Ché Fornusek, PhD1 and Phu Hoang, PhD2,3
From the 1Exercise Health and Performance Faculty Research Group, University of Sydney, 2Neuroscience Research Australia, University of New South Wales and 3MS Studdy Centre, Lidcombe, Multiple Sclerosis Limited, Sydney, Australia
OBJECTIVE: To investigate the feasibility of neuromuscular electrical stimulation cycling modified to suit persons with advanced multiple sclerosis.
SUBJECTS: Eight women with secondary progressive multiple sclerosis.
METHODS: Subjects participated in an 18-session (40 min) neuromuscular electrical stimulation cycling program. A pedaling cadence of 10 rev•min-1 was employed and stimulation intensity was not modulated to control cadence, but increased gradually throughout each session. The outcomes included the stimulation intensity tolerated, thigh circumference changes, and power output and cardiorespiratory response during cycling. Participants were interviewed about perceived benefits of the treatment including changes in transfer ability.
RESULTS: Seven participants (Expanded Disability Status Scale 6.5–8.5) (mean 7.4 (standard deviation 0.7)) completed the training program over an average of 10 weeks. Greater stimulation intensities were tolerated than previously reported for persons with multiple sclerosis. Increases were found in thigh volume. Perceived benefits included improvements in transfer ability, leg circulation, spasticity and strength.
CONCLUSION: Modifying neuromuscular electrical stimulation cycling allowed persons with advanced multiple sclerosis to tolerate greater stimulation intensities and exercise their muscles more intensely than previous studies. The benefits reported, which were solely due to neuromuscular electrical stimulation cycling, demonstrate that persons with preserved sensation and muscle paralysis/paresis might benefit from neuromuscular electrical stimulation exercise when it is adjusted appropriately.
Key words: electric stimulation; multiple sclerosis; paralysis; exercise.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Ché Fornusek, Exercise Health and Performance Faculty Research Group, University of Sydney, NSW 1824 Sydney, Australia. E-mail: che.fornusek@sydney.edu.au
Accepted Dec 16, 2013; Epub ahead of print Apr 22, 2014
Introduction
Multiple sclerosis (MS) is a degenerative disease of the central nervous system that can affect the brain, spinal cord, and optic nerves. The symptoms include paralysis/paresis, spasticity, fatigue, cognitive impairment, and bowel and bladder dysfunction (1). Persons with MS are generally less active than the general population (2) which may lead to deconditioning that further reduces functional abilities (3). In less severe cases of MS regular exercise is beneficial for managing many MS symptoms (4) and reversing deconditioning due to inactivity (2, 5). Persons with advanced MS (i.e. Expanded Disability Status Scale (6) [EDSS] > 7.0) may find exercise very difficult due to significant fatigue, leg muscle paresis and poor shoulder condition (7). Previous research in exercise for advanced MS has been restricted to arm cranking (7) and short term studies with neuromuscular electrical stimulation (NMES) cycling (8).
NMES cycling exercise (9), which allows paralyzed legs to exercise on a stationary ergometer, might be beneficial for persons with advanced MS (8). During NMES cycling the subject is seated on a stationary recumbent cycle ergometer and pairs of gel-backed electrodes are placed on the quadriceps, hamstrings, and gluteal muscles of each leg. During NMES cycling a computer reads the position of the pedal cranks and controls a muscle stimulator to generate appropriately timed NMES-induced muscle contractions to drive the pedals and produce cycling exercise. In persons with spinal cord injury (SCI), NMES cycling training can increase leg muscle mass, leg blood flow, and improve glucose metabolism, while providing a light aerobic workout (10, 11).
We theorize that NMES cycling exercise may bestow similar benefit to persons with advanced MS. Prior studies have examined NMES cycling in persons with MS, but these earlier studies did not modify the NMES cycling to suit persons with MS (8, 12–14). Specifically, the stimulation control algorithm used in these previous NMES cycling studies was designed for persons with complete SCI; the stimulation amplitude was modulated by automatic feedback to control cycling speed or the power (Fig. 1) (15). Our experience is that this method does not work well in persons with sensation and may limit the stimulation that can be tolerated and the exercise intensity reached.
