Rachel Milte, Bachelor of Science (Honours)1, Julie Ratcliffe, PhD2, Michelle Miller, PhD1, Craig Whitehead, PhD3, Ian D. Cameron, MBBS, PhD, FACRM, FAFRM, (RACP)4 and Maria Crotty, PhD3
From the 1Department of Nutrition and Dietetics, 2Flinders Clinical Effectiveness, 3Department of Rehabilitation, Aged, and Extended Care, Flinders University, Adelaide and 4Rehabilitation Studies Unit, University of Sydney, Sydney, Australia
OBJECTIVE: To investigate the preferences of frail older people for individualised multidisciplinary rehabilitation to promote recovery from a hip fracture.
DESIGN: Discrete Choice Experiment.
SETTING: Acute and Rehabilitation Hospitals in Adelaide, South Australia.
Subjects: Eighty-seven patients with recent hip fracture (16 living in residential care facilities prior to fracture).
METHODS: Patients providing informed consent (or consenting family carer proxies in cases where patients were unable to provide informed consent (n = 10)) participated in a face to face interview following surgery to repair a fractured hip to assess their preferences for different configurations of rehabilitation programs.
RESULTS: Overall, participants expressed a strong preference for improvements in mobility and a willingness to participate in rehabilitation programs involving moderate pain and effort. However, negative preferences were observed for extremely painful interventions involving high levels of effort (2 h per day for 2 months). Subgroup analysis revealed consistently similar preferences according to place of residence (residential care vs community).
CONCLUSIONS: Improvements in mobility are highly valued by frail older people recovering from hip fracture, including those living in residential care. Further research should be directed towards achieving greater equity in access to rehabilitation services for the wide spectrum of patients attending hospital with hip fractures.
Key words: discrete choice experiment; hip fracture; older people; residential care; rehabilitation.
J Rehabil Med 2013; 45:
Guarantor’s address:  Professor Julie Ratcliffe, Flinders Clinical Effectiveness, Flinders University, GPO Box 2100, Adelaide 5001, South Australia. E-mail: Julie.ratcliffe@flinders.edu.au
Professor Julie Ratcliffe, Flinders Clinical Effectiveness, Flinders University, GPO Box 2100, Adelaide 5001, South Australia. E-mail: Julie.ratcliffe@flinders.edu.au
Submitted December 2, 2011; accepted July 11, 2012
Introduction
Hip fractures are amongst the most devastating consequences of osteoporosis and injurious accidental falls with around 25% of patients dying in the first year after fracture (1, 2), with only 40% returning to pre-fracture levels of mobility (2), and annual expenditures exceeding 400M AUD (3). Rehabilitation strategies for frail older people following hip fractures are still evolving. However, there is evidence to suggest that an individualised multidisciplinary rehabilitation programme is associated with improvements in mobility relative to usual orthopaedic care (4). A previous study by Salkeld and colleagues (5) to assess the preferences for health of older women at risk of hip fracture living in the community indicated that even a small improvement in mobility was very highly valued and could have a large positive impact on quality of life. Whilst a rehabilitation programme has the ability to achieve large improvements in mobility (6), typically this also involves a period of substantial effort and endurance by the individual participant, as well as the endurance of significant levels of pain. In addition, paradoxically this type of intervention may also increase the risk of further falls and injuries principally because the individual achieves greater mobility as a consequence. Presently, scant evidence is available concerning the preferences of older people for an individualised multidisciplinary rehabilitation programme to promote recovery from a hip fracture.
Discrete Choice Experiment (DCE) is a stated preference technique originating in mathematical psychology which is designed to establish the relative importance and impact of individual attributes, or characteristics, upon the overall utility of a good or service (7). Within health economics there has been an exponential increase in the number of DCE studies undertaken within the last decade, with the majority focused upon the assessment of patient preferences within a wide variety of health care programmes and services (8, 9). However, DCE studies specifically designed for and conducted with older people (aged 65 years and over) remain rare in comparison with those conducted with general adult samples (8, 9). A recent commentary highlighted the potential for the application of discrete choice experiments in promoting patient choice for older people (8) and a recently published study in this jorurnal has demonstrated the potential for DCEs to engage older people in eliciting their views and preferences about alternative stroke specific rehabilitation services (10).
