Jasmijn F. M. Holla, MSc1, Marike van der Leeden, PT, PhD1,2,3, Wilfred F. H. Peter, PT1,4, Leo D. Roorda, MD, PhD1, Martin van der Esch, PT, PhD1, Willem F. Lems, MD, PhD5,6, Martijn Gerritsen, MD, PhD5, Ramon E. Voorneman, MD, MSc5, Martijn P. M. Steultjens, PhD7 and Joost Dekker, PhD1,2,3,8
From the 1Amsterdam Rehabilitation Research Center/Reade, Amsterdam, 2Department of Rehabilitation Medicine, VU University Medical Center, Amsterdam, 3EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam, 4Department of Rheumatology, Leiden University Medical Center, Leiden, 5Jan van Breemen Research Institute/Reade, Amsterdam, 6Department of Rheumatology, VU University Medical Center, Amsterdam, The Netherlands 7Institute for Applied Health Research and School of Health and Life Sciences, Glasgow Caledonian University, Glasgow, UK and 8Department of Psychiatry, VU University Medical Center, Amsterdam, The Netherlands
OBJECTIVE: To establish whether proprioception and varus-valgus laxity moderate the association between muscle strength and activity limitations in patients with early symptomatic knee osteoarthritis.
DESIGN: A cross-sectional study.
SUBJECTS: A sample of 151 participants with early symptomatic knee osteoarthritis from the Cohort Hip and Cohort Knee study.
METHODS: Regression analyses were performed to establish the associations between muscle strength, proprioception (knee joint motion detection threshold in the anterior-posterior direction), varus-valgus laxity and activity limitations (self-reported and performance-based). Interaction terms were used to establish whether proprioception and laxity moderated the association between muscle strength and activity limitations.
RESULTS: Proprioception moderated the association between muscle strength and activity limitations: the negative association between muscle strength and activity limitations was stronger in participants with poor proprioception than in participants with accurate proprioception (performance-based activity limitations p = 0.02; self-reported activity limitations p = 0.08). The interaction between muscle strength and varus-valgus laxity was not significantly associated with activity limitations.
CONCLUSION: The results of the present study support the theory that in the absence of adequate proprioceptive input, lower muscle strength affects a patient’s level of activities to a greater degree than in the presence of adequate proprioceptive input.
Key words: knee osteoarthritis; activity limitations; muscle strength; proprioception; varus-valgus laxity.
J Rehabil Med 2012; 00: 00–00
Correspondence address: Jasmijn Holla, Amsterdam Rehabilitation Research Center Reade, Dr. Jan van Breemenstraat 2, NL-1056 AB Amsterdam, The Netherlands. E-mail: j.holla@reade.nl
Submitted November 17, 2011; accepted May 22, 2012
INTRODUCTION
Osteoarthritis (OA) of the knee is a leading cause of activity limitations (e.g. stair-climbing, walking) in Western countries (1–3), and an important physical determinant of activity limitations is muscle strength (4, 5). Lower muscle strength is a major cause of activity limitations, since muscle strength is needed for all activities of daily living (4, 6). Recent evidence points out that proprioception and varus-valgus laxity moderate (i.e. alter the strength of) the association between muscle strength and activity limitations (4, 7, 8). Thus, lower muscle strength is associated with activity limitations, and the strength of this association is influenced by proprioception and varus-valgus laxity.
Proprioception can be defined as the conscious and unconscious perception of joint movement and joint position (9, 10). This perception depends on afferent receptors in the muscles, ligaments, synovial capsule and skin, and is influenced by visual, auditory and vestibular inputs (11). Proprioception activates and modulates muscles in order to stabilize the joint and to produce controlled joint movements (8). Stable knees that do not give way are essential for executing daily activities. Studies have demonstrated that proprioception is poor in patients with knee OA compared with healthy controls (12). As far as we know, only one study has examined the influence of proprioception on the association between muscle strength and activity limitations: van der Esch et al. (8) demonstrated that the association between muscle strength and activity limitations is stronger in knee OA patients with poor proprioception than in patients with accurate proprioception. They concluded that in the absence of adequate neuromuscular control through poor proprioceptive input, muscle strength affects a patient’s level of activities to a greater degree (8).
