Marta Imamura, MD, PhD1, Christoph Gutenbrunner, MD2, Gerold Stucki, MD3,4, Jianan Li, MD5, Jorge Lains, MD6, Walter Frontera, MD, PhD7, John Olver, MBBS, MD, FAFRM8, Levent Özçakar, MD9, Joel DeLisa, MD, MS10, Linamara Rizzo Battistella, MD, PhD1 and John Melvin, MD11
From the 1Institute of Physical and Rehabilitation Medicine, University of São Paulo School of Medicine, São Paulo, Brazil, 2Department for Rehabilitation Medicine, Hannover Medical School, Hannover, Germany, 3Swiss Paraplegic Research (SPF), Nottwil, 4Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, Switzerland, 5Department of Rehabilitation Medicine, First Affiliated Hospital of Nanjing Medical University, Nanjing, China, 6Centro de Medicina de Reabilitação da Região Centro, Rovisco Pais, Tocha, Portugal, 7Department of PM&R, Vanderbilt University School of Medicine, Nashville, USA, 8Monash University-Epworth Rehabilitation, Melbourne, Australia, 9Department of Physical and Rehabilitation Medicine, Hacettepe University Medical School, Ankara, Turkey, 10Department of Physical Medicine and Rehabilitation, UMDNJ, New Jersey Medical School, Newark, and 11Department of Rehabilitation Medicine, Jefferson Medical College, Thomas Jefferson University, Philadelphia, USA
This paper reports on recent changes and future plans concerning the International Society of Physical and Rehabilitation Medicine. Issues discussed are its structural organization, collaboration and recognition, liaison with the World Health Organization, work in strengthening science, and its future agenda.
Key words: Physical and Rehabilitation Medicine/organization & administration; societies; medical; organisationals structure; non-governmental organisation; World Health Organization.
Correspondence address: Marta Imamura, Institute of Physical and Rehabilitation Medicine, University of São Paulo School of Medicine, São Paulo, Brazil. E-mail: Martaimf5@gmail.com
J Rehabil Med 2014: 46: 97–107
Accepted Nov 21, 2013; Epub ahead of print Jan 13, 2014
Introduction: Aims and mandates of THE ISPRM
The International Society of Physical and Rehabilitation Medicine (ISPRM) is the international organization in the field of Physical and Rehabilitation Medicine (PRM). The society’s mission is “to optimize functioning and health-related quality of life and minimise disability in persons with disability and/or medical problems throughout the world” (Box 1). The ISPRM brings together regional organizations, national societies, and individuals with an interest in PRM.
The work of the ISPRM comprehends 3 main mandates: the scientific, the professional, and the humanitarian (1). The multidimensional nature of the ISPRM leads to a broad spectrum of activities to achieve the mission and goals of the society (Box 1).
|
Box 1. Proposal for a new mission statement of the International Society for Physical and Rehabilitation Medicine (ISPRM) |
|
The mission of the ISPRM is to optimize functioning and health-related quality of life and minimise disability in persons with disability and/or medical problems throughout the world This will be achieved by: • enabling physicians and researchers active in physical and rehabilitation medicine to develop and apply optimal care • strengthening the development and capacity of national organisations of Physical and Rehabilitation Medicine • partnering with international organisations to develop and implement effective disability and rehabilitation policies • promoting collaboration among governments, non-governmental organisations, organisations of persons with disabilities, business and others |
It is important to note that the ISPRM is a non-governmental organization (NGO) in official relation with the World Health Organization (WHO). This means that the ISPRM is obliged to contribute to WHO projects especially in the field of disability and rehabilitation and, at the same time, must disseminate information about WHO’s activities. The collaboration with WHO is defined in 2- or 3-year collaboration plans. The role of the ISPRM as an NGO has to be reflected in its working and decision-making structure, which must follow democratic and transparent principles.
The international scope, the broad spectrum of mandates, and the challenging mission requires efficient working structures and organizational management. In order to achieve these, ISPRM is involved in a process of structural reorganization.
Structural reorganiZation of THE ISPRM
The ISPRM is a non-profit, non-governmental international association. ISPRM’s official bodies are the Assembly of Delegates, the Assembly of Individual Members, the Executive Committee, the President’s Cabinet, and the Council of Presidents. These bodies are composed as described below (Fig. 1).