DCEs are typically administered through a questionnaire in which the respondent is presented with a series of choices between alternative health or rehabilitation programs and asked to choose the program that they would prefer. The alternative programs are described in terms of their attributes and associated levels (for example waiting time, location of treatment, type of treatment and staff providing the treatment). DCEs therefore provide information about the acceptability of different characteristics of programs, the trade-offs that patients are willing to make between these characteristics, and the relative importance of each of these characteristics in determining overall utility or value (11). This study sought to apply discrete choice experiment methodology to investigate the preferences of older people for rehabilitation to promote recovery from a hip fracture. Specifically, the DCE sought to investigate what older people would be prepared to endure in terms of levels of pain, physical effort and the risk of further falls and injury to recover the ability to mobilise independently following hip fracture through participation in an individualised multidisciplinary rehabilitation programme.
Methods
Questionnaire design
A DCE questionnaire was developed for completion via a face to face interview between the consenting participant and a trained interviewer. The questionnaire contained two main sections. Section A comprised a series of attitudinal statements relating to recovery following hip fracture, mobility, and quality of life. Respondents were asked to indicate the degree to which they agreed or disagreed with each statement on a 5 point Likert scale ranging from completely agree to completely disagree. Section B of the questionnaire contained the DCE questions. The scenarios presented for consideration in the DCE were based upon 4 salient attributes identified by the research team in consultation with rehabilitation clinicians based upon increasing levels of pain, effort, risk of further falls and mobility. The full factorial options resulted in 81 possible scenarios for presentation (=34). A fractional factorial design was employed to reduce this to a more practical total of 36 scenarios, generating 18 binary choice sets, which were 100% efficient for the estimation of main effects (7). This design was divided into 3 versions and 6 binary choice sets were presented within each version. Within each binary choice set, participants were asked to indicate their preferred choice between a pair of hypothetical scenarios reflecting the characteristics of an individualised multidisciplinary rehabilitation programme they would receive at two alternative locations. Given that patients were already currently participating in a rehabilitation program, a “forced choice” experiment was considered appropriate and no opt out option was provided.
Administration of questionnaire
Participants were recruited from Flinders Medical Centre, and the Repatriation General Hospital in Adelaide, South Australia. The study was approved by the Flinders Clinical Research Ethics Committee (approval no. 4609, approval granted february 2009). Patients were approached sequentially between May 2009 and November 2010 following referral to the research team by a key contact staff member at each hospital. Inclusion criteria were admission with a falls related proximal femur fracture, 60 years old and above, and not currently receiving palliative care. All patients who gave informed consent to participate took part in a face to face interview with one of two study researchers. The interviews were completed approximately 7 days following their surgery, either at the patient bedside or at their home.
Consenting family carer preferences were elicited by proxies directed to answer from the patient’s perspective in cases where significant cognitive impairment (defined in terms of a score less than 19/30 on the Mini-Mental State Examination (MMSE)) prevented an individual from giving informed consent and responding directly to the questionnaire. Whilst previous DCE studies in health care have tended to include participants with a reasonably high level of cognitive function (defined in terms of a MMSE score of 24 or above) for this study we attempted to be more inclusive in order to reflect more fully the views and preferences of older people themselves (including those from a residential care background), as opposed to obtaining proxy responses from a family member. There is evidence that the preferences of proxies often do not correspond well with the preferences of the patients themselves (12). The DCE was initially piloted with a small sample of patients (n = 10) with a range of levels of cognitive function to check respondents level of understanding of the questions and to indicate that they were providing meaningful responses. The findings from the pilot study indicated that patients with mild cognitive impairment (MMSE 19–23) were able to complete the questionnaire and were also able to provide meaningful responses. Minor changes to question layout and phraseology were made as a consequence of the findings of the pilot study to improve participant understanding.
Data analysis
The data from the DCE were analysed within a random utility theory framework using a conditional logit regression model (13). The function to be estimated was of the following form:
V = β75%risk_fall + β50%risk_fall + β25% risk_fall + βmild_pain + βmoderate_pain + βsevere_pain + β30_mins + βone_hour + βtwo_hours + βmobility-Independant + βmobility_frame + βmobility-wheelchair + e + u
V is the utility or satisfaction associated with the different rehabilitation programs.
