Thorsten Meyer, PhD1, Christoph Gutenbrunner, MD2, Carlotte Kiekens, MD3,
Dimitrios Skempes, MPH4,5, John L. Melvin, MD6, Kuno Schedler, DSc (Econ)7,
Marta Imamura, MD, PhD8 and Gerold Stucki, MD4,5
From the 1Institute for Epidemiology, Social Medicine, and Health Systems Research, 2Department for Rehabilitation Medicine, Hannover Medical School, Germany, 3Physical and Rehabilitation Medicine, University Hospitals Leuven, Leuven, Belgium, 4Swiss Paraplegic Research (SPF), Nottwil, 5Department of Health Sciences and Health Policy,
University of Lucerne, Lucerne, Switzerland, 6Department of Rehabilitation Medicine, Jefferson Medical College, Thomas Jefferson University, Philadelphia, USA, 7Institute for Systemic Management and Public Governance of the University of St Gallen, St Gallen, Switzerland and 8Department of Orthopaedics and Traumatology, University of Sao Paulo School of Medicine, Sao Paulo, Brazil
There is a need for a comprehensive classification system of health-related rehabilitation services. For conceptual clarity our aim is to provide a health-related conceptual description of the term “rehabilitation service”. First, we introduce a common understanding of the term “rehabilitation”, based on the current definition in the World Health Organization’s World Report on Disability, and a conceptual description of rehabilitation agreed upon by international Physical and Rehabilitation Medicine organizations. From a health perspective, rehabilitation can be regarded as a general health strategy with the aim of enabling persons with health conditions experiencing or likely to experience disability to achieve and maintain optimal functioning. Secondly, we distinguish different meanings of the term “service”, that have originated in management literature. It is important to distinguish between micro, meso and macro level uses of the term “service”. On a meso level, which is central for the classification of rehabilitation services, 2 aspects of a service, i.e. an offer of an intangible product and an organizational setting in which the offer is upheld, are both essential. The results of this conceptual analysis are used to develop a conceptual description of health-related rehabilitation, which is set out at the end of this paper. This conceptual description may provide the basis of a classification of health-related rehabilitation services, and is open for comments and discussion.
Key words: rehabilitation; health services; organization; classification; conceptual analysis.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Thorsten Meyer, Institute for Epidemiology, Social Medicine, and Health Systems Research, Hannover Medical School, 30625 Hannover, Germany.
E-mail: meyer.thorsten@mh-hannover.de
Accepted Sep 3, 2013; Epub ahead of print Nov 21, 2013
Introduction
Health systems development became a major focus of the work of the World Health Organization (WHO) under the aegis of its director general Dr Gro Harlem Brundtland, with the publication of the World Health Report in 2000 (1). This development was later taken up by other major political players for global health, such as the World Health Assembly and the World Bank, giving the issue of “strengthening health systems” a high political priority (2, 3). A health systems framework, consisting of 6 building blocks, including leadership and governance, service delivery, human resources, essential medical products and technologies, health information systems and health financing, was developed by the WHO in order to understand health systems, target development gaps and monitor change (2, 4). A strong commitment to the importance of good health system data, which should guide health policy decisions, is at the heart of this development.
Rehabilitation, as a key health strategy to address disability (5, 6), is essential to a health system addressing the needs of its population. The seminal publication of the World Report on Disability by the WHO and the World Bank (7) emphasized the potential rehabilitation has to tackle disability-related health issues. However, a lack of data on disability became apparent, including data on rehabilitation services and their role within the health system. Lack of (access to) available rehabilitation services has been pinpointed as a major barrier to rehabilitation, especially in low-income countries or rural areas. Data on rehabilitation are often not disaggregated from data on other healthcare services, and administrative data on the provision of services is often fragmented due to the fact that rehabilitation may take place in a variety of settings and be performed by different professions. There is no common framework for the evaluation of these rehabilitation services.