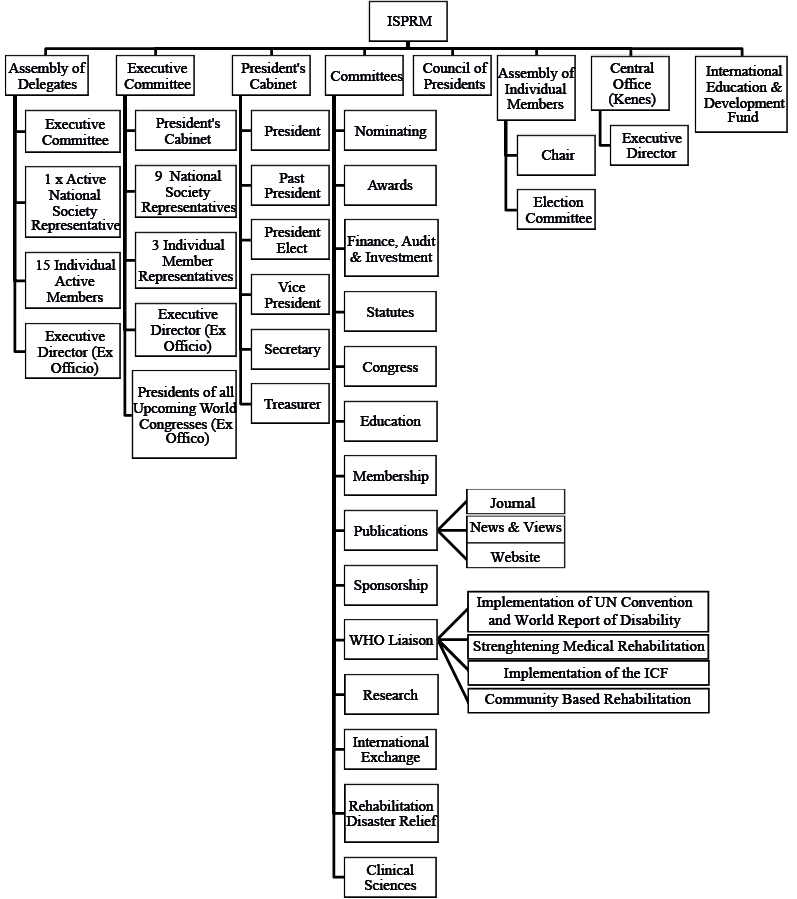
Fig. 1. Official organizational structure of International Society for Physical and Rehabilitation Medicine (ISPRM). WHO: World Health Organization; UN: United Nations; IPSCI: International Perspectives on Spinal Cord Injury; ICF: International Classification of Disability, Functioning and Health.
Membership involvement
Membership of the ISPRM comprises two distinct categories: national PRM societies and individual members. To increase the participation of members in the decision-making process of the society, the voting processes for the election of delegates of individual members and representatives of the various geographical areas have been modified. The Assembly of Delegates consists of representatives of the national societies and of the individual members. In addition, representatives of the regions of the world (see below) are members of the Assembly of Delegates. The Assembly of Delegates elects the Members of the President’s Cabinet and has responsibility for all strategic decisions of the society.
Involvement of ISPRM sub-areas
The ISPRM aims at an equal contribution of PRM specialists and scientists from all parts of the world, both in the election of representatives and in the various committees. To achieve this goal a definition of geographical areas and sub-areas of the world is of major importance. In the past, ISPRM was structured into 5 regions (North America, Latin America, Europe, Africa and Middle East, Asia and Oceania) (Table I). This division did not match the structure of world regions used by the WHO (Table I, column 1). The main difference between these approaches was that the WHO considered all of the Americas together, while Africa and the Middle East and Asia and Oceania included 2 regions. Because the ISPRM, as an NGO, collaborates closely with the WHO, an adaptation of ISPRM regions or areas to the WHO’s concept was proposed and approved (2). This new division is based on 3 large world regions: (i) The Americas; (ii) Europe, Middle East and Africa; and (iii) Asia and Oceania. These regions were named ISPRM World Areas and used as a basis for the nomination of ISPRM presidents and the location of World Congresses (Fig. 2) (3).
However, for practical and operational purposes a further subdivision of these world areas is needed, e.g. to define the background of members of the Scientific Committee for the world congresses. In that context a 3 × 3 × 3 model was proposed to include a minimum of 3 members from each of the large 3 areas and a minimum of one member from each of the sub-areas (3). Again, the purpose of this arrangement is to maintain equity among the various areas and sub-areas and to avoid dominant representation from any single area of the world. Such a concept can only work if all areas can be structured in 3 sub-areas in an appropriate way (Table I and Fig. 2).
|
Table I. World regions of the World Health Organization (WHO) and United Nations (UN), and the International Society for Physical and Rehabilitation Medicine (ISPRM)’s world areas and sub-areas |
||||
|
WHO and UN regions and subregions |
ISPRM areas and sub-areas |
|||
|
WHO regionsa |
UN subregionsb |
|
ISPRM world areas |
ISPRM sub-areas |
|
Region of the Americas |
North America |
The Americas |
North America |
|
|
Central America and Caribbean |
Middle America |
|||
|
South America |
South America |
|||
|
European region |
Northern Europe, Western Europe, Southern Europe and Eastern Europe |
Europe, Eastern Mediterranean and Africa |
Europec |
|
|
Eastern Mediterranean region |
Western Asia |
Eastern Mediterraneand |
||
|
African region |
Northern Africa, Western Africa, Middle Africa, Eastern Africa and Southern Africa |
Africa |
||
|
South East Asia region |
Central Asia and Eastern Asia |
Asia and Oceania |
Central and East Asia |
|
|
Western Pacific region |
Southern Asia and South-eastern Asia |
South and South Eastern Asia |
||
|
Micronesia, Melanesia, Polynesia, Australia and New Zealand |
Oceania5 |
|||
|
awww.who.int/about/brochure_en.pdf (18 September 2012). bunstats.un.org/unsd/methods/m49/m49regin.htm (18 September 2012); this document provides a list of included countries. cIn ISPRM Israel is included in Europe. dWHO terminology was used in this case. eThe term “Oceania” was used because it is established in Physical and Rehabilitation Medicine (name: “AOSPRM”). |
||||
Fig. 2. Areas and sub-areas of the world (from reference 3).

The new structure is fully compatible with the United Nation’s (UN) structure of sub-regions (Table I, column 2), with a few exceptions where the ISPRM new structure comprises more than 1 UN sub-region (Northern Africa, Western Africa, Middle Africa, Eastern Africa and Southern Africa are combined into one region). With the approval of the appropriate governing bodies of the ISPRM the list can be used for the purpose of nomination of experts to the scientific congress and other committees, but for other purposes that require proportional participation.