Varus-valgus laxity of the knee joint is defined as the displacement or rotation of the tibia with respect to the femur in the varus-valgus direction (7, 13). The degree of varus-valgus laxity is determined largely by the passive restraint system (i.e. ligaments and joint capsule). Besides muscle strength and proprioception, the passive restraint system contributes to the stability of the knee joint (7). Two studies compared the degree of varus-valgus laxity in knee OA patients with that in healthy controls: one study reported higher laxity in OA patients (14), whereas the other study reported no difference (15). Two studies have examined the influence of joint laxity on the relationship between muscle strength and activity limitations in knee OA (7, 13). These studies reported opposite results. Sharma et al. (13) found a weaker relationship between muscle strength and activity limitations in patients with greater varus-valgus laxity. They concluded that in the presence of a given level of varus-valgus laxity, muscle strength makes a smaller contribution to maintenance of activities than it does in patients with more stable knees (13). Van der Esch et al. (7) found a stronger relationship between muscle strength and activity limitations in patients with greater varus-valgus laxity. They concluded that in patients with high joint laxity, muscle strength around the knee compensates for the loss of stability provided by the passive restraint system (7). It is assumed that the discrepancy in results between the two studies is attributable mainly to the difference in analytical approach (7). We prefer the analytical approach used by van der Esch et al. (7), because they analysed the data of all patients in one regression analysis using a continuous measure for laxity, whereas Sharma et al. (14) compared the correlation between muscle strength and activity limitations in a high laxity group with that in a low laxity group.
The influence of proprioception (8) and varus-valgus laxity (7) on the association between muscle strength and activity limitations might be explained by compensation mechanisms within the processes of joint stabilization and neuromuscular control. Muscle actions can compensate for lack of adequate passive stabilization and poor proprioception as long as there is sufficient muscle strength available. When there is insufficient muscle strength available, the muscles are unable to perform the dual task of stabilizing the joint and producing the movements necessary to perform physical activities. This will result in increased activity limitations.
As described above, previous research (7, 8, 13) on these associations have reported conflicting findings. Consequently, there is need for further research, especially into early symptomatic OA, because in this patient group these associations have not yet been examined. If inaccurate proprioception and high varus-valgus laxity influence the relationship between muscle strength and activity limitations, this would have implications for the content of, and expectations regarding, exercise therapy in the individual patient with knee OA. It is possible that tailored exercise interventions for patients with inaccurate proprioception or high knee joint laxity in an early stage of the disease lead to better outcomes. Therefore, the aim of the present study was to establish whether proprioception and varus-valgus laxity moderate the association between muscle strength and activity limitations in patients with early symptomatic knee OA. It was hypothesized that: (i) the association between muscle strength and activity limitations is stronger in patients with poor proprioception than in patients with accurate proprioception; and that (ii) the association between muscle strength and activity limitations is stronger in patients with high varus-valgus laxity than in patients with low varus-valgus laxity.
PATIENTS AND METHODS
Study population
A cross-sectional study was conducted in a sample of 151 participants with early symptomatic knee OA from the Cohort Hip and Cohort Knee (CHECK) study (16). CHECK is a prospective cohort study of 1,002 individuals with early symptomatic OA of the knee or hip. On entry, all participants had pain or stiffness of the knee or hip, and were aged 45–65 years. They had not yet consulted their physician for these symptoms, or the first consultation was within 6 months before entry. Participants with any other pathological condition that could explain the symptoms were excluded (e.g. other rheumatic disease, previous hip or knee joint replacement, congenital dysplasia, osteochondritis dissecans, intra-articular fractures, septic arthritis, Perthes’ disease, ligament or meniscus damage, plica syndrome, Baker’s cyst). Additional exclusion criteria were: comorbidity that did not allow physical evaluation and/or follow-up of at least 10 years, malignancy in the last 5 years, and inability to understand the Dutch language.