There are international classification systems that provide a common language to describe aspects of health and healthcare. They enable the comparison of health-related data within populations over time and between populations at the same point in time, as well as the compilation of internationally consistent data (8). However, the reference classifications of the WHO, the International Classification Diseases (ICD), the International Classification of Functioning, Disability and Health (ICF), as well as the upcoming International Classification of Health Interventions (ICHI), all relate to the personal level, i.e. to the micro level of patient care. A comprehensive description of healthcare for persons with disabilities should also include the context, i.e. setting, in which an intervention takes place. We refer to this as the meso level of healthcare. To date, we are missing this important piece of meso level information: what types of services are offered in relation to which patients’ needs? A sound comparative description of service provision and analysis of service gaps is hampered without sound information on rehabilitation services. A classification system for rehabilitation services could be used as a common framework to describe rehabilitation services within a defined region or country. It would offer the opportunity for inter-regional or international comparisons, and should provide the information needed for better planning, organization and monitoring of rehabilitation care as well as prioritizing rehabilitation services in national and global health policy agendas. Therefore, there is a need to develop a respective classification system.
The International Society for Physical and Rehabilitation Medicine (ISPRM), as the international umbrella organization of physical and rehabilitation medicine, has identified the development of a rehabilitation service classification system as one of its policy agenda items (9). Following the procedures of ISPRM, ISPRM leadership had mandated the WHO/ISPRM-Liaison-Committee, and specifically its Medical Rehabilitation Sub-Committee to develop a series of discussion papers, of which the present paper is the first.
The starting point of such a classification should be a clear understanding of the basic underlying concepts. Therefore, we aim to provide a conceptual description of the term “rehabilitation service”. First, we will discuss our understanding of the terms “rehabilitation” and “service”. Then we will bring both lines of thought together, and propose a conceptual description of health-related1 rehabilitation services.
What is rehabilitation?
Rehabilitation in the area of health is a complex concept. It has no single or common location, such as a hospital, for secondary or tertiary curative care, nor is it performed by a circumscribed profession defined by an organ system, such as ophthalmology or cardiology. Therefore, a definition of rehabilitation requires other starting points. Rehabilitation is best described by its aim, to re-habilitate, i.e. to restore or return a person to a state of optimal functioning in interaction with his or her environment. Hence, rehabilitation relates to the individual level. Interventions on the societal level, e.g. barrier removal initiatives, are not considered rehabilitation (7, p. 96).

1The UN Convention on the Rights of Persons with Disabilities (United Nations General Assembly, 2006) distinguishes health-related rehabilitation (§25) and rehabilitation as a general term (§26) that can be related besides health to areas of employment, education and social services. While, in practice, it is not easy to draw a clear-cut line between these areas, in the present paper we apply a health-related rehabilitation perspective.
Rehabilitation has been defined as an idea, or “concept” (10, p. 3). It has been conceptually specified as 1 of 4 health strategies (11).2 Essentially, rehabilitation might be best characterized as a general health strategy that is specific in its aim of optimizing human functioning. For example, the World Report on Disability defines rehabilitation as “a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments” (7, p. 96). Accordingly, a recently developed conceptual description of rehabilitation based on the model of the ICF (12) is constituted by the goal “to enable persons with health conditions experiencing or likely to experience disability to achieve and maintain optimal functioning” (6, p. 282). This conceptual description of rehabilitation has been endorsed by various international professional societies in the field of physical and rehabilitation medicine3.
It is worth considering whether we could define rehabilitation services by viewing rehabilitation first and foremost as a health strategy characterized by a specific aim. It could be argued that almost everything we do in healthcare is, to some degree, related to improvement of functioning. For example, an operation on the cardiac valve is not made just because of an organ defect, but to restore adequate levels of functioning in a person, e.g. the ability to do a physical job. In many cases, problems with functioning might be the initial reason for patients to contact healthcare (primary or community care), or resolving these may be regarded as the ultimate goal of medical care.
There is no specific location or single profession related to rehabilitation in these definitions (7).4 Rehabilitation needs may be present along the continuum of care, from the acute or initial phase immediately following recognition of a health condition, through to post-acute and maintenance phases, and involves hospitals, rehabilitation facilities and community institutions (6, 7, 13).