New central office
In parallel with the growth of the organization, ISPRM decided during the 2011 Congress in Puerto Rico, to end relations with the previous Central Office and to look for a new management company that could support the growth of ISPRM membership and strategy worldwide. ISPRM selected Kenes Associations Worldwide® (KAW) for this purpose. KAW is uniquely dedicated to the management of medical associations and has offices in Europe, Latin America, Asia Pacific, and soon North America. The headquarters of KAW are located in Geneva, Switzerland, where ISPRM is already registered as a non-profit organization. The transition plan for the association management with KAW comprehends the points summarized in Table II. Kenes International® will be providing services to ISPRM on the following main 3 levels:
• Level 1: executive and membership management.
• Level 2: communications services, platforms and technologies, webcasting.
• Level 3: consulting in strategic planning, financial management, campaigns and public relations, fundraising.
A direct result of this transition was a significant cost reduction in secretariat services of nearly 50% and an increase in services provided to ISRPM.
|
Table II. Characteristics and services of the new management company |
|
|
Kenes Associations Worldwide will meet the following prerequisites in meeting the needs of ISPRM: |
|
|
• |
One point of contact for association management through a qualified Executive Manager with experience in general administration and office management. |
|
• |
Expertise and solid experience in managing medical non-profit associations and in registering an association such as ISPRM as a non-profit organization in Geneva, Switzerland. |
|
• |
A headquarter office, fully operational and centrally located in Geneva and access to boardroom at no charge as well as boardrooms in Kenes Group location. |
|
• |
Professional guidance from Executive Director as needed. |
|
• |
Conformity with bylaws and procedures. |
|
• |
Strategic planning and support of the President’s priorities. |
|
• |
All ISPRM records will be maintained in an online repository. |
|
• |
Advice on legal issues and Directors and Officers Errors and Omissions insurance. |
|
• |
Maintenance of the ISPRM calendar of important dates. |
|
• |
Access to full range of business, financial, public relations, fundraising expertise and communications technology and website maintenance. |
|
• |
Expertise in public relations, branding and marketing (including website management and newsletter production). |
|
• |
Expertise in preparation of sponsorship grants. |
|
• |
Expertise in membership development and administration and database management. |
|
• |
Finance and accounting expertise and ability to produce regular financial statements and reports, bank accounts management. |
|
• |
Solid knowledge and experience in coordination of governance and committee meetings. |
|
• |
Liaison with WHO and coordination of translations through members in WHO languages. |
|
• |
Option for pre-financing the website from ISPRM shared congress profits. |
|
WHO: World Health Organization; ISPRM: International Society for Physical and Rehabilitation Medicine. |
|
Collaboration and mutual recognition
In addition to the direct involvement of the membership it is crucial for ISPRM to establish close collaboration with other regional societies. This includes PRM organizations in the various areas and sub-areas of the world, such as the Latin American Association of Medical Rehabilitation (AMLAR), the Asian Oceania Society for PRM (AOSPRM), the Pan-Arab Association of Physical Medicine and Rehabilitation (PAPMR) and the European Bodies in the field (European Society for Physical and Rehabilitation Medicine (ESPRM); European Union of Medical Specialists (UEMS) PRM Section; and European Academy for Rehabilitation Medicine (EARM)). Furthermore, close collaboration with other professional societies around the world that are active in medical rehabilitation is also crucial for the success of ISPRM. Collaboration with area bodies is now established by mutual recognition agreements.
Mutual recognition agreements with PRM societies in various areas/sub-areas of the world
The purpose of this initiative is to establish close cooperation with PRM organizations in various areas/sub-areas of the world, to create a structure of cooperation in mutual recognition that fits the WHO’s working agenda, to support communication between the WHO areas and across borders, to integrate neighbouring areas/sub-areas, and to strengthen the integration and communication of multiregional activities within ISPRM. Such cooperation should include all of the main working areas of ISPRM and the 3 mandates mentioned above (Table III).
|
Table III. Mutual recognition work plan |
||
|
ISPRM mandate |
Related work plan |
|
|
1. |
Humanitarian mandate |
Analysis and implementation of the World Report on Disability: analysis of the impact on the regional situation and development of guidelines for the implementation into health strategies. |
|
Implementation of ICF: e.g. ISPRM proposes to facilitate the recruitment of experts for the project to describe the functional properties of the 100 most frequent diseases in rehabilitation and the ISPRM project to develop an ICF-based tool to measure functioning and disability. |
||
|
2. |
Professional mandate |
Contribute to the development of ISPRM definitions for functional syndromes and clinical guidelines for its PRM treatment and management. |
|
Discussion about the conceptual descriptions of rehabilitation as a health strategy and of PRM as well as the rehabilitation service matrix including the development of use-cases. |
||
|
3. |
Scientific mandate |
Connect PRM journals from the respective region to the ISPRM web of journals. |
|
Appointing at least 3 members nominated by the 3 European Bodies to the scientific committee of the 9th World Congress of the ISPRM in Berlin 2015 and organising a session in the congress. |
||
|
ICF: International Classification of Disability, Functioning and Health; PRM: Physical and Rehabilitation Medicine; ISPRM: International Society for Physical and Rehabilitation Medicine. |
||
Specific collaboration efforts are:
1. Implementation of the UN Convention on the Rights of People with Disabilities and the World Report on Disability at the regional levels (including analysis and dissemination).