The CHECK cohort was formed from October 2002 till September 2005. At baseline, the majority of this cohort (83%) reported knee symptoms, of whom 76% fulfilled the clinical American College of Rheumatology (ACR) criteria for knee OA (17). Hip symptoms were reported by 59% of participants, of whom 24% fulfilled the clinical ACR criteria for hip OA (18). At baseline, none of the participants had radiographic OA (i.e. Kellgren and Lawrence grade (KL-grade) ≥ 2) (19). Two-year follow-up data show an increase in radiographic signs: 19% of the participants with knee symptoms had radiographic knee OA and 6% of the participants with hip symptoms had radiographic hip OA. Therefore the CHECK cohort can be considered as an early symptomatic OA cohort. Nationwide, 10 general and academic hospitals in the Netherlands are participating, located in urbanized and semi-urbanized regions. General practitioners (GP) in the surroundings of the participating centres were invited to refer eligible persons. All patients who visited the GP on their own initiative, potentially fulfilling the inclusion criteria, were referred to 1 of the 10 participating centres. In addition, participants were recruited through advertisements and articles in local newspapers and on the Dutch Arthritis Association website. The physicians in the participating centres checked whether referred patients, as well as patients from their outpatient clinics, fulfilled the inclusion criteria.
All participants with knee symptoms recruited through Reade, Center for Rehabilitation and Rheumatology, in Amsterdam (n = 151) were additionally invited to participate in the present study. Additional measurements (muscle strength, joint proprioception, varus-valgus laxity and a performance-based measure of activity limitations) were integrated in the existing measurement schedule for CHECK at the two-year follow-up visit. The CHECK study was approved by the medical ethics committees of all participating centres. The additional measurements necessary for the present study were approved by the Medical Ethical Committee of the Slotervaart Hospital and Reade, Center for Rehabilitation and Rheumatology. All participants gave their written informed consent before entering the study.
Activity limitations
Activity limitations were assessed with both a self-report measure and a performance-based measure. Self-reported activity limitations were assessed with the physical functioning subscale of the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC-PF) (20, 21). This subscale consists of 17 items, which assess the degree of difficulties one has in executing activities. Items are answered on a 5-point scale. The sum of scores on all 17 items is used as the score for activity limitations. Scores range from 0 to 68, with higher scores indicating more activity limitations. The WOMAC is widely used in clinical research, and has been shown to be reliable, valid and responsive for use in patients with OA (20–22).
Performance-based activity limitations were assessed with a timed stair-climbing test. The stairs had 12 steps with a rise of 16 cm and a run of 30 cm. Participants began the task by standing on a line 58 cm from the first step. Participants were instructed to climb the stairs step by step as quickly as they felt safe and comfortable. They were encouraged not to use the handrail, but were not prohibited for doing so for safety. The task ended when participants stood with both feet upstairs. The task was scored as the total time needed to climb the stairs. A longer time to complete the task indicates more activity limitations. Excellent test-retest reliability was reported for a comparable stair-climbing task in patients with knee OA (23).
Muscle strength, proprioception and varus-valgus laxity
A single physical therapist assessed all participants according to a standardized protocol. Muscle strength in Newton metre (Nm) of the upper leg (quadriceps and hamstrings) was assessed using an isokinetic dynamometer (EnKnee; Enraf-Nonius, Rotterdam, the Netherlands). Measurements were made in sitting position at an angular velocity of 60º per s, which reflects a speed of movement usually applied during daily tasks, e.g. walking. This method has been shown to yield reproducible and valid results (24, 25). Following instruction, participants performed 1 test measurement. After a 30-s rest participants performed 3 maximal quadriceps strength measurements during knee extension, and 3 maximal hamstrings strength measurements during knee flexion. For analysis the maximum voluntary contraction obtained from 3 measurements of the quadriceps and from 3 measurements of the hamstring muscles of the index knee (most affected knee) were summed and divided by 2 to obtain a measure of total muscle strength around the index knee (5). The measure was corrected for weight by dividing it by the participant’s weight. Participants identified their most affected (index) knee in the clinical interview (n = 47). For participants with bilateral symptoms we defined an index knee based on the following decision tree: (i) highest KL-grade (19); (ii) lowest degree of active knee flexion; (iii) highest pain during active knee flexion; and (iv) crepitus during knee flexion (n = 93). In participants for whom we could not define an index knee based on these signs, we randomly assigned an index knee (n = 11).
Proprioception was measured using a device based on a description by Pai et al. (26). The device consisted of a chair with a computer-controlled motor and transmission system and two attached free-moving arms. Each arm supported the subject’s shank and foot and moved in the sagittal plane. Participants were seated with the knees in 90º flexion. An arm attached to the device forced the knee towards extension at a speed of 0.3º per s. Participants were asked to push a button the moment they perceived a change in the position of the knee joint. The difference in knee angle between the starting position and the position at the moment the participant pushed the button (i.e. the joint motion detection threshold) was used as an indicator for proprioception. The mean joint proprioception obtained from 3 measurements of the index knee was used for analysis. This method has been shown to yield reproducible and valid results (8, 10, 27).