While, in 1981, WHO described the target group of rehabilitation as “the disabled and handicapped” (15, p. 9), the current approaches converge to target individuals who experience, or who are likely to experience, disability in interaction with their environments (7). Differences arise as to whether the presence of a health condition should be a specifying characteristic (6). All descriptions convey the notion of optimizing functioning as the ultimate aim of rehabilitation. An explicit reference to health-related aspects of rehabilitation is in line with the understanding of rehabilitation as 1 of 4 health strategies (5). According to the ICF a health condition is not related only to acute or chronic diseases, but is an umbrella term also encompassing disorders, injuries or trauma (12).

2These 4 health or healthcare strategies include prevention, curation, rehabilitation and support.
3Section of Physical and Rehabilitation Medicine of the Union Européenne des Médecins Spécialistes (UEMS-PRM section), European Society of Physical and Rehabilitation Medicine (ESPRM), European Academy of Rehabilitation Medicine (EARM), ISPRM.
4 It should be noted that specialties of various professions have evolved that are specific to the field of rehabilitation (6), e.g. physicians specializing in physical and rehabilitation medicine (14) or rehabilitation psychologists, in the USA and Germany.
In the United Nations Convention on the Rights of Persons with Disabilities (16), the most rapidly negotiated human rights treaty of the 21st century, rehabilitation is again understood and characterized by its aim, i.e. “to enable persons with disabilities to attain and maintain maximum independence, full physical, mental, social and vocational ability, and full inclusion and participation in all aspects of life” (article 26, § 1). It should start as early as possible, be multidisciplinary and based on individual needs and strengths, be voluntary, and access to services should be in close proximity to a person’s place of residence in the community.
To sum up, from a health perspective, rehabilitation can be thought of as a general health strategy with the aim of enabling persons with health conditions experiencing, or likely to experience, disability to achieve and maintain optimal functioning. This definition allows the inclusion of consideration of very different settings or professions who deal with rehabilitation issues, such as geriatrics, social psychiatry, or a physical therapy office.
What is a service?
All healthcare systems provide health services. However, within the health sector there is a lack of conceptual clarity on the meaning of the term “service”, despite its widespread use.
From an etymological perspective the term “service” comes from the act of serving, as has been attested from the early 13th century. From the 16th century onwards the term related to the “duty of a military man”. This use of the term has carried into the present. The use of the term in relation to the service industry (as distinct from production) is attested from 1941.5 The term “service” has been widely used in management theory, specifically in the sub-discipline of marketing and production (17). Contrary to tangible products, i.e. goods, services are intangible products, e.g. accounting, consultancy, education, transportation. No transfer of possession or ownership takes place when services are sold. They cannot be stored or transported, are instantly perishable, and come into existence at the time they are bought and consumed. Services are supplied in themselves (“service industry”), but they might also be closely associated with goods. For example, when buying a car, a customer may rely on a wide set of additional services that are linked to this car and which increase the overall customer value of this transaction (18). In a medical context, establishing a diagnosis is a service that might go along with the delivery of a good, e.g. a medication, or the delivery of a further service, e.g. a therapy or any type of intervention.

5Definition from online etymology dictionary, www.etymonline.com.
While this definition implies that all medical services are in direct contact with a person in need or in demand of a service, there are also non-personal services important for the health sector, e.g. so-called ancillary services (19), such as laboratory services.
In the context of governmental services it has been highlighted that public services often do not address a conventional customer who buys a readymade product. Rather, public services are often co-produced by so-called pro-sumers (a combination of a producer and a consumer of the service) (20). The peculiar situation of a service provider in this case is that the success of his efforts depends on the cooperation of the client. This is true for the teacher–student relationship, for the relationship between social worker and client, but also for the relationship between therapist and patient in rehabilitation.
From a general healthcare perspective, it should be noted that the term “service” has wide uses and may refer to very different levels of care. It relates to the micro level of care where the delivery of interventions is focused. It relates to a meso level of healthcare in 2 ways. Services characterize what a health institution offers in principle in terms of intangible products to patients with certain health-related characteristics. Also, the organizational units of healthcare, i.e. facilities or delivery points of services, are sometimes called services6 (21). While, in principle, the first meso level description of a service can be thought of without the second, e.g. telephone counselling, the second meso level description of a service only makes sense in combination with the first meso level description of a service. It might be thought of as the setting necessary to provide services. Lastly, it has also been used on a macro or policy level, exemplified in the term “military services” or even “health services”, as in health services research (Fig. 1). Therefore, it is necessary to specify our use of the term, accordingly.