2. Definition of PRM on the basis of the comprehensive model of human functioning and description of the principles of PRM services within the framework of a service matrix.
3. Implementation of the International Classification of Functioning, Disability and Health (ICF) in terms of the assessment of disability in rehabilitation practice (including the development of appropriate tools and its application for data collection).
4. Organization of ISPRM World Congresses in combination with regional meetings.
5. Collaboration of regional and international journals (a “web of journals”).
Such mutual recognition agreements were signed in 2012 with the Latin American and European bodies active in PRM (AMLAR, ESPRM, UEMS-PRM-Section and Board, EARM). In 2013, similar agreements were signed with the AOSPRM and the PAPMR. A mutual recognition agreement was also signed with Rehabilitation International (RI).
Another goal is to support communication among WHO areas and across their regional borders to integrate neighbouring regions (e.g. Europe, Middle East and Northern Africa). Thus, mutual recognition agreements have been signed between the ISPRM and the Baltic & North Sea Forum on Physical and Rehabilitation Medicine (BNF-PRM); the Mediterranean Forum of Physical and Rehabilitation Medicine (MFPRM) and the ASEAN Rehabilitation Medicine Association (ARMA). This will strengthen the communication of multi-regional activities within the ISPRM. In particular, it will contribute to the inclusion of other countries to the activities of the ISPRM (e.g. Russia, Belarus and Ukraine).
All mutual recognition agreements include a 2-year working plan that has already been defined. An example of activities included in these plans is the organization of separate scientific sessions (with simultaneous translation into Spanish) by AMLAR in the 7th World Congress of the ISPRM, held in Beijing, China, in 2013.
Collaboration with other societies
Many medical conditions result in impairments and disability. These require rehabilitative interventions. Thus, it will be relevant to ISPRM to develop collaborations with other professional organizations with an interest in the population of persons with disabilities. This may also be relevant for the PRM professionals who should educate our colleagues in other medical specialties on key rehabilitation procedures recommended during the acute phases of particular pathologies (Table IV).
|
Table IV. Example of international societies in rehabilitation and related fields and their specific topics |
||
|
Society |
Geographical coverage |
Pathologies discussed |
|
Rehabilitation International |
Worldwide |
General rehabilitation |
|
Stroke International |
Worldwide |
Stroke |
|
International Association for the Study of Pain (IASP) |
Worldwide |
Pain |
|
International Spinal Cord Society (ISCoS) |
Worldwide |
Spinal cord |
|
International Society Prosthetics and Orthotics (ISPO) |
Worldwide |
Prosthetics and orthotics |
Collaboration with industry partners
Several companies develop and manufacture products that are important during the rehabilitation process and/or enhance functional independence of people with disabilities. Thus, it may be appropriate for ISPRM to collaborate with industry partners who have an interest in developing such technologies and assistive devices.
ISPRM’s role as A Non-Governmental Organization
As mentioned above, ISPRM is an NGO in official relation with the WHO. ISPRM has to contribute to WHO’s activities in the area of disability and rehabilitation and, at the same time, help to disseminate information about the activities of the WHO among ISPRM’s members.
ISPRM’s liaison with WHO
The president of the ISPRM appoints an ISPRM-WHO-Liaison officer for the term of office of his/her presidency. This officer’s responsibility is to maintain regular contact with the WHO, in particular with the WHO’s Disability and Rehabilitation Team (DAR-Team). The officer participates in official WHO meetings, such as the Executive Board and the World Health Assembly, and is ready to react to WHO’s initiatives and inquiries. As this is an ambassadorial function, the president invites the ISPRM-WHO-Liaison-Officer to the Executive Committee meetings of ISPRM. The work related to this role of ISPRM as NGO is predominantly carried out by the ISPRM-WHO-Liaison-Committee (ISPRM-WHO-LC) and guided by 2-year collaboration plans (actual period of plan: 2011–2013).
Collaboration plan with the WHO
According to the collaboration plan with the WHO for the years 2011–2013, the following projects are in progress:
1. Contribution to WHO meetings at the regional and international levels as well as to special meetings to discuss the Implementation of the World Report on Disability and the Rehabilitation Guidelines Review Committee.
2. Involvement of the WHO representatives in ISPRM World Congresses, including participation in the plenary sessions. This was implemented in the 7th World Congress of ISPRM held in June 2013 in Beijing.
3. Dissemination, analysis and implementation of the World Report on Disability (WRD). This activity included the participation in the discussion on the presentation of the WRD in the UN headquarters in New York in 2012 and in the strategic meeting in Geneva shortly afterwards. The focus of ISPRM’s contributions is the identification of gaps in the inclusion of people with disabilities worldwide and in the development of rehabilitation strategies. This work is carried out in closed collaboration with the other rehabilitation professions and the WHO DAR professional organizations network. An article on the WRD and its impact on PRM was published in the Journal of Rehabilitation Medicine (JRM) (4). In addition, a special supplement to the American Journal of Physical Medicine and Rehabilitation on the regional implications of the WRD is in press.
