The bootstrap method (11) was used to improve the stability of estimation results for rehabilitation effectiveness. Conservative 99% CIs were used for the prediction.
Future studies on the effectiveness of specific rehabilitative therapies and related outcome measures are needed. Since randomized controlled trials of rehabilitation interventions are unethical, but scientifically optimal, improved modelling of rehabilitation outcomes after earthquakes is indicated; analysis of simulated data with counterfactual distributions, for example (30). Future investigation of effective enabling, inclusive environmental solutions and community-based rehabilitation programming is necessary to optimize quality of life and community reintegration for Sichuan SCI survivors and victims of future earthquakes (31).
In conclusion, this study demonstrates the effectiveness of institutional, individualized physical rehabilitation programming on functional rehabilitation outcomes in a series of SCI victims from the 2008 Sichuan earthquake. Ambulation ability, wheelchair mobility, and ADL independence were significantly improved. The significance of early commencement of rehabilitation therapy was demonstrated, while longer time to rehabilitation, coupled with increased time to rescue, was shown to be relatively ineffective. Most medical complications were managed effectively.
ACKNOWLEDGEMENTS
The authors are grateful for support for this research from the Earthquake Victims’ Rehabilitation Center of West China Hospital, Mianzhu County Hospital, and Jiangyou Orthopedic Hospital, Sichuan, China. The authors are also grateful to Dr S. Y. Lee for his editorial assistance and Bernie A. G. Fellinghower for statistical advice.
REFERENCES