Laxity was measured using a device consisting of a chair with an attached free moving arm. The arm supported the patient’s shank and moved the shank across the transverse axis of the knee joint, in the frontal plane. Participants were seated with the thigh, shank and ankle immobilized. The knee was in 20º flexion. A weight of 1.12 kg that was attached to the free-moving arm was used to load the lower leg. This weight was attached by a cord 0.68 m from the pivot, resulting in a net moment on the knee of 7.7 Nm. The load could be applied to the lower leg both medially and laterally, resulting in a varus or valgus rotation of the knee in the frontal plane. The sum of the varus and valgus deviations was taken as the knee joint laxity score. The mean knee joint laxity obtained from 3 measurements of the index knee was used for analysis. This method has been shown to yield reproducible results (28).
Additional measures
Additional data recorded were age, gender, body mass index, the duration of knee symptoms, the ACR clinical criteria for knee OA (17), the KL-grade for radiographic knee OA (19), pain (numeric rating scale for pain during the last week (NRS pain) and pain subscale of the WOMAC (20)), and stiffness (stiffness subscale of the WOMAC (20)).
Statistical analysis
Separate analyses were performed for the self-report (WOMAC-PF) and performance-based (timed stair-climbing test) outcome measure of activity limitations. Linear regression analyses were performed to assess the associations between muscle strength, proprioception and activity limitations. Prior to the analyses we checked whether the assumptions for linear regression (e.g. no strong multicollinearity (Pearson’s correlation coefficient (r) < 0.80), homoscedasticity, linearity) were met (29). First regression models were built with muscle strength as independent variable and activity limitations as dependent variable. Secondly, proprioception was added as independent variable to the models. Thirdly, moderation of proprioception was assessed by adding an interaction term between muscle strength and proprioception (muscle strength × proprioception) to the models. Fourthly, confounding of age, gender, duration of symptoms, NRS pain and varus-valgus laxity was assessed by adding these variables as covariables to the models. An added covariable was considered to be a confounder if the regression coefficient (B) of the interaction term changed with >10%. Subsequently, the same analyses were performed for varus-valgus laxity. In step 4 of these analyses we assessed confounding of proprioception instead of varus-valgus laxity. Results were considered statistically significant at p < 0.05.
The independent variables muscle strength, proprioception and varus-valgus laxity were centred around the mean. An interaction term is often highly correlated with the independent variables of which it is comprised. Centring reduces multicollinearity: when the independent variables are centred, the only remaining correlation between the independent variables and the product term is that due to non-normality (30). In addition, centring allows for a meaningful interpretation of main effects because centring alters the meaning of the intercept term (30). When the independent variables are centred the regression coefficient of an independent variable is the effect of this variable on the outcome variable for a person who is average on all other independent variables.
RESULTS
Study population
Characteristics of the study population are presented in Table I. The study population comprised 151 participants (120 women and 31 men) with a mean age of 58.5 years. The majority of participants (68.9%) reported bilateral knee symptoms. The median knee symptom duration was 3.7 years, 78.1% of participants fulfilled the ACR clinical criteria for knee OA, and 19.2% had radiographic knee OA. The median score for self-reported activity limitations (WOMAC-PF) was 13, and the median score for the timed stair-climbing test was 4.6 s.
