Martin Heine, MSc1,2, Olaf Verschuren, PhD1,2 and Gert Kwakkel, PhD3,4
From the 1Brain Center Rudolf Magnus and 2Center of Excellence for Rehabilitation Medicine, University Medical Center Utrecht and Rehabilitation Center De Hoogstraat, Utrecht, 3Department of Rehabilitation Medicine, MOVE Research Institute Amsterdam, VU University Medical Center and 4Department of Neurorehabilitation, Centre of Rehabilitation and Rheumatology READE, Amsterdam, The Netherlands
OBJECTIVE: To examine the Oxygen Uptake Efficiency Slope (OUES) as an outcome for physical fitness in patients with multiple sclerosis.
DESIGN: Cross-sectional study.
Patients: A maximal cycling ergometry test was performed by 56 patients with multiple sclerosis.
METHODS: The OUES was compared with healthy reference values. Correlation analysis was used to assess the concurrent validity of the OUES and the following commonly used parameters of maximal exercise testing: maximal power output (Wmax) and peak oxygen consumption (VO2peak). The predictive validity of a submaximal OUES, derived using only 50% of the exercise duration (OUES50), and an OUES derived using the full exercise duration (OUES) were determined.
RESULTS: The OUES (mean 24.2 (standard deviation; SD 7.2)) was markedly lower than previously reported healthy reference values (mean 46.0 (SD 9.0)). Pearson correlation coefficients ranged from 0.514 (p < 0.01) between the OUES and Wmax and 0.857 for VO2peak (p < 0.01). The predictive validity of OUES50 for OUES was 0.918 (p < 0.01).
CONCLUSION: The moderate to high concurrent validity of the OUES with Wmax and VO2peak and high predictive validity of OUES50 for OUES suggest that maximal exercise testing in patients with low to moderate multiple sclerosis is not necessary.
Key words: multiple sclerosis; exercise testing; oxygen uptake efficiency slope; exercise tolerance; cardiopulmonary fitness.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Martin Heine, Brain Center Rudolf Magnus and Center of Excellence for Rehabilitation Medicine, University Medical Center Utrecht and Rehabilitation Center De Hoogstraat, Rembrandtkade 10, 3583 TM Utrecht, The Netherlands. E-mail: m.heine@dehoogstraat.nl
Accepted Feb 25, 2014, Epub ahead of print May 21, 2014
Introduction
Obtaining a valid measure of physical fitness in patients with multiple sclerosis (MS) is important for the purpose of monitoring physical fitness and evaluating the effect of interventions intended to improve physical fitness. Physical functioning is an important determinant of daily functioning in patients with MS (1). The current gold standard for the assessment of physical fitness is the maximal cardiopulmonary exercise test (CPET). Such tests are often accompanied by gas exchange measurement for direct assessment of peak oxygen uptake (VO2peak). The latter is considered a viable measure of physical fitness if the established criteria for maximal exercise are met: (i) a perceived exertion > 17 on the Borg Rating of Perceived Exertion (BORG) scale, (ii) a respiratory exchange ratio > 1.10, (iii) a heart rate within 90% of calculated maximal heart rate, and (iv) an oxygen consumption plateau is reached while the workload is still increasing (2). Patients with MS may be prevented from meeting these criteria by a variety of limiting symptoms of central (i.e. spasticity) and peripheral (i.e. reduced muscle strength) origin (3–6).