βx are the estimated parameters of the model. e is the error term for the difference in observations. u is the error term for the differences between responses.
The estimated coefficients and their statistical significance (or otherwise) indicate the relevant importance of the different attributes on individual preferences. A positive sign on a coefficient indicates that as the level of the attribute increases so does the utility derived and the converse applies for a negative sign on a coefficient. The base levels of the coefficients could then be calculated using the formula that they were equal to the negative one multiplied by the sum of the coefficients for the two other levels. For every respondent, tests were also carried out to determine if any of the attributes were dominant (14). A dominant response implies that the scenario with the preferred direction of preference for one particular attribute is always chosen, irrespective of the levels of the remaining attributes presented. For example, a participant who always chooses the best level for mobility in every choice situation (irrespective of falls risk and the levels of pain or effort presented) has a dominant response pattern for mobility. Sub group analyses were undertaken by estimating two separate DCE models for [1] residential status: living in residential care versus living in the community, [2] education level: completed high school versus no qualifications, [3] age: 79 years and below versus 80 years and above, and the results were compared.
In order to estimate marginal rates of substitution (MRS), a conditional logit model was estimated including the risk of falling and the duration of effort required in the rehabilitation session as continuous variables. The MRS were then calculated by dividing the estimated coefficient for the attribute by the estimated coefficient for the selected value attribute (risk of falling or duration of effort).
Results
A total of 149 patients with a recently proximal femoral fracture were approached of whom 87 (58%) consented to participate in the study. The majority n = 61 (70%) of the participants were women and were between 71 and 80 years of age, n = 64 (74%). A small proportion were living in residential care prior to fracture [n =16 (18%)], the majority were living independently in the community prior to admission, n = 71 (82%). A total of 34 (39%) participants had a MMSE of 23 or below, of whom 10 (11%) had an MMSE of 19 or lower and therefore the questionnaire was completed on their behalf by a proxy family carer. For those participants with a MMSE of 23 and below, the results were found to be similar to those with a MMSE of 24 and above (results not shown), and therefore the results of these two groups were combined in a pooled analysis. Six (60%) of those participants whose questionnaire was completed by a proxy family carer were from residential care, the remainder were from the community.
The number of respondents who were dominant for each attribute and the total number of participants who were dominant for any attribute is presented in Fig. 1, along with the breakdown of dominant respondents for each attribute by sub group: living in residential care vs. the community prior to fracture in Fig. 2. Fig. 1 shows that 42 out of 81 (52%) participants who completed the this section of the questionnaire were dominant for the mobility attribute, this being much more common than dominance for any other attribute. Sub-group analysis revealed that the proportion of dominant respondents was largely similar for those living in residential care vs. the community prior to fracture.
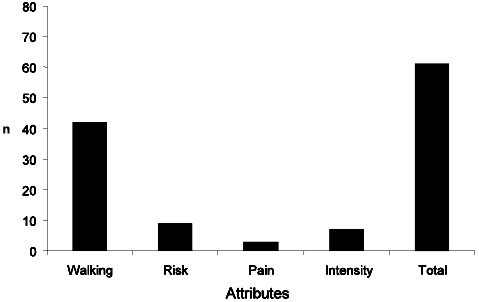
Fig. 1. The proportion of participants exhibiting dominant choice patterns from the total sample.
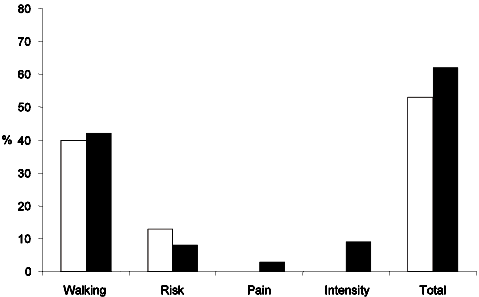
Fig. 2. The proportion of participants exhibiting dominant choice patterns within the residential care and community subgroups. Black columns represent the community subgroup and white columns represent the residential care subgroup.