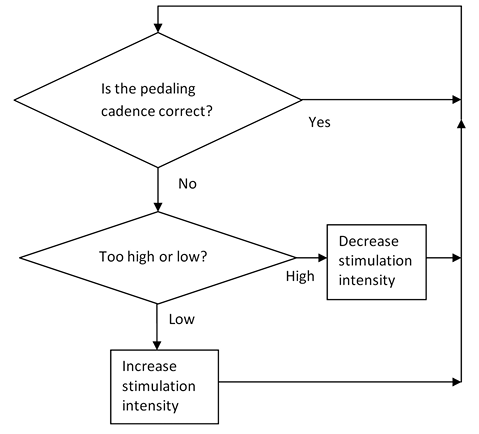
Fig. 1. Algorithm traditionally used to control pedal cadence during neuromuscular electrical stimulation cycling. Stimulation amplitude is modulated to control pedal cadence, i.e. if pedal cadence is too low then stimulation amplitude is increased (to set maximum) and if too high then stimulation amplitude is reduced.
Therefore, the goal of this study was to investigate the feasibility of NMES cycling that we have adapted to suit persons with advanced MS. The NMES cycling was adapted to maximize the stimulation tolerated by increasing the stimulation slowly throughout the exercise session as the patient habituated to the uncomfortable stimulation. A lower pedaling cadence (i.e. 10 rev•min–1) was also used to increase the muscle forces generated (16).
Methods
The experimental protocol used in this research was approved by the Human Ethics Committee of the University of Sydney (Protocol No. 12758) and all participants provided informed consent. This study was performed in the FitAbility clinic at the Discipline of Exercise and Sports Science (University of Sydney).
Participants
Eight participants (mean 39 years (standard deviation (SD) 14); range 30–57 years) volunteered for this study (Table I). Inclusion criteria were that the participants had secondary progressive multiple sclerosis, an EDSS (6) of 6.5–8.5 and were aged 18–65 years. The majority of subjects used a manual wheelchair for daily mobility except for subject H who used a power wheelchair and subjects A and B who walked with bilateral support from a rollator walker. Participants were screened by a medical doctor to ensure that they were fit to partake in NMES cycling exercise. The screening included a full medical history and physical examination. The exclusion criteria for the study were if subjects had lung problems, coronary heart disease, congestive heart failure, epilepsy, uncontrolled hypertension, leg orthopaedic problems, or medical conditions that might preclude them from safely exercising with NMES (e.g. pregnancy, pacemaker/implanted defibrillator, advanced osteoporosis).
|
Table I. Participant characteristics |
|||||
|
Volunteer |
EDSS |
Age, years |
Sex |
Training frequency |
Medications |
|
A |
6.5 |
58 |
F |
2/week |
Galtiramer Acetate |
|
B |
6.5 |
45 |
F |
3/week |
Interferon β 1A, Tizanidine, Atenolol |
|
C |
7.0 |
30 |
F |
2/week |
- |
|
D |
7.0 |
55 |
F |
3/week |
Baclofen |
|
E |
7.5 |
57 |
F |
2/week |
Oxybutynin, Fluoxetine |
|
F |
7.5 |
47 |
F |
2/week |
Mitoxantrone |
|
G |
8.0 |
52 |
F |
2/week |
Baclofen, Diazepam, Gabapentin |
|
H |
8.5 |
50 |
F |
2/week |
Baclofen |
|
Subjects are ordered from less severe to more disability due to multiple sclerosis. EDSS: Expanded Disability Status Scale; F: female. |
|||||
Neuromuscular electrical stimulation cycling training
Each volunteer participated in 18 40-min NMES cycling sessions on a custom designed isokinetic NMES cycle ergometer (9) (Fig. 2). The NMES cycle ergometer consisted of a motorized cycle ergometer (Motomed Viva 1.5, Reck Medizintechnik GmBH, Betzenweiller, Germany), recumbent seating, a notebook computer, and a custom muscle stimulator. Participants were offered the option of training 2 or 3 times per week. If sessions were missed then additional training sessions were performed as necessary to total 18 sessions. The participants were instructed not to push voluntarily during the training to isolate the effects of NMES training; although combined training (voluntary plus NMES) might be expected to bestow more benefit, the purpose of this study was to examine what benefits might be gained from NMES by those severely disabled by MS. To the best of our knowledge none of the participants pushed voluntarily.