4. Participation of ISPRM’s Natural Disaster Relief Committee in the definition of early rehabilitation after natural disasters. ISPRM will contribute to the planned two-page checklist of minimum responses required in emergencies. This will include concrete action points and a detailed list of existing resources for addressing the needs of persons with disabilities in emergencies. Moreover, ISPRM will compile a database of international experts for PRM in disaster relief, which may provide a PRM professional volunteer team when it is needed in any region of the world. In order to do this, a series of scientific meetings have been held as part of ISPRM’s congresses and interim meetings and some conceptual and scientific papers have been published (5).
5. Development of a common definition or description of rehabilitation as one of 4 main health strategies (6) including the competencies of PRM and the parameters to classify rehabilitation services (7, 8). This work has been started by discussing conceptual descriptions of rehabilitation and of PRM, based on the ICF-model and classification, and with the development of a rehabilitation service matrix and criteria for community-based rehabilitation strategies focusing on the needs of people with disabilities in developing countries.
6. Implementation of the ICF at the clinical level and in population-based epidemiology, including the testing and validation of ICF Core Sets in all WHO regions and more than 35 countries in cooperation with the DAR team and the (Classifications, Terminology and Standards (CTS)) team of the WHO. This project includes the use of ICF Core Sets as international standards for the documentation, reporting, and use in clinical practice along the continuum of care from the acute hospital to integration in the community. The ICF Core Sets are also used to identify the functional impact of the 100 most frequent health conditions in rehabilitation and to develop a generic assessment tool to evaluate disability at a population level.
7. The ISPRM also will actively contribute to the review and, as advisors for the newly developed community-based rehabilitation guidelines, contribute to any inter-professional agency initiatives to develop a joint curriculum for rehabilitation professions. Furthermore, the ISPRM is contributing to the development, dissemination and implementation of an international perspective on spinal cord injury.
Strengthening science in PRM
As mentioned above, strengthening science in the field of PRM is one of the main goals and mandates of ISPRM. This is in line with one of the recommendations of the World Report on Disability (9), which views lack of research in rehabilitation as a barrier for persons with disability to get optimal care. To take leadership in science among others, the ISPRM will be taking the following actions:
• Describing the scientific field of PRM (10, 11) and defining relevant scientific topics (12).
• Ensuring regular and high-level scientific communication and exchange via the web of journals (13, 2) and scientific congresses (see below).
• Providing education and training in science, e.g. by the São Paulo-Harvard courses (see below).
ISPRM scientific topic list
Congresses are one of the core activities of scientific and professional societies. It is of major importance to ensure that recent scientific developments are included in the congress programme and to enable continuous communication among experts in the different core topics and areas of expertise. In order to increase continuity of the discussion in World Congresses, the Congress Committee of ISPRM developed a comprehensive abstract topic list in close cooperation with the Presidents and Chairpersons of the scientific committees of the ISPRM World Congresses in 2012, 2014 and 2015, to be used both for congress announcements and for abstract submission (12).
The first version of this list was based on the definitions of human functioning and rehabilitation research that describes distinct areas of inquiry in PRM. Five main areas of research were identified based on the WHO model of human functioning (biosciences in rehabilitation, biomedical rehabilitation sciences and engineering, clinical PRM sciences, integrative rehabilitation sciences, and human functioning sciences) (Fig. 3) (11). For the abstract topic list, these research areas were grouped according to the proposals of congress themes or tracks. In a second step, the first version was systematically compared with the topics of the 2003 ISPRM World Congress.
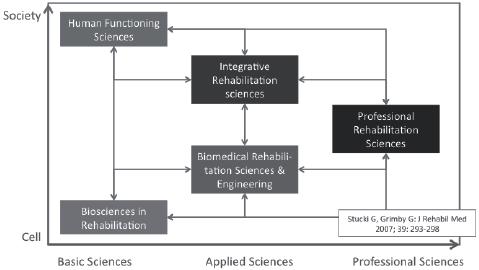
Fig. 3. Model of main areas of Physical and Rehabilitation Medicine (PRM) sciences (from reference 11; modified).
The new regular abstract topic list is comprehensive and includes a full range of topics. It is comparable with those used in other regional and international scientific societies, e.g. in pain research and rheumatology. Such a list may also be helpful to structure research in PRM elsewhere, e.g. for research funding programmes and other scientific information tools within the field.
ISPRM congress standards
As mentioned above, the ISPRM World Congresses is one of the most important activities of the society. However, participation in the congress is still not satisfactory. Some ISPRM members state that they prefer to attend other conferences that are more focused/limited to their special interest. It has been pointed out that the scientific level is variable and sometimes not optimal. We believe that both the quality and the attractiveness of the Congress were significantly enhanced in our 2013 World Congress in Beijing.
Congress goals. The following functions can be seen as the main goals of ISPRM congresses:
1. Science:
(a) Presentation and discussion of recent research projects
(b) Information about new trends in research and recent results
2. Education:
(a) Updates on best clinical practices
(b) Improving clinical skills
3. Policy:
(a) Discussion about the specialty and its position in the health system
(b) Promoting awareness of the field of PRM among the general public and the medical community
(c) Presentation of the WHO projects
4. Socializing:
(a) Networking
(b) Personal interactions
(c) Encouraging involvement of early-career professionals
Scientific and educational programme. In order to achieve these goals the congress programme must meet the expectations of the participants, especially in providing new information and knowledge. The scientific programme should include two main sections:
• The first section should ensure continuous communication of important scientific findings. This part is uniform in all ISPRM World Congresses and is the basis of the standard programme. This part of the programme contains mainly original papers selected from the abstract submitted according to the ISPRM topic list. Some invited lectures, mainly from PRM experts, may also be included. In this section, special interest groups can organize their own sessions with a narrower focus.