Table I presents the results from the conditional logit model for the total sample. Both of the higher attribute levels relating to mobility (walking with a stick independently and walking with a frame) and the attribute level relating to the lowest risk of further falls (25%) were found to be highly important in determining positive preferences for an individualised multidisciplinary rehabilitation programme and were highly statistically significant (p < 0.001). Participants also exhibited negative preferences for the attribute levels relating to severely painful interventions and levels of effort involving rehabilitation intervention durations of two hours or more per day and both of these attribute levels were statistically significant.
|
Table I. Conditional logit model results (total sample). Data shown as coefficients with 95% confidence intervals (CI) |
|||
|
Attributes |
Attribute level |
Coefficient (95% CI) |
p |
|
FALLS: Your risk of falling and breaking another bone at some time point following rehabilitation |
50% or a 1 in 2 chance |
0.0354 (–0.1670 to 0.2378) |
0.732 |
|
25% or a 1 in 4 chance |
0.5450 (0.3316 to 0.7583) |
0.000 |
|
|
PAIN: The level of pain you would need to accept during rehabilitation with the aim of recovering your ability to walk short distances |
Moderate pain for 6 to 8 weeks |
0.2097 (–0.0004 to 0.4199) |
0.051 |
|
Severe pain for 6 to 8 weeks |
–0.4036 (–0.6111 to –0.1962) |
0.000 |
|
|
EFFORT: The level of effort you would need to make during rehabilitation by working hard and exercising with a physiotherapist |
1 h per day for 2 months |
0.0088 (–0.1985 to 0.2162) |
0.933 |
|
2 h per day for 2 months |
–0.4916 (–0.7020 to –0.2812) |
0.000 |
|
|
MOBILITY: Your ability to recover walking following participation in the programme |
Walking with a frame with 1 person close by |
0.4032 (0.2063 to 0.6001) |
0.000 |
|
Walking with a stick independently without help |
1.3807 (1.1697 to 1.5916) |
0.000 |
|
Table II presents the results from the conditional logit model for the subgroups according to place of residence prior to the hip fracture. It can be seen that both groups exhibited strong positive preferences for higher levels of the mobility attribute. However in contrast to those participants living in the community those living in residential care prior to hip fracture were less averse to severely painful interventions and levels of effort involving rehabilitation intervention durations of two hours or more per day. Both of these attribute levels were statistically significant in influencing the preferences of the community group but were uninfluential for the residential care group. The responses to the attitudinal questions for the total sample, and also for each subgroup can be found in Table III. The responses to the attitudinal statements broadly reinforce the findings from the DCE, indicating a strong preference to undertaking rehabilitation programmes with a view to increasing mobility, in both the residential and community care subgroups and the total sample.
Table IV presents the results of the conditional logit model for the sample with risk of falling and duration of effort for rehabilitation included as linear, continuous variables and the results of the marginal rates of substitution using risk of falling (risk) and duration of effort (duration) as value attributes. Plotting of the coefficient values attached to alternative levels of these two value attributes indicated that the assumption of a linear relationship was appropriate. The results indicate that, in general, participants would be prepared to accept a 22% increase in the risk of falling and breaking another bone to avoid enduring severe pain from participating in a rehabilitation programme. In general participants would also be prepared to accept an increase in the duration of the rehabilitation programme of over 2 h in a 2 month period (132 min) in order to achieve the highest mobility outcome of walking with a stick unaided.
|
Table II. Results of conditional logit model for subgroups based on living in the community or in residential care |
|||||
|
Attributes |
Attribute levels |
Residential care (n = 16) Coefficient (95% CI) |
p |
Community (n = 71) Coefficient (95% CI) |
p |
|
FALLS: Your risk of falling and breaking another bone at some time point following rehabilitation |
50% or a 1 in 2 chance |
–0.0684 (–0.5481 to 0.4113) |
0.780 |
0.0583 (–0.1672 to 0.2837) |
0.613 |
|
25% or a 1 in 4 chance |
0.7499 (0.2344 to 1.2653) |
0.004 |
0.4999 (0.2629 to 0.7369) |
0.000 |
|
|
PAIN: The level of pain you would need to accept during rehabilitation with the aim of recovering your ability to walk short distances |
Moderate pain for 6 to 8 weeks |
0.2129 (–0.2808 to 0.7066) |
0.398 |
0.2175 (–0.0168 to 0.4519) |
0.069 |
|
Severe pain for 6 to 8 weeks |
–0.1673 (–0.6592 to 0.3247) |
0.505 |
–0.4675 (–0.6991 to –0.2359) |
0.000 |
|
|
EFFORT: The level of effort you would need to make during rehabilitation by working hard and exercising with a physiotherapist |
1 h per day for 2 months |
–0.4692 (–0.9482 to 0.0096) |
0.055 |
0.1287 (–0.1036 to 0.3609) |
0.277 |
|
2 h per day for 2 months |
–0.1620 (–0.6513 to 0.3273) |
0.516 |
–0.5774 (–0.8138 to –0.3411) |
0.000 |
|
|
MOBILITY: Your ability to recover walking following participation in the programme |
Walking with a frame with 1 person close by |
0.8300 (0.3556 to 1.3045) |
0.001 |
0.3062 (0.0871 to 0.5253) |
0.006 |
|
Walking with a stick independently without help |
1.2330 (0.7463 to 1.7197) |
0.000 |
1.4322 (1.1949 to 1.6695) |
0.000 |
|
|
CI: confidence interval. |
|||||
|
Table III. Responses to attitudinal questions for total sample and by subgroup: living in residential care vs the community prior to fracture |
|||||||||||
|
|
A n (%) |
B n (%) |
C n (%) |
D n (%) |
E n (%) |
F n (%) |
G n (%) |
H n (%) |
|||
|
Total |
Strongly agree |
51 (58.6) |
32 (36.8) |
40 (46.0) |
0 (0) |
27 (31.0) |
3 (3.4) |
0 (0) |
9 (10.3) |
||
|
Agree |
31 (35.6) |
44 (50.6) |
38 (43.7) |
0 (0) |
55 (63.2) |
11 (12.6) |
5 (5.7) |
39 (44.8) |
|||
|
Neither agree nor disagree |
3 (3.4) |
7 (8.0) |
6 (6.9) |
0 (0) |
2 (2.3) |
5 (5.7) |
1 (1.1) |
20 (23.0) |
|||
|
Disagree |
1 (1.1) |
4 (4.6) |
3 (3.4) |
23 (26.4) |
2 (2.3) |
37 (42.5) |
24 (27.6) |
11 (12.6) |
|||
|
Strongly disagree |
1 (1.1) |
0 (0) |
0 (0) |
64 (73.6) |
0 (0) |
31 (35.6) |
57 (65.5) |
4 (4.6) |
|||
|
Did not answer |
0 (0) |
0 (0) |
0 (0) |
0 (0) |
1 (1.1) |
0 (0) |
0 (0) |
4 (4.6) |
|||
|
Residential care |
Strongly agree |
6 (37.5) |
3 (18.8) |
3 (18.8) |
0 (0) |
3 (18.8) |
0 (0) |
0 (0) |
3 (18.8) |
||
|
Agree |
7 (43.8) |
10 (62.5) |
8 (50.0) |
0 (0) |
11 (68.8) |
2 (12.5) |
0 (0) |
10 (62.5) |
|||
|
Neither agree nor disagree |
1 (6.3) |
2 (12.5) |
3 (18.8) |
0 (0) |
1 (6.3) |
2 (12.5) |
0 (0) |
1 (6.3) |
|||
|
Disagree |
1 (6.3) |
1 (6.3) |
2 (12.5) |
7 (43.7) |
1 (6.3) |
5 (31.3) |
6 (37.5) |
2 (12.5) |
|||
|
Strongly disagree |
1 (6.3) |
0 (0) |
0 (0) |
9 (56.3) |
0 (0) |
7 (43.8) |
10 (62.5) |
0 (0) |
|||
|
Community based |
Strongly agree |
45 (63.4) |
29 (40.8) |
37 (52.1) |
0 (0) |
24 (33.8) |
3 (4.2) |
5 (7.0) |
6 (8.5) |
||
|
Agree |
24 (33.8) |
34 (47.9) |
30 (42.3) |
0 (0) |
44 (62.0) |
9 (12.7) |
0 (0) |
29 (40.8) |
|||
|
Neither agree nor disagree |
2 (2.8) |
5 (7.0) |
3 (4.2) |
0 (0) |
1 (1.4) |
3 (4.2) |
1 (1.4) |
19 (26.8) |
|||
|
Disagree |
0 (0) |
3 (4.2) |
1 (1.4) |
16 (22.5) |
1 (1.4) |
32 (45.1) |
18 (25.4) |
9 (12.7) |
|||
|
Strongly disagree |
0 (0) |
0 (0) |
0 (0) |
554 (77.5) |
0 (0) |
24 (33.8) |
47 (66.2) |
4 (5.6) |
|||
|
Missing |
|
|
|
|
1 (1.4) |
|
|
4 (5.6) |
|||
|