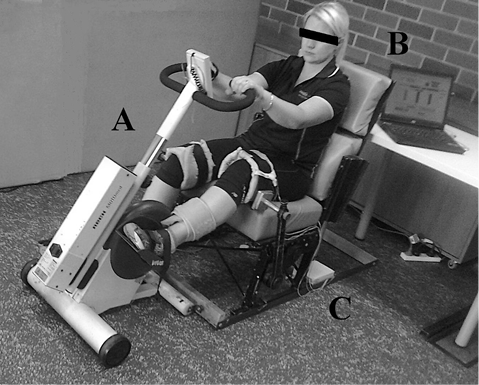
Fig. 2. Neuromuscular electrical stimulation (NMES) cycling setup used in the current study. A: Motomed Viva cycle (Motomed Viva 1.5, Reck Medizintechnik GmBH, Betzenweiller, Germany); B: notebook computer; C: NMES stimulator and leads.
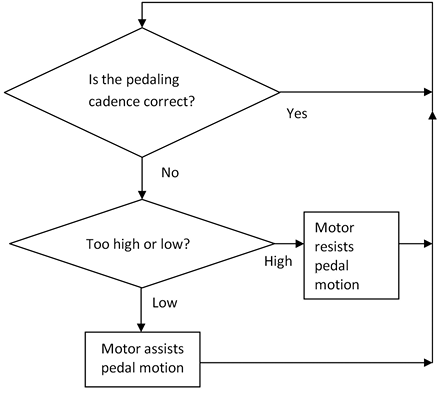
The NMES cycling was modified in two ways from the traditional NMES cycling which was designed for persons with complete SCI and uses cadences between 35–50 rev•min–1. The first modification was that a cadence of 10 rev•min–1 was used. The second modification was to not use feedback control of stimulation intensity to control pedal cadence. The isokinetic design of the Motomed cycle ergometer used a motor to control the pedal cadence (Fig. 3) independently of the stimulation intensity. This allowed the stimulation intensity to be gradually increased in a steady slow predetermined manner during each session.
Initially, the stimulation amplitude was set at 30mA and then slowly increased by the control software at a constant rate to reach a predetermined level at 20 min. If the predetermined stimulation level was too uncomfortable during a given session then the trainer could reduce the stimulation intensity or restrict it from increasing further. Stimulation amplitude was then held at the level achieved at 20 min for the rest of the session. During subsequent sessions participants were encouraged to tolerate greater maximum stimulation amplitude. If stimulation to particular muscles was more uncomfortable, then stimulation intensity could be reduced to those muscles.
Stimulation was delivered to the quadriceps hamstrings and glutei muscles via Empi gel-backed surface electrodes. The stimulator delivered 300 μs pulses at a frequency of 35 Hz; these values are within the range of commonly used values in NMES cycling.
Measurements
To gain an idea of the feasibility of the NMES cycling exercise we measured cycling performance, surveyed perceived benefits, and measured changes in thigh circumference. Stimulation intensity and power output were recorded during all training sessions. These data were used to determine the maximum stimulation intensities tolerated, and mean and peak power outputs during the last (18th) session.
Patient perceptions, perceived therapeutic benefits and detrimental effects
At the completion of the training and testing, participants were asked questions about the beneficial and detrimental effects of NMES cycling. Participants were also asked to rate their impressions of change in standing transfer ability on a 15 point scale, where –7 indicated a “great deal worse”, 0 indicated “no change”, and +7 indicated “a very great deal better”; this question was modeled on earlier research (17).
Thigh circumference measurements and volume calculations
Pre and post measurements were made for thigh circumference with a tape measure on each leg at distal, mid, and proximal positions. The points were measured 10, 20, and 40% of the femur length above the superior border of the patella while the subject was supine. A mean value of 3 measurements was obtained at each site. The thigh circumferences were used to calculate volume changes by representing each leg as two frustums.
Metabolic exercise testing
Additionally, 5 of the subjects performed an additional testing session where cardiorespiratory responses were measured. Heart rate, oxygen uptake (VO2), and Ventilation (Ve) were recorded using an open-circuit spirometry metabolic gas analysis system (Medical Graphics CPX; Medical Graphics Corp, St. Paul, USA) at rest and during the exercise. Heart rate and cardiorespiratory data was averaged over 1 min intervals, then rest and maximum values were extracted from the data. Perceived exertion was assessed from the participants using the 15 point Borg (6–20) Rating of Perceived Exertion (RPE) scale. Participants were asked to rate how painful and tiring the NMES cycling exercise was on a 10 point visual analogue scale (10 being worse pain/most tiring imaginable).
Statistical analysis
After the data was confirmed to be normally distributed, paired t-tests were used to compare between the pre and post values for the thigh volumes calculated from the circumference measurements. SigmaPlot 12.3 was used to perform the statistical analyses. Unless otherwise stated, data are presented as mean with standard deviation (SD).
Results
Seven participants (EDSS mean 7.4 (SD 0.7)) completed the 18 sessions NMES cycling program (see Table II). Subject A quit the exercise program after 13 sessions. The other subjects attended an average of 1.8 sessions per week and completed the program in a mean of 10 weeks.
Over the first few weeks, the maximum stimulation intensity (pulse amplitude) and duration of the session was increased. By the sixth session all participants were performing 40 min of NMES exercise. By the end the mean maximum stimulation delivered to the quadriceps, hamstrings, and gluteal muscles was 91mA (SD 11), 86mA (SD 18), and 69mA (SD 21), respectively. The average cycling power outputs produced for the last training session was 5.2W (SD 2.6) (peak power 7.7W (SD 3.6). The gradual increase in stimulation amplitudes maintained the force of the muscle contractions throughout each training session. Some of the participants reported mild heat sensitivity during the last 10 min of each session which was adequately addressed by using a pedestal fan to cool the subject.
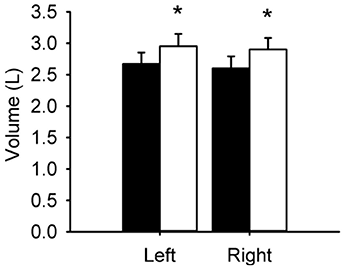
After training the mean thigh circumferences at the proximal, middle and distal thigh measurement positions increased in all but Subject F. For the region of thigh where the circumferences were measured significant increases (Left +10.7%, p = 0.005; Right +11.6%, p > 0.001) were found after training in the calculated thigh volume (Fig. 4).
Overall participants felt that their transfer ability was improved moderately (median 4, interquartile range 2–5) after the training program (Table II). When asked about other benefits, 3 participants reported improved circulation, 2 reported increased strength, and 2 decreased spasticity. One subject reported that they found the exercise especially tiring and another noted that her legs were stiff the next morning after training.
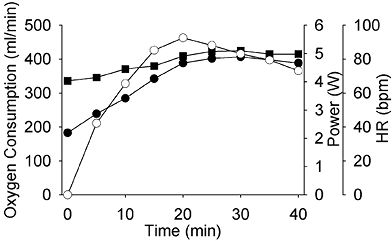
NMES cycling elicited a small increase in cardiorespiratory metabolism in the 5 subjects tested (Fig. 5). Heart rate increased from a mean resting value of 67bpm (SD 9) to a peak of 85bpm (SD 10). Oxygen consumption and ventilation increased from 183 ml•min–1 and 6.9 L•min–1 to 407 ml•min–1 and 17.0 L•min–1, respectively. On a 10 point scale patients indicated that 40 min of NMES cycling was moderately tiring (mean 5.2 (SD 2.7)). The mean stimulated pain sensation was rated as 5.7 (SD 2.2) out of 10. Perceived exertion was rated as light (mean 12 (SD 3)) on the RPE scale (Borg 6–20).
|
Table II. Beneficial and detrimental effects from NMES cycling program |
|||||||||||
|
Participant |
EDSS |
Left volume (Δ%) |
Right volume (%Δ) |
Δ Transfer ability (–7 to +7) |
Peak power (W) |
HR (rest/peak) |
RPE (6–20) |
NMES pain |
NMES induced tiredness |
Benefits reported |
Negative effects |
|
B |
6.5 |
14.5 |
9.9 |
+1 |
7.1 |
(81/100) |
11 |
6.5 |
5 |
↑circulation |
Tiring |
|
C |
7.0 |
11.1 |
18.0 |
+5 |
7.2 |
– |
– |
– |
– |
↑circulation, ↓cramp |
None |
|
D |
7.0 |
13.3 |
11.1 |
+4 |
5.9 |
(62/98) |
14 |
6 |
7 |
↑circulation, ↓pain |
None |
|
E |
7.5 |
8.9 |
17.0 |
+6 |
10.3 |
(62/85) |
13 |
5 |
5 |
↑strength, ↑balance |
None |
|
F |
7.5 |
3.3 |
–1.7 |
+4 |
9.1 |
(71/96) |
8 |
2 |
1 |
↑strength |
Leg stiffness |
|
G |
8.0 |
13.3 |
16.7 |
+2 |
12.8 |
– |
– |
– |
– |
↓spasticity |
None |
|
H |
8.5 |
12.2 |
15.6 |
+2 |
1.5 |
(61/83) |
15 |
8 |
8 |
↓spasticity, ↑muscle mass |
None |
|
Subject A did not finish training program. The variables indicated with a “–“ were not measured for subjects C and G. EDSS: Expanded Disability Status Scale; HR: heart rate; RPE: Rating of Perceived Exertion; NMES: neuromuscular electrical stimulation. |
|||||||||||
Discussion
The novel features of this study are that we have adapted NMES cycling to persons with MS and then explored the feasibility of NMES cycling for advanced MS via an 18-session training program. Even though males were eligible for this study, all participants were female, which is likely related to a combination of sexual disparity in the incidence of MS (18) and perhaps selection bias related to the potential to commit to the study. We found that women with advanced MS can tolerate sufficiently high intensities of stimulation during NMES cycling to induce acute increases in cardiorespiratory metabolism and produce gains in thigh volume over 18 sessions. We expect that males would have responded similarly to the female participants. The gains in thigh volume in the current study are consistent with prior NMES cycling findings in persons with SCI (19). Changes in thigh circumference do not give an accurate measure of muscle mass changes, since changes could also be due to changes in fat mass changes; subject F illustrates this point. However, we expect the thigh volume changes were due to muscle hypertrophy.