• The second section presents a more in-depth discussion of selected topics of recent interest. This section mainly includes invited lectures by researchers and experts, but it should also include speakers from outside PRM. The aims of this second part of the programme are to discuss new topics and stimulate innovation in the field, and to provide new information from closely associated fields. Local experts from the host country or region should participate.
With regard to ISPRM’s special role as NGO in official relation with WHO, one plenary session should be on the subject of a recent topic related to the ISPRM-WHO liaison.
The educational programme should include different formats, such as seminars and hands-on workshops, to emphasize the development of practical clinical skills. In addition, best-practice sessions about clinical topics should be included, including guidelines and best practices as well as translational aspects of research.
In order to reach to a wide audience with diverse interests, the programme should include sessions in the 5 official WHO languages with topics of special interest, collaborative sessions with other societies and partners of ISPRM (e.g. International Society Prosthetics and Orthotics (ISPO), RI and others), satellites and breakfast/lunch symposia (e.g. in collaboration with industrial partners), governance sessions (to be conceptualized), and other types of activities.
ISPRM Scientific Committee. In order to guarantee the highest possible scientific level and to ensure its continuity, the scientific committee of ISPRM should be actively involved in the preparation of the scientific and educational programme together with the local organizing committee. The scientific committee should include experts from the main scientific fields of ISPRM and members from all ISPRM World sub-areas. They are selected by their expertise in the main ISPRM topics and their scientific activities. The committee will have its first meeting in Cancun in June 2014 and should be renewed regularly.
Research networks and online training
Research networks. Due to the impressive developments in medicine in the last few decades, the performance and publication of scientific research have already become important activities for any medical specialty. The very survival and progress of medical specialties may very well depend on the successful generation of new knowledge. Academic strength is noteworthy, not only from a scientific point of view, but also from the point of view of the quality of medical care provided to those in need. Scientific research is required to demonstrate that clinical interventions are beneficial.
In terms of research, ISPRM needs to communicate effectively the importance of research, develop an appropriate scientific agenda, and contribute to the development of research capacity. One crucial strategy in this regard is the training of our future generation of researchers. The following can help us achieve that goal:
• Develop mechanisms to support and reward successful young PRM physicians (i.e. scholarship, registration waivers, free journal subscription, etc.).
• Disseminate stories of successful PRM research.
• Conduct research training workshops in different countries and/or during the World Congresses (a workshop was included in the programme of the 2013 World Congress in Beijing).
• Develop a research centres of excellence network for conducting PRM research.
Online training. Education of future generations is of utmost important. ISPRM is focusing on the use of online strategies for this purpose. Two important points must be highlighted:
• The use of new teaching approaches including the concept of collaborative learning. For this purpose, a platform is planned to be constructed for conducting several online courses for PRM physicians worldwide.
• Aside from being able to by-pass the possible access barriers experienced by various physicians, that approach and technology can be used for lengthy supervised interactive training. We have developed a novel global training programme based on the collaborative learning method using the tools of Web 2.0. The platform used allows delivery of up-to-date and state of the art distance-learning courses, combining traditional and novel learning approaches that can be broadcast to several participating centres around the world. Two main features of this approach are interaction and collaboration, which are two critical aspects to induce learning in the setting of distance-learning courses. Some of these features include discussion forums, blogs, weekly polls, podcasting, and case discussion group-projects whereby student’s work on a challenging case related to the module using the Wiki platform. In addition, interactions with faculty and staff are made via chat and a two-way video-conferencing system. In summary, 3 methods of learning using techniques of computer-supported collaborative learning are combined in the programme: web-based learning, collaborative learning, and problem-based learning. Web-based learning consists of using the internet as a support platform for the course. Collaborative learning comprises stimulation of experience and knowledge sharing among participants. The idea is that participants work together toward common goals and each can contribute to fill in gaps in knowledge, therefore using the concept of learning through teaching. In problem-based learning, students are placed in an active problem-solving environment, training them to identify what they need to learn to solve the presented problems, thus filling their previous knowledge gaps. This educational programme attempts to overcome the obstacles of improving postgraduate training in the field of PRM. Initial courses in the planning stages will be on chronic pain, musculoskeletal ultrasound, and fascial manipulation.
ISPRM’s web of journals
Scientific journals represent one of the most important mechanisms to disseminate scientific, medical, and health policy information. The publication of research findings, clinical observations, educational articles, and policy discussions in scientific journals is one of the pillars of scientific and clinical progress of any medical specialty. Thus, it is important for ISPRM to support journals dedicated to PRM and to make their content available to professionals in the organization. One of the ways of accomplishing this goal is to develop a virtual web of journals that will be recognized as an important part of ISPRM’s mission and provide a unique service to our members. This web of journals can also be instrumental in the publication of professional content that may not be research-based, such as educational guidelines. Proposed in the first article on the way forward for ISPRM (2), the web of journals is now a reality. The Sub-committee of Publications of the Publications Committee has been making progress in the “construction” of this web.
This web of journals represents an electronic communication network linking all individuals and national societies interested in the advancement of our field. By definition, journals included in ISPRM’s web have to be dedicated to the advancement of PRM and can be divided into 3 categories:
1. One official journal of ISPRM.
2. Journals “published in association with ISPRM”.
3. Journals “endorsed by ISPRM”.
All of these journals have a link to the ISPRM’s website and the electronic version of these journals is available to ISPRM members at no cost. Some of the content is immediately available to the members and some articles are available after several months of publications.