A: I am confident that I will be able to walk again eventually; B: I want to be able to walk again even if there is a high risk that I could fall again and break another bone in the future; C: I am prepared to make a large physical effort over a period of several weeks to enable me to walk again; D: I would prefer to go into a wheelchair now and forget about walking again; E: I am prepared to accept pain for a number of weeks whilst following an exercise programme if it will enable me to walk again; F: I am very tired and I don’t want to have physiotherapy to help me with walking; G: I would be happy to use a mechanical lifter to move me from the bed to a chair for the rest of my life; H: I would be prepared to pay a fee to receive an 8-week rehabilitation programme in the nursing home to help me walk again. |
|||||||||||
|
Table IV. Marginal rates of substitution using risk of falls and duration of effort as value attributes |
||||
|
Attribute |
Level |
Coefficient (SE) |
MRS risk, % |
MRS duration of effort, min |
|
FALLS |
Risk |
–0.0160*** (0.0057) |
– |
2.000 |
|
PAIN |
Mild |
0.138 |
–8.625 |
–0.005 |
|
|
Moderate |
0.209** (0.104) |
–13.063 |
–26.125 |
|
|
Severe |
–0.347*** (0.010) |
21.688 |
43.375 |
|
EFFORT |
Duration |
–0.0078*** (0.0020) |
0.500 |
– |
|
MOBILITY |
Wheelchair bound |
–1.361 |
85.063 |
170.125 |
|
|
Walking with a frame |
0.304*** (0.091) |
–19.000 |
–38.000 |
|
|
Walking with a stick |
1.057*** (0.105) |
–66.063 |
–132.125 |
|
*p < 0.1, **p < 0.05, ***p < 0.01. SE: standard error; MRS: marginal rates of substitution. |
||||
The results of the conditional logit model were also analysed split for subgroups based on education level (no qualification vs high school completion and above) and age (79 years and below vs 80 years and above). There were no significant differences between the results split according to subgroup and the main results (data not shown).
Discussion
To our knowledge this is the first time DCE methodology has been applied to ascertain patient preferences for an individualised multidisciplinary rehabilitation programme following hip fracture. The findings from this DCE study indicate that mobility outcomes and the achievement of independent mobility have significant and positive impacts for frail older people recovering from hip fracture. This study also provides important preliminary evidence for the feasibility and future potential for DCE methodology to be applied to elicit the treatment preferences of frail older people, a sub-group of the population traditionally excluded from studies of this nature (9).
Although our sub-sample of participants from residential care was small (n =16), we found that the preferences of participants from a residential care background were broadly similar to those from a community background. Participants from both residential care and the community exhibited strongly positive preferences for improved mobility following hip fracture and these differences were found to be statistically significant. This finding is reinforced by the responses to the attitudinal questions whereby all participants from both residential care and the community (100%) expressed they disagreed or strongly disagreed with the statement ‘I would prefer to go into a wheelchair now and forget about walking’. Presently in Australia, patients from high care residential aged care facilities (nursing homes) are denied the same opportunities in relation to rehabilitation care as compared to people from community or low care residential aged care settings, an approach which is increasingly being questioned (15). Recently updated hip fracture guidelines from the National Institute of Health and Clinical Excellence (NICE) in the UK have recommended that priority research be undertaken into the provision of rehabilitation strategies for rehabilitating residential care patients following a hip fracture through their care facilities (16). A recent systematic review and an editorial have also highlighted the likely clinical benefit to this group (17). The findings from this study concur with these recommendations.