| Table I. Characteristics of the study population (n = 151) |
| Characteristics | Value |
| Age, years, mean (SD) | 58.5 (5.0) |
| Female, n (%) | 120 (79.5) |
| Body mass index, kg/m2, mean (SD) | 25.6 (3.8) |
| Knee symptoms, n (%) | |
| Unilateral | 47 (31.1) |
| Bilateral with index knee | 93 (61.6) |
| Bilateral with equal symptoms | 11 (7.3) |
| Duration of knee symptoms, years, median (IQR) | 3.7 (2.8–5.0) |
| Clinical knee OA (ACR criteria), n (%) | 118 (78.1) |
| KL-grade ≥ 2, n (%) | 29 (19.2) |
| Numeric rating scale for pain during the last week, range: 0–10, median (IQR) | 3.0 (2.0–5.0) |
| WOMAC pain score, range: 0–20, median (IQR) | 5.0 (2.0–7.0) |
| WOMAC stiffness score, range: 0–8, median (IQR) | 3.0 (2.0–4.0) |
| WOMAC physical function score, range: 0–68, median (IQR) | 13.0 (7.0–22.0) |
| Timed stair climbing test, s, median (IQR) | 4.6 (4.1–5.6) |
| Muscle strengtha of the index knee, Nm/kg, mean (SD) | 1.0 (0.3) |
| Proprioception of the index knee, degrees, median (IQR) | 2.4 (1.6–3.9) |
| Varus-valgus laxity of the index knee, degrees, median (IQR) | 11.1 (8.4–14.6) |
| aMaximum contraction of the quadriceps and hamstring muscles averaged and divided by weight. IQR: interquartile range; SD: standard deviation; OA: osteoarthritis; ACR: American College of Rheumatology; KL-grade: Kellgren and Lawrence grade; WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index. |
Moderation of proprioception
The results of the analyses to test moderation of proprioception are presented in Table II. Univariable regression analyses (models 1) showed that muscle strength was negatively associated with both outcome measures of activity limitations (WOMAC-PF: B = –16.06, p < 0.001; timed stair-climbing test: B = –2.68, p < 0.001). When proprioception was added to the models (models 2), muscle strength was still negatively associated with activity limitations (WOMAC-PF: B = –13.94, p < 0.001; timed stair-climbing test: B = –2.45, p < 0.001). Proprioception (a higher score indicates less accurate proprioception) was positively associated with activity limitations (WOMAC-PF: B = 0.97, p = 0.002; timed stair-climbing test: B = 0.12, p = 0.02).
| Table II. Results of the regression of activity limitations (WOMAC physical function and timed stair-climbing test) on muscle strength and knee proprioception |
| Model | Independent variables | WOMAC physical function | | Timed stair-climbing test |
| B | 95% CI | p | | B | 95% CI | p |
| 1 | Muscle strength | –16.06 | –21.29 to –10.83 | < 0.001 | | –2.68 | –3.55 to –1.82 | < 0.001 |
| 2 | Muscle strength | –13.94 | –19.16 to –8.71 | < 0.001 | | –2.45 | –3.33 to –1.57 | < 0.001 |
| | Proprioception | 0.97 | 0.35 to 1.59 | 0.002 | | 0.12 | 0.02 to 0.23 | 0.02 |
| 3 | Muscle strength | –15.17 | –20.54 to –9.81 | < 0.001 | | –2.73 | –3.62 to –1.83 | < 0.001 |
| | Proprioception | 0.64 | –0.09 to 1.36 | 0.08 | | 0.05 | –0.07 to 0.17 | 0.45 |
| | Muscle strength × proprioception | –2.17 | –4.60 to 0.27 | 0.08 | | –0.50 | –0.90 to –0.10 | 0.02 |
| Independent variables are centred around the mean. None of the confounders examined (i.e. age, gender, duration of knee symptoms, numeric rating scale for pain, varus-valgus laxity) changed the B of the interaction term muscle strength × proprioception with more than 10%. WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; CI: confidence interval. |
The moderation analyses (models 3) showed that the interaction between muscle strength and proprioception was significantly associated with performance-based activity limitations (timed stair-climbing test: B = –0.50, p = 0.02). The analysis with self-reported activity limitations as outcome measure showed a trend in the same direction (WOMAC-PF: B = –2.17, p = 0.08). This implies that in participants with poor proprioception muscle strength was stronger associated with activity limitations than in participants with accurate proprioception. Adjustment for age, gender, duration of knee symptoms, pain and varus-valgus laxity did not change the B of the interaction term muscle strength × proprioception with more than 10%.
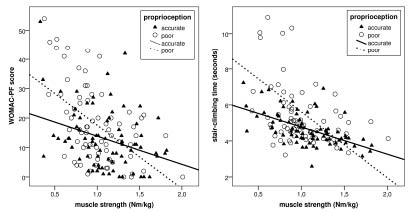
To visualize the interaction between muscle strength and proprioception, proprioception was dichotomized into poor proprioception (joint motion detection threshold ≥ 2.4º) and accurate proprioception (joint motion detection threshold < 2.4º), using the median-split method (see Fig. 1).
Fig. 1. Association between activity limitations and muscle strength in an accurate proprioception group (low joint motion detection threshold < 2.4º) and a poor proprioception group (high joint motion detection threshold > 2.4º).
Moderation of varus-valgus laxity
The results of the analyses to test moderation of varus-valgus laxity are presented in Table III. Multivariable regression analyses with muscle strength and varus-valgus laxity as independent variables and activity limitations as outcome variable (models 2) showed that muscle strength was negatively associated with both measures of activity limitations (WOMAC-PF: B = –17.04, p < 0.001; timed stair-climbing test: B = –2.71, p < 0.001). Laxity was only significantly associated with self-reported activity limitations (WOMAC-PF: B = –0.44, p = 0.01), not with performance-based activity limitations (timed stair-climbing test: B = –0.01, p = 0.65).
| Table III. Results of the regression of activity limitations (WOMAC physical function and timed stair-climbing test) on muscle strength and varus-valgus laxity |
| Model | Independent variables | WOMAC physical function | | Timed stair-climbing test |
| B | 95% CI | p | | B | 95% CI | p |
| 1 | Muscle strength | –16.06 | –21.29 to –10.83 | < 0.001 | | –2.68 | –3.55 to –1.82 | < 0.001 |
| 2 | Muscle strength | –17.04 | –22.22 to –11.86 | < 0.001 | | –2.71 | –3.59 to –1.84 | < 0.001 |
| | Laxity | –0.44 | –0.77 to –0.11 | 0.01 | | –0.01 | –0.07 to 0.04 | 0.65 |
| 3 | Muscle strength | –16.91 | –22.22 to –11.60 | < 0.001 | | –2.84 | –3.73 to –1.95 | < 0.001 |
| | Laxity | –0.44 | –0.78 to –0.11 | 0.01 | | –0.01 | –0.07 to 0.04 | 0.68 |
| | Muscle strength × laxity | 0.13 | –0.95 to 1.21 | 0.81 | | –0.13 | –0.31 to 0.05 | 0.15 |
| Independent variables are centred around the mean. Also after adjustment for age, gender, duration of knee symptoms, NRS pain and proprioception, the interaction between muscle strength and laxity was not significantly associated with activity limitations. WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index; CI: confidence interval. |
The moderation analyses (models 3) showed that the interaction between muscle strength and varus-valgus laxity was not significantly associated with activity limitations (WOMAC-PF: B = 0.13, p = 0.81; timed stair-climbing test: B = –0.13, p = 0.15), also not after adjustment for age, gender, duration of knee symptoms, pain and proprioception. This implies that varus-valgus laxity did not moderate the association between muscle strength and activity limitations.
DISCUSSION
The aim of the present study was to establish whether proprioception and varus-valgus laxity moderate the association between muscle strength and activity limitations in patients with early symptomatic knee OA.
The results of the study showed that the association between muscle strength and activity limitations was stronger in participants with poor proprioception than in participants with accurate proprioception. This finding confirms the results of a previous study of van der Esch et al. (8). The fact that we managed to replicate the findings of van der Esch et al. (8) strengthens the evidence for the theory that in the absence of adequate proprioceptive input, lower muscle strength affects a patient’s level of activities to a greater degree (8). The present study was performed in a population with early symptomatic knee OA, whereas the study of van der Esch et al. (8) was performed in 63 patients fulfilling the clinical ACR criteria for knee OA (38% had radiographic OA). The theory seems to be applicable to both populations. There are several mechanisms that could explain the interaction between muscle strength and proprioception. First, patients with weaker muscles may have less muscle mass and fewer proprioceptors, and consequently impaired proprioceptive input (31). Secondly, reduced sensitivity of the muscle spindles may play a role (12, 31). During activities, patients with weaker muscles use a relatively high percentage of their maximum force, resulting in higher contraction levels, and thereby reduced sensitivity of the muscle spindles, leading to impaired proprioceptive input (31). A third possible mechanism is fatigue. Patients with weaker muscles will fatigue faster, leading to impaired proprioceptive input (31).