Since 2006, the official journal of ISPRM has been the JRM. JRM is an excellent international journal published independently by a not-for-profit foundation that circulates internationally. It also publishes the abstracts of World Congress and important manuscripts discussing the policies of ISPRM. ISPRM participates in the development of the journal official policies.
In the last 3 years, the European Journal of Physical and Rehabilitation Medicine, the Portuguese Journal of Physical and Rehabilitation Medicine, and the French Journal of Physical and Rehabilitation Medicine were approved by the President’s Cabinet of ISPRM as journals “published in association with ISPRM”. In addition the journals Rehab in Review and The Chinese Journal of Physical and Rehabilitation Medicine are now recognized as “endorsed by ISPRM”. The electronic version of these journals is available to ISPRM members on the official website of the Society.
The concept of a web of journals has been accepted by colleagues in various ISPRM areas and sub-areas; thus, several other journals have applied for one of the above categories and are being evaluated by the Publications Committee of the ISPRM and the President’s Cabinet for potential inclusion in the web of journals. In the future, ISPRM should strengthen this web and use it to reach individual members and national societies, raise the profile of PRM research, and contribute to the body of knowledge that supports scientific and medical endeavours around the world.
The way forward
In 2013 the President of the ISPRM presided over a strategic planning meeting that included the President’s Cabinet, some ISPRM committee chairs, and selected members. Information about this meeting is given in the articles on “The way forward” (2 and present paper), describing new developments and challenges and defining a concrete 2-year working plan.
future direction
It can be concluded from the above discussion that the comprehensive and worldwide mandate is highly challenging for the ISPRM. This will require a very efficient organizational structure and increased involvement of members from all areas and sub-areas of the world. Thus, an important focus of our activity is improvement of the ISPRM’s organizational structure, including the consequent implementation of democratic and transparent processes. With regards to the scientific mandate of the ISPRM, major activities have been started to improve scientific education, communication and standards. Last, but not least, with the new “Clinical Sciences” committee a basis for the improvement of practicing PRM based on scientific knowledge has been established recently. Another important focus is the role of ISPRM as an NGO in special relations with the WHO. This can be done effectively by developing a close working relationship with the WHO and with the involvement of the ISPRM Liaison Officer in relevant WHO activities. These activities are closely related to the humanitarian mandate of the ISPRM (e.g. disaster-relief activities) and also relate to the professional mandate (conceptualizing medical rehabilitation and PRM).
Working agenda 2012–2014
The working agenda for the years 2012–2014 has been developed by continuing the previous work plan (14), adding the aforementioned recent topics and additional plans. Table V shows the updated working plan (3).
|
Table V. International Society for Physical and Rehabilitation Medicine (ISPRM) policy agenda for the years 2012–2013 (3) |
|||
|
Strategic goal |
ISPRM activities |
Status of ISPRM activities |
|
|
1. |
Enhancement of collaboration with regional PRM societies |
Establishment of mutual recognition and collaboration plans with regional PRM societies (following the model of the WHO DAR/ISPRM collaboration plan). |
Mutual recognition agreements between ISPRM and the European PRM Bodies (ESPRM, UEMS-PRM Section and Board, EARM), the PARM, AMLAR and the AOSPRM have been signed. Additionally a mutual recognition agreement with the Baltic and North Sea Forum, the Mediterranean Form of Physical and Rehabilitation Medicine and the ASEAN Rehabilitation Medicine Association has been signed. |
|
2. |
Improve organisation structure and internal management of ISPRM |
ISPRM’s activities will be managed more effectively. Information will be provided for members and executives. This includes among others update of databases, such as membership lists, tracking working processes and information management. In addition, fundraising and sponsorship will be optimized. |
After signature of cooperation Kenes International works on an improvement of all managerial processes within ISPRM. |
|
3. |
Enhancement of ISPRM congresses |
Enhanced involvement of central offices in ISPRM congresses and of ISPRM officials in scientific committees and programmes. |
From 2016 onwards all World Congresses will be organised under the responsibility of Kenes International as PCO. New congress standards will be implemented step by step from the 2013 Congress on. The scientific programme will be structured according to the new ISPRM topic list. An ISPRM scientific committee will be established consisting of members from all nine ISPRM sub-areas. The ISPRM scientific committee will have regular meetings. |
|
4. |
Improvement of network of scientific cooperation and publication organs |
1. ISPRM aims at creation of a network of scientific journals in order to provide enough journals for peer reviewed publication in the field and its subfields as well as to avoid self-citation. 2. In addition, the exchange of young scientists will be supported by ISPRM. |
1. Besides of the official journal ISPRM collaborates with a number of peer reviewed scientific journals either as endorsement or association. 2. An exchange programme for young scientists has been established. Both activities are followed up continuously. |
|
5. |
Democratization of ISPRM governance structure and election procedures |
Creation of Individual Members Assembly and move from nomination and approval to election of representatives by Assembly of Delegates. Election of 3 representatives of individual members (1 per ISPRM world area) and 9 representatives of national members (3 per ISPRM world area) into Executive Committee by Assembly of Delegates to replace previous ISPRM regional vice-presidents. |
After deciding on the new structure it is put into practice step by step, starting from the elections in the interim meeting in Atlanta 2012. |
|
6. |
Supporting the establishment of rehabilitation services worldwide |