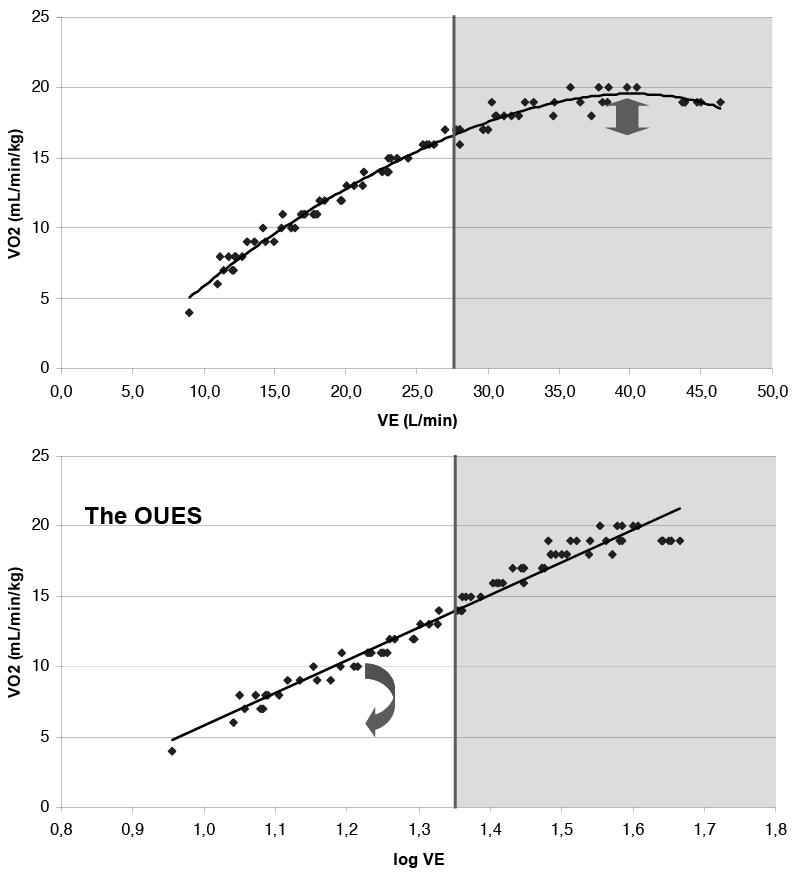
To develop an objective and independent submaximal measure of aerobic exercise capacity, Baba et al. (7) introduced the Oxygen Uptake Efficiency Slope (OUES) as an alternative physiological parameter based on the curve-linear relation between minute ventilation (VE) and oxygen consumption (VO2peak). Log-transformation of the VE yields a linear relation between log VE and VO2:
VO2 (ml/min/kg) = α × log VE (L/min) + β
The slope (α) in this equation is the OUES, a dimensionless measure of the efficiency of oxygen uptake with increasing VE (Fig. 1). A higher OUES means greater ventilatory efficiency. This measure has a few advantages over VO2peak. First, the calculation of the OUES is independent of test observer, incremental exercise protocol and patient effort, and is therefore suitable for patients who are not able or willing to attain maximal exercise values (8). Secondly, physiologically speaking, the OUES relies on the integration between cardiovascular, musculoskeletal, and respiratory functions (9), so it can be regarded as a single index of cardiorespiratory fitness that can be determined from submaximal exercise data (8). In healthy subjects, the OUES has a test-retest reliability similar to that of, e.g. VO2peak (intraclass correlation coefficient (ICC) = 0.890 vs ICC = 0.910) (10). The above properties make the OUES a possible alternative for VO2peak in patients with MS who are unable to attain maximal exercise, and may provide clinicians with a better estimate of cardiorespiratory fitness in these patients.
Unfortunately, the validity of the OUES has not yet been studied in patients with MS. The objective of the present study was 3-fold: (i) to determine the OUES of patients with MS and compare it with values previously reported for healthy persons; (ii) to assess the relation between the OUES and commonly used parameters of maximal exercise tolerance; and (iii) to study the predictive validity of the OUES based on submaximal exercise duration.
Methods
Participants
A cross-sectional sample of 56 participants of the “Treating fatigue in multiple sclerosis: aerobic training, cognitive behavioural therapy and energy conservation management” (TREFAMS-ACE) study (ISRCTN69520623) with definite MS (11) were included in the present study (12). The TREFAMS-ACE trial was approved by the medical ethics board of the VU University Medical Center Amsterdam. Each patient received both written and oral information about the purpose and risk of the TREFAMS-ACE trial before providing written informed consent. Patients were included if they experienced substantial fatigue (fatigue subscale of the checklist on individual strength > 35), were ambulant (Kurtzke’s Expanded Disability Status Scale (EDSS) ≤ 6.0) and had no clinical depression (depression subscale of the Hospital Anxiety and Depression Scale ≤ 11). Patients were excluded if they had been participating in a professionally guided exercise programme or any other programme to alleviate fatigue in the 3 months prior to inclusion. Patients were also excluded if they had comorbidities that precluded maximal exercise participation.