Varus-valgus laxity was not found to moderate the association between muscle strength and activity limitations. This finding is not in accordance with previous studies in established knee OA. In 164 patients with radiographic knee OA, Sharma et al. (13) found a weaker association between muscle strength and activity limitations in patients with greater varus-valgus laxity. In 86 patients with clinical knee OA (of which 80% had radiographic OA), van der Esch et al. (7) found a stronger association between muscle strength and activity limitations in patients with greater varus-valgus laxity. In comparison with the study populations of Sharma et al. (13) and van der Esch et al. (7), our population was younger, had less severe radiographic OA, higher muscle strength, higher varus-valgus laxity, and reported less activity limitations. Possibly varus-valgus laxity influences the association between muscle strength and activity limitations only in patients whose muscles are not strong enough to compensate sufficiently for the loss of stability provided by the passive restraint system. Our study population may have been able actively to stabilize their joints with their relatively strong muscles, despite high varus-valgus laxity.
Muscle strength was strongly negatively associated with activity limitations, indicating a higher level of activity limitations in participants with weaker muscles. This finding is in accordance with studies in established OA (4, 5, 7, 8, 32, 33).
Proprioception was found to be directly positively associated with activity limitations. This finding indicates that participants with poor proprioception have a higher degree of activity limitations than participants with accurate proprioception. This is in agreement with 3 earlier studies in established OA, in which proprioception was measured using the same method (8, 26, 34). Also, in the majority of studies that measured proprioception with another method (i.e. a joint repositioning task), a direct association between poor proprioception and a higher degree of activity limitations was found (12, 35–39). Proprioception apparently affects activity limitations in two ways: (i) poor proprioception is directly associated with a higher degree of activity limitations; and (ii) poor proprioception strengthens the association between muscle strength and activity limitations.
In contrast to Sharma et al. (13) and van der Esch et al. (7), we found a negative association between varus-valgus laxity and activity limitations, indicating less activity limitations in participants with higher varus-valgus laxity. As earlier mentioned, this may be caused by differences in study populations (i.e. our population was younger and had less severe radiographic OA, higher muscle strength, higher varus-valgus laxity and a lower degree of activity limitations). However, our knowledge on the pathophysiology and course of varus-valgus laxity in knee OA patients is not sufficient to explain the different results.
Based on the results of the present study and earlier studies (5, 8, 12), it can be hypothesized that besides muscle strengthening exercises, proprioception exercises may reduce the degree of activity limitations in patients with early symptomatic knee OA. This may have implications for the content of exercise therapy in patients with early symptomatic knee OA. It is possible that tailored exercise interventions, in which specific proprioception exercises are combined with muscle strengthening exercises, may lead to better outcomes.
Some methodological issues need to be addressed. First, in the present study the reliability of the muscle strength, proprioception and laxity measurements was not tested. However, all measurements were taken by a single physical therapist according to a strict protocol. Previous studies have shown that the methods used yield reproducible and valid results (10, 24, 25, 28). Secondly, to visualize the interactions between muscle strength and proprioception, we dichotomized proprioception using the median-split method. Because there are no universal cut-offs to separate accurate proprioception from poor proprioception it is not known whether the cut-off value used is clinically relevant in early symptomatic knee OA. Thirdly, because the present study had a cross-sectional design no causal inferences can be made.
In conclusion, evidence was obtained for the theory that in the absence of adequate proprioceptive input, lower muscle strength affects a patient’s level of activities to a greater degree than in the presence of adequate proprioceptive input. The theory that in patients with high joint laxity, muscle strength around the knee compensates for the loss of stability provided by the passive restraint system could not be confirmed.
ACKNOWLEDGEMENTS
CHECK is funded by the Dutch Arthritis Association on the lead of a steering committee comprising 16 members with expertise in different fields of OA chaired by Professor J. W. J. Bijlsma and coordinated by J. Wesseling, MSc. Involved are: Erasmus Medical Center Rotterdam; Kennemer Gasthuis Haarlem; Leiden University Medical Center; Maastricht University Medical Center; Martini Hospital Groningen/Allied Health Care Center for Rheumatology and Rehabilitation Groningen; Medical Spectrum Twente Enschede/ Ziekenhuisgroep Twente; Reade, Center for Rehabilitation and Rheumatology (formerly Jan van Breemen Institute)/VU Medical Center Amsterdam; St Maartenskliniek Nijmegen; University Medical Center Utrecht and Wilhelmina Hospital Assen.
REFERENCES