Additionally, all participants felt that their transfer ability was improved. The participants with EDSS 7.0 and 7.5 reported that their ability to transfer had improved the most (i.e. in the range of moderately better to a great deal better). These individuals all used manual wheelchairs for daily mobility and 3 of these 4 were able to transfer independently. They may have benefitted the most because they can voluntarily contract their quadriceps muscles and the NMES may have reversed muscle weakness due to secondary disuse atrophy. The other individuals may not have perceived benefit because they already had enough significant leg strength to walk (subject B) or not enough leg strength and relied on others for transfers (participants G and H).
The participants reported a variety of other peripheral benefits ranging from improved strength, circulation, and decreased leg spasticity. Since participants were instructed not to push during the cycling exercise, even if they were able, these benefits are solely due to the electrical stimulation exercise. NMES cycling exercise was reported as tiring but all participants could tolerate 40 min exercise sessions after 2–3 weeks of training.
Prior to this research, it was not known if the presence of sensation in persons with advanced MS would severely limit the NMES intensity (8), the exercise intensity and the potential benefits bestowed due to long-term training. The method of NMES cycling in this feasibility study was changed in two ways from traditional NMES cycling to suit persons with MS; a low pedaling cadence was used and stimulation pulse amplitude was increased gradually at a slow but constant rate for the first 20 min of the exercise session. The isokinetic nature of the NMES cycle used in this study (9) allowed both these deviations from traditional NMES cycling. Low cadence training (i.e. 10 rev•min–1) produces greater muscle forces and more hypertrophy compared to the higher cadences traditionally used with NMES cycling (i.e. 50 rev•min–1) while still providing an equivalent cardiorespiratory workout (19, 20).
Literature suggests that if a greater stimulation intensity can be employed then a greater muscle mass will be recruited and more benefits will be gained (21, 22). In a prior NMES cycling study in MS (8), the stimulation intensities reported were much lower than applied in the current study. For example, in the two-week study of Szecsi et al. (8) the mean stimulation amplitudes used were 52 mA. We found that the intensity could be increased over the session as the sensory fibres desensitized to the repetitive electrical stimulation pulses. This allowed participants to tolerate stimulation amplitudes with a mean of 91 mA and 86 mA in the quadriceps and hamstrings. The conventional method used to control stimulation during NMES cycling (15) does not allow this because stimulation intensity is not independent of cycling cadence and has to be modulated rapidly to control the cycling speed.
In conclusion, the findings suggest that when NMES cycling exercise is appropriately adapted to persons with advanced MS it may be feasible and might bestow benefits. This method should also suit other populations with preserved sensation and muscle paralysis/paresis, for example those with cerebral palsy or incomplete SCI. The improvements in lower limb health suggested by the current findings need to be confirmed with further research. The current data shows that NMES could be a good exercise option for persons with advanced MS who often have very limited capacity for aerobic exercise. The current data shows that cardiorespiratory metabolism was accelerated slightly; it is possible that some of the participants could have achieved a greater aerobic workout with voluntary exercise. Further work is required to understand the relative benefits of voluntary and NMES exercise with respect to energy expenditure, cardiovascular response elicited, and the degree of disability due to MS. Well planned research could determine which disability sub-populations of MS might benefit from NMES exercise.
References