Descriptives
Prior to the cardiopulmonary exercise test, patient-reported baseline characteristics and disease specifics were recorded: sex, age, height, weight, body mass index (BMI), time since diagnosis, and type of MS (classified as relapsing remitting, primary progressive, secondary progressive, or unknown). Neurological disability was determined by certified neurologists using EDSS (13). The EDSS rating was determined prior to enrolment. Only patients with low to moderate disability defined as an EDSS ≤ 6.0 were included, implying that all patients in this study were able to walk at least 100 m using no more than one single-sided walking aid. EDSS scores were categorized as follows: EDSS ≤ 2.0 low disability; EDSS 2.5–4.0 mild disability; and EDSS ≥ 4.5 moderate disability.
Cardiopulmonary exercise testing
An incremental exercise test was performed on a programmable, electromagnetically braked cycle-ergometer (Kettler X7, Kettler, Germany) to determine maximal exercise capacity. The handlebars and saddle were adjusted to match each patient’s anthropometrics. Following a 3-min rest phase, patients started cycling at 25 Watt, with power output increased by 10 Watt (women) or 15 Watt (men) each min. This protocol was based on the rationale that small increments prolong exercise duration and enable patients with peripheral limitations to sustain a longer exercise duration. Ideally the exercise is terminated due to voluntary exhaustion following 8–12 min of exercise. During the exercise testing, patients were asked to maintain a cadence of 60–80 rotations/min (rpm). Patients were only vigorously encouraged beyond a respiratory exchange ratio > 1.00 by protocol. The exercise test was terminated by volitional exhaustion, a cadence <45 rpm or safety reasons, compliant with the American College of Sports Medicine’s guidelines for clinical exercise testing (2).
Gas exchange of each patient was measured using a portable mixing-chamber monitoring system (MetaMax 3B, Cortex Medical, Germany). Volume, pressure, and gas analysers were calibrated automatically by the system prior to each test using a 3 l syringe, pressure at the time (mmHg), and both ambient and reference gases (4.98% CO2, 17.05% O2), respectively. Raw data was averaged over 10-s intervals for analysis. VO2peak was defined as the highest recorded 10-s average during the final minutes of exercise. Heart rate was monitored using fingertip pulse oximetry. The following parameters derived from the CPET were used in the present study: VO2peak, maximal work rate (Wmax), maximal respiratory exchange ratio (RER), perceived exertion immediately following voluntary exhaustion, measured by the BORG scale (14), and measured maximal heart rate vs calculated maximal heart rate (%HRmax).
Oxygen uptake efficiency slope
CPET data was obtained for each completed step of the incremental exercise protocol. A linear regression equation was fitted onto the oxygen consumption, corrected for bodyweight and log-transformed minute ventilation. The slope of this regression line was the OUES. The accuracy of this regression line was determined using Pearson correlation coefficients. A second regression line was fit using the first 50% of the exercise duration (OUES50) only for those participants who reached a heart rate within 90% of the calculated maximal heart rate (%HRmax). This criterion was chosen because it is a physiological parameter that is easily obtained during CPET, compared with VO2 plateau or lactate. In case of an uneven number of data points, the number of data points was rounded downwards. We hypothesized that patients who showed a %HRmax > 90% exceeded the levels of submaximal exercise. Hence, only these subjects were used to calculate OUES50.
Statistical analysis
Baseline characteristics were described using descriptive statistics (means and standard deviation (SD)) and presented separately for each level of disability. Visual inspection of the outcomes and determinants used showed a normal distribution. Pearson’s correlation coefficients were used to assess the relationship between the OUES and patient characteristics and between the OUES and CPET outcomes. Pearson’s correlation coefficients were also used to test the predictive validity of the submaximal OUES50. One-way ANOVAs were used to test for mean differences between each of the disability groups, with Bonferroni post-hoc adjustment for multiple testing. Agreement between the OUES and OUES50 was assessed by the approach described by Bland & Altman (15). SPSS version 19.0 was used for statistical analyses. A 2-tailed p-value ≤ 0.05 was considered statistically significant in all tests.
Results
Fifty-six patients with definite MS participated in this study. Table I presents their descriptive statistics. The mean OUES was 24.2 (SD 7.2). Regarding the criteria for maximal exercise, 48.2% reached a maximal heart rate ≥ 90% of the calculated maximal heart rