Electrodiagnostic studies are the gold-standard evaluation tools for peripheral nerve entrapment syndromes. However, although they can indirectly localize the site of injury (through physiological data), they cannot provide morphological confirmation as do other imaging methods (1). Furthermore, during lower limb diagnostics in particular, electrophysiologists may encounter various challenges concerning certain entrapment syndromes, e.g. meralgia paraesthetica, tarsal tunnel syndrome, Morton’s neuroma. In addition, technical difficulties during sensory evaluations with surface electrodes (even with near-nerve needle techniques) may overwhelm the diagnostics (2–5). In this case, ultrasound appears to be a very convenient, real-time imaging tool, whereby it is practical for the physician to scan several peripheral nerves immediately after medical/physical examination of the patient. In addition, in the aforementioned challenging cases, it becomes a powerful diagnostic tool rather than merely an adjunct to electrodiagnostics. With ultrasound, one can morphologically confirm entrapment, uncover the underlying cause of injury, precisely guide onward intervention (injection/surgery), and follow up the injury (1).
Thus, having organized study of the upper limb in 2012 (6), in a similar workshop in 2013 we studied the lower limb nerves in parallel sessions using cadavers and ultrasound (Fig. 1).
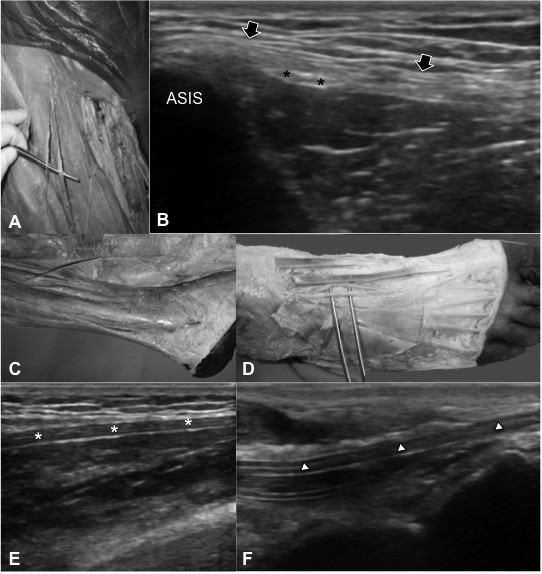
Fig. 1. Anatomical dissections and their corresponding ultrasound images for (A, B) lateral femoral cutaneous, (C, E) superficial and (D, F) deep peroneal nerves. (A) Lateral femoral cutaneous nerve is shown distal to its bifurcation in the inguinal region lateral to the femoral nerve and vessels. (B) On ultrasound imaging (axial view), the nerve is visualized as two fascicles (black asterisks) next to the anterior superior iliac spine (ASIS) at the level of the inguinal ligament (black arrows) before its bifurcation. (C) Superficial peroneal nerve is shown to become more superficial distally innervating the (reflected) skin. (D) The distal end of the deep peroneal nerve is shown on the dorsum of foot. (E) On ultrasound imaging (longitudinal view), the nerve (white asterisks) is visualized as a hypoechoic tubular structure. (F) On ultrasound imaging (longitudinal view), the nerve (white arrowheads) is visualized as a tubular structure within the muscles (on the left side) and very superficial distally (on the right side).
This time we included in-depth electrophysiological discussion regarding the above-mentioned entrapment syndromes, and tried to determine how diagnostic challenges can be overcome.
In addition to entrapment syndromes, the other important issue is that of nerve blocks. In rehabilitation settings, such interventions are performed for neuralgia, muscle spasticity, diagnosis/treatment of painful joint conditions, and surgery. Due to the anatomical variability of the nerves, such procedures are technically difficult and their success rates using anatomical landmarks are suboptimal (7). Guidance using high-dose radiation (computed tomography, fluoroscopy) does not fall within the scope of this paper; however, our answer to the question as regards the comparison of ultrasound vs stimulator-guided nerve blocks would be “seeing is believing”. It is possible to decrease both the amount of local anesthetic and the onset of the anesthetic block (time interval between application and block occurence) and it is possible to avoid intravascular injections (7–9).
Overall, ultrasound is a practical and cost-effective imaging method for the management of peripheral nerve pathologies. We believe that it is the superiority of physiatrists to have the opportunity to perform ultrasound together with electromyography and this will lead to the best diagnoses in these patients.
REFERENCES
Accepted Apr 23, 2013; Epub ahead of print May 16, 2013
Levent Özçakar, MD1, Murat Kara, MD2, Bülent Yalçın, MD3, Elif Yalçın, MD2, Tülay Tiftik, MD2, Sedat Develi, MD3 and Fatih Yazar, MD3
From the 1Hacettepe University Medical School, Department of Physical and Rehabilitation Medicine, 2Ankara Physical and Rehabilitation Medicine Training and Research Hospital and 3Gülhane Military Medical Academy, Faculty of Medicine, Department of Anatomy, Ankara, Turkey. E-mail: lozcakar@yahoo.com