The DCE study represents a snapshot study of patient preferences at one time point only, following surgery for hip fracture. It may be the case that patients could change their preferences for rehabilitation over time, for example, if optimal rehabilitation is not achieved, or if their health declines further. We elected to survey patients about their preferences for rehabilitation early after their surgery when they were first commencing rehabilitation as it has been demonstrated that it is at this time-point that their engagement with a rehabilitation program is most important as rehabilitation must commence early following surgery to achieve the best outcomes (16). The chosen attributes and levels were developed with health professionals engaged in the provision of rehabilitation programmes and piloted with patients receiving rehabilitation for relevance, language and coverage. However, it is important that future research includes a comprehensive and client-focused method of defining attributes and levels for DCEs. The selection criteria recently presented by Coast et al. (18) recommending more methodologically rigorous methods of attribute selection based on qualitative methods would be useful in this regard.
This study provides important preliminary evidence relating to the preferences of frail older people for improved mobility as a consequence of an individualised multidisciplinary rehabilitation intervention following hip fracture. The findings indicate that, in general, the desire to recover mobility through a rehabilitation intervention is tempered by an aversion to high levels of risk of further falls and pain. This finding is important to note, given the current NICE recommendations to investigate the effectiveness of higher intensity rehabilitation programs, which may result in increased pain and fatigue for patients (16). If these guidelines were implemented in Australia, our study provides evidence that frail older adults are willing to participate in programmes requiring increasing effort and resulting in increasing pain during rehabilitation. However, a significant proportion is averse to programmes of severe pain and very long duration. Therefore, while higher intensity rehabilitation programmes are likely to be acceptable to this group, especially if they provide the chance of improved mobility outcomes for participants, it would be important for those designing such programmes to consider process outcomes such as the level of effort involved. It will be important in the future for both researchers and clinicians to determine novel strategies to design rehabilitation programmes which provide the intensity required to gain the mobility outcomes that older people so highly value but within levels of effort and pain which are acceptable. Physical exercise programmes are not only of interest for hip fracture rehabilitation, but are also of interest in older adults as a way of reducing the functional decline associated with hospitalisation (19) and in older community dwelling adults to reduce functional decline to maintain health and independence (20). Particularly Liu & Latham (20) in their Cochrane review of the effects of resistance strength training on physical function in older adults found effects on strength and vitality with higher intensity interventions, although the number of published studies was small. It would be interesting to consider whether the findings we have reported in hip fracture patients would also apply to other groups of older adults. While this may be the case, the preferences of older adults in other groups receiving rehabilitation programs needs further examination.
The study also adds to the bourgeoning literature highlighting the potential for the wider application of DCE methodology as a valuable tool for engaging with, and eliciting the views and preferences of, frail older people in relation to their health and health care (8, 10, 21), a group traditionally excluded from studies of this nature (8, 9). We attempted to be inclusive with the DCE by not excluding older adults with mild cognitive impairment. The preferences of those with mild cognitive impairment are particularly important given the increasing awareness that those with cognitive difficulties should not be excluded from rehabilitation programmes (16). The preliminary finding from our study are generally positive and indicate the potential for DCE’s to be conducted in samples of older people with mild cognitive impairment. However it is important that further work is conducted to assess the practicality and feasibility of this approach in older people with cognitive impairment. The application of qualitative research methods, including think aloud approaches (22), may be particularly helpful in this regard to investigate the process of DCE decision making in this group. Further research should also be directed towards achieving greater equity in access to rehabilitation services for the wide spectrum of patients attending hospital with hip fractures.
Acknowledgements
This study was supported financially by contributions an Australian NHMRC Health Services Research Strategic Award Grant 402791 entitled ‘Transition Care: Innovation and Evidence’. We are grateful to Dr Leonie Burgess for assistance with the DCE study design and Associate Professor Emily Lancsar for her helpful comments on a previous version of this paper.
References