Fig. 1. Different levels of services in health care.
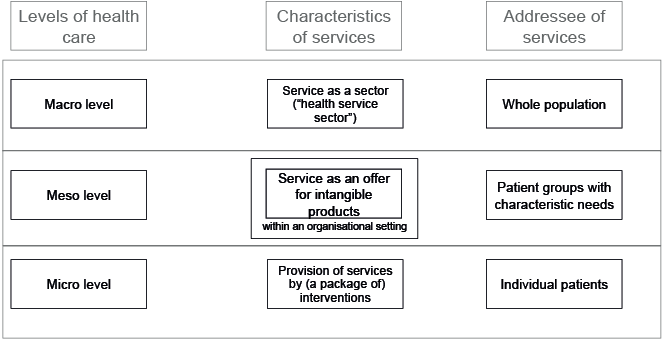
Health service provision takes place in a particular organizational setting and leads to the delivery of (a series of) health interventions. It appears that health services, due to their prominent role in healthcare, are the main product, while goods, if present at all, are part of a service or intervention. Healthcare interventions are part of a service7. Interventions relate to personal services, not to non-personal services.

6In both German and Dutch we distinguish between a “Dienstleistung” (German) or “dienstverlening” (Dutch) and a “Dienst”, which can also refer to the setting in which a service is provided.
7In fact, the definition of a health intervention within the development of the ICHI uses the term “service” in this restricted sense: [A health intervention is a] “service performed for or on behalf of a client(s) whose purpose is to improve health, to alter or diagnose the course of a health condition or functioning, or to promote wellness”. (Unpublished paper, ICHI development project plan, version 2.1, July 2010, p. 8).
For the sake of a classification of rehabilitation service, it should be stated that we are not interested on the micro level perspective on services, i.e. the actual provision of services on an individual level. Here, a classification system (ICHI) is already under development (8). We are also not interested in the macro level distinguishing different policy domains. A classification of rehabilitation services should relate to the meso level of healthcare, i.e. a description of offers of personal or non-personal intangible products for persons with specified health-related needs. These products are inherently related to the setting in which they are offered and delivered. In addition, it might be useful to identify rehabilitation services by identifying the setting in which rehabilitation is offered and delivered (e.g. clinics, hospital units, rehabilitation facilities, organizations).
For example, a rehabilitation clinic can represent a rehabilitation service on an organizational level, i.e. a rehabilitation facility. It may offer and deliver different rehabilitation services, e.g. for persons with chronic back pain and amputees, providing both rehabilitation interventions and non-personal products, including goods such as prosthetics.
Health services, as defined on this meso level, can be further characterized by their degree of professionalism. People offering a service should have a minimum degree of special education in health issues, i.e. professionalism might be thought of as a prerequisite for a health service.
To sum up, services within the healthcare field are personal and non-personal intangible products offered to improve health, to alter or diagnose the course of a health condition or functioning, or to promote wellness, by delivering interventions within an organizational setting by health professionals and, under certain conditions, appropriately trained community-based workers.
What is a rehabilitation service?
Table I depicts our proposal for a conceptual description of rehabilitation services. It is fair to assume that, in healthcare, most products delivered are intangible (i.e. they are services), and that the delivery of tangible products (i.e. goods) is usually integrated into a service (line 2 of Table I).
|
Table I. A conceptual description of health-related rehabilitation services |
|||
|
Line |
|||
|
1 |
Rehabilitation services, |
||
|
2 |
are personal and non-personal intangible products |
||
|
3 |
offered to persons with a health condition experiencing or likely to experience disability or to their informal care-givers |
||
|
4 |
within an organisational setting |
||
|
5 |
in interaction between provider and person |
||
|
6 |
addressing individual functioning needs |
||
|
7 |
that aim at enabling persons to achieve and maintain optimal functioning |
||
|
8 |
considering the integration of other services addressing the individual‘s needs |
||
|
9 |
including health, social, labour and educational services |
||
|
10 |
and delivered by rehabilitation professionals, other health professionals, or appropriately trained community-based workers. |
||
Services might be thought of as a potential or an offer that is held available for provision, as indicated in line 3 of Table I. Here, as in line 5, we prefer to use the term “person”, rather than “patient”, to describe the addressee of the service. This is in line with the UN Convention on the Rights of Persons with Disabilities. This person is characterized in line 3, referring both to the broad ICF term “health condition” as introduced above, to relate this conceptual description to the area of health, and to the disabling experience of the person, as in the definition of the World Report on Disability or by the conceptual description of rehabilitation provided by Meyer et al. (6). Also, we have included family or informal care-givers of a person with a health condition as possible addressees of a rehabilitation service.
A service is always offered within a special organizational setting (line 4), that is inherently related to the service itself. These characteristics should be strongly related the quality of the service. Therefore, in practice, services can hardly be viewed independently of their respective organizational setting. These settings could be part of a rehabilitation classification system themselves, or serve as the point of departure to identify rehabilitation services.
Line 5 illustrates the pro-sumer role of the person that characterizes an interaction between partners, i.e. professional and person.
Line 6 points to the fact that any health service should address individuals’ needs, and rehabilitation services should react to functioning needs in terms of the ICF. These services related to functioning needs could comprise the performance, application or integration of biomedical and technological interventions, psychological and behavioural, educational and counselling, occupational and vocational, social and supportive, and physical environmental interventions, as has been exemplified in a conceptual description of physical and rehabilitation medicine (22).
Line 7 is taken from the conceptual description of rehabilitation (6) and pinpoints the central aim of rehabilitation as its defining core element. Services should be identified as rehabilitation services if their primary goal is related to enabling persons to achieve and maintain optimal functioning (line 7). For example, a classification of rehabilitation services in terms of rehabilitation settings would need to specify the organizational units providing the services. It can be a community rehabilitation centre, a department of a community centre, a rehabilitation clinic, or a department within a hospital. As can be seen, the size and scope of the different organizational settings can vary to a large extent. Also, the primary goal of the respective organizational setting has to be determined. If the core interest and the competencies of the professionals of the organizational setting are to enable persons experiencing or likely to experience disability to achieve and maintain optimal functioning, the service provided by the organizational setting should be called a rehabilitation service. For example, this could be an early rehabilitation unit in a hospital. If the organizational unit is a surgical unit that performs interventions aiming at the enhancement or prevention of deterioration of body structures or function, this should not be called a rehabilitation setting.
It is interesting to note that the System of Health Accounts (SHA) of the Organisation of Economic Cooperation and Development (OECD), in trying to identify rehabilitation care, came to a comparable solution (19). Here the term “focus” is used, comparable to what we have called “core interest”. The SHA document states that “Whereas curative services focus primarily on the health condition, rehabilitation services focus on the functioning associated with the health condition.” (p. 87). In distinguishing rehabilitation from other health functions, the SHA claims that “only rehabilitative components with a primary purpose related to health functioning” should count within the category of rehabilitation. In the SHA, too, rehabilitation is thought to take place over the course of the health condition, along a continuum of care and across sectors from health, education and labour to social affairs (19).
There is a special characteristic of rehabilitation services that should be kept in mind. In rehabilitation, individuals with chronic care conditions are often characterized by multiple and/or complex needs. Therefore, rehabilitation service provision has to face the complexity of these needs, which require the integration and management efforts between service providers for integrated medical and social support service (line 8). Individuals with chronic needs must access a number of diverse systems of care and services, including the areas of health, education, labour, and social affairs (line 9). These diverse systems of care and services need to be integrated in order to meet the needs of the person (23, 24). Individuals with chronic care conditions are often unable to navigate a non-integrated service system on their own. Therefore, organizations need to form inter-organizational ties with one another within integrated systems (25, 26), often arranged through intermediaries which have in-depth knowledge of a system of health services in a specific field or region (27). The World Report on Disability points out that, to ensure the continuity of care, coordination should be present when more than 1 service provider is involved in rehabilitation, (7).
In providing specific rehabilitation services, it is essential that the professionals involved possess appropriate qualifications (7) (line 10). These professionals can be rehabilitation personnel, health personnel, or community-based workers, who usually address a wide range of individual problems.8 It should be noted that professional expertise specific to rehabilitation is a prerequisite for a professional rehabilitation service. This does not preclude that individuals with disabilities (peer counsellors) or family members can be taught to provide functioning interventions themselves. The availability of the different needed professions is often an issue in low-income countries (7).

8The issues of different fields of expertise in different rehabilitation professions, and of training of rehabilitation professionals are closely related to national laws and local customs, and are beyond the scope of this paper.
Discussion
The UN Convention on the Rights of Persons with Disabilities calls on state parties to organize, strengthen and extend comprehensive habilitation and rehabilitation services and programmes, particularly in the areas of health, employment, education and social services (Art. 26). The World Report on Disability pinpointed the need for appropriate data and more accurate statistics, which is also the prerequisite of the health systems strengthening initiatives initiated by WHO. Service delivery is 1 of the 6 building blocks of health systems that need to be strengthened, particularly in developing countries. However, there is a lack of consensus on what constitutes a health service. For the area of health-related rehabilitation, we have presented and argued for a proposal of a conceptual description of rehabilitation services. This is based on a thorough discussion of the ideas of rehabilitation and services. It might be possible and useful to extend our approach to other areas of health, or to other areas of rehabilitation, such as labour, education or social affairs. However, this discussion is beyond the scope of the present paper. This conceptual description aims to be comprehensive and descriptive, without making statements about what should be regarded as a good or bad service. Other approaches are needed to follow that thread; for example, related to the health systems building blocks approach, which has included some quality indicators for monitoring health systems.
We have tried to emphasize that a rehabilitation services classification system should not be about classifying rehabilitation interventions. Health interventions are currently in the process of being classified in the ICHI of the WHO. Rather, we are aiming at distinguishing different rehabilitation “packages” of interventions and further non-personal products, addressing functioning needs, and offered within different types of organizational settings that are related by a common goal, to enhance functioning in persons with a health condition experiencing, or likely to experience, disability.
Rehabilitation services are special services within the realm of healthcare. They are intangible; however, the provision of goods can be part of a service. They can be very complex, e.g. part of the care for a person with a spinal cord injury in a specialized spinal cord injury centre. Or they can be quite simple, e.g. exercise training for cardiovascular patients in a sports club supervised by a physical therapist as part of a rehabilitation plan.
One challenge of the results of this paper lies in the fact that we cannot just classify services that call themselves rehabilitation services, as that could be too restrictive.9 We might miss services that, to all intents and purposes, are rehabilitative. And we might include services that might call themselves rehabilitative, but should be run under a different label. Therefore, the challenge is to identify and characterize appropriate organizational settings and to pinpoint the main goals of their services. In doing so, we might cope with the problem that rehabilitation services are inherently dependent on the health system they are part of. An approach that is able to integrate the peculiarities of the individual health systems is a prerequisite for the development of a common classification of rehabilitation services.
However, classifying rehabilitation services involves more than just classifying rehabilitation institutions. An institution can offer different rehabilitation services, e.g. an early rehabilitation unit might offer services for stroke patients, for patients before and after elective surgery, and for geriatric patients.
In order to open debate, the WHO/ISPRM-Liaison-Committee is publishing its work as discussion papers in the official journal of ISPRM. We are working towards the goal of developing a framework for a classification system of rehabilitation services. Obviously this process must be comprehensive with respect to the involvement of expertise from all world regions. It is also important to recognize that these discussion papers are seen as a starting point for a collaborative effort in partnership with other interested non-governmental organizations. Therefore, we strongly encourage readers to discuss our proposals and we invite comments.

9The term “rehabilitation” can also refer to political issues, e.g. in Dutch and French, where this is the most common meaning; there, what we call rehabilitation in the meaning of the present paper, is called “revalidatie” (Netherlands) or “rééducation fonctionnelle” “réadaptation” (France).
References
9The term “rehabilitation” can also refer to political issues, e.g. in Dutch and French, where this is the most common meaning; there, what we call rehabilitation in the meaning of the present paper, is called “revalidatie” (Netherlands) or “rééducation fonctionnelle” “réadaptation” (France).