1. Discussion paper with working title “ISPRM’s potential roles in fostering the establishment of PRM services in low resourced settings”. 2. New items for WHO DAR/ISPRM collabora- tion plan have been proposed by ISPRM. 3. Minimum requirements will be defined for rehabilitation physicians and other health professionals involved in rehabilitation services. These requirements will give support to developing countries to establish effective rehabilitation services. 4. Structural models will be provided for the development of rehabilitations services in countries with different development levels. |
1. Discussion paper is currently under technical reviewed by the WHO Liaison Committee. 2. Proposed new WHO DAR/ISPRM collaboration plan currently under review by the WHO. 3. A task force will elaborate minimum requirements for education of rehabilitation physicians and other health professionals active in rehabilitation services. 4. Structural models will be developed based on a new classification approach for medical services and collaboration of the new subcommittee on “Community-Delivered Rehabilitation”) and based on WHO’s CBR guidelines. |

|
Table V. Contd. |
|||
|
Strategic goal |
ISPRM activities |
Status of ISPRM activities |
|
|
7. |
Developing rapid rehabilitation response to natural and man-made disaster |
Conceptualisation of ISPRM for natural disaster relief strategies and scientific founding for such concepts. |
1. Publication of conceptional papers and sessions about natural disaster relief in scientific meetings. 2. Development of a concept of an interventional task force in close cooperation with WHO. |
|
8. |
Enhancement of research capacity |
1. Establishment of a clinical science committee and identification of scientific topics with high priority. 2. Develop and implement educational structures to increase scientific work capacity. |
1. A new clinical sciences committee has been established in 2012 and will develop a working agenda until June 2013. Special interest groups for concrete work will be founded. 2. Harvard educational courses on principles and practice of clinical research have been implemented. Additional projects will be developed. 3. Regular reviews will be provided in MediGrip. Its concept will be enhanced until 2014. |
|
9. |
Development of ISPRM constituency and membership |
1. Facilitation of foundation of PRM societies. 2. Development of new membership models. |
1. PRM societies in low-resource settings: Identification of white spots provided in discussion paper; development of strategies to support the foundation of new scientific societies. 2. New membership models will be developed in cooperation with Kenes International. |
|
10. |
General curricula in disability and rehabilitation |
General curricula on disability and rehabilitation in medical education have been developed. |
The ISPRM curricula for undergraduate education and for specialist training will be published by the educational committee. Thereafter actions will be taken to implement these at national levels. They will be integrated into the next collaboration plan with WHO. |
|
11. |
Fighting discrimination |
Implementation of the UN Convention on the Rights of People with Disabilities. |
The respective Sub-Committee of the WHO Liaison Committee will be merged with the WHO implementation subcommittee in order to achieve synergetic effects. ISPRM will develop a concept to observe UN-activities and analyse its impact for medical rehabilitation. A concept to increase the number of people with disabilities in medical schools and specialist training centres will be developed by 2013. |
|
12. |
Implementation of the ICF in rehabilitation |
1. Review the process of implementation of the ICF in rehabilitation practice. 2. Define functional properties of the most relevant health conditions in rehabilitation. 3. Develop ICF-based assessment tools for functioning and disability. |
1. A systematic review on the implementation of the ICF in clinical practice was published in 2012. 2. In close cooperation with WHO the ICF Implementation Subcommittee is working on a list of functional properties of the 100 most frequent health conditions in rehabilitation. 2. A project to develop an ICF-based mobility assessment has also been started. Its results will be published in 2015. |
|
13. |
Contribution to WHO guidelines and develop best practice models for implementation |
Developing concepts for community-delivered rehabilitation services, as published by WHO. |
A new subcommittee within the WHO-Liaison committee will be established in mid-2013. It will develop criteria and concepts to improve rehabilitation service delivery in the community. A special focus of this work will deal with the specific situation of low- and middle-income countries. |
|
14. |
Development of best practice models for rehabilitation of patients with specific health conditions |
ISPRM will stepwise develop best-practice guidelines for health conditions with high prevalence in rehabilitation. This includes the definition of functional syndromes. |
The newly founded Clinical Science Committee will develop a strategic plan and a list of priorities. Regular information about existing guidelines will be disseminated, e.g. using the MediGrip App. |
|
15. |
Strengthening medical rehabilitation through unifying taxonomy |
1. Position papers on conceptual descriptions of the rehabilitation strategy and PRM. 2. Discussion paper on rehabilitation services within health services matrix. |
1. Conceptual descriptions of rehabilitation as a health strategy and of PRM have been published and adopted by ISPRM in November 2012 after intense discussion. Explanation of these descriptions and use cases will be published. 2. A framework for the description of rehabilitation services is under development and will be published for further discussion in a series of conceptual papers until the end of 2013 by the WHO-Liaison Sub-Committee on Strengthening Medical Rehabilitation. |
|
WHO: World Health Organization; ICF: International Classification of Disability, Functioning and Health; PRM: Physical and Rehabilitation Medicine; UN: United Nations; UEMS-PRM: European Union of Medical Specialists PRM Section; EARM: European Academy for Rehabilitation Medicine; PARM: Pan Arabic Association of PRM; AMLAR: Latin American Association of Medical Rehabilitation; AOSPRM: Asian Oceania Society for PRM; WHO DAR: World Health Organization Disability and Rehabilitation team; CBR: Community Based Rehabilitation; PCO: Professional Congress Organizer; ESPRM: European Society for Physical and Rehabilitation Medicine. |
|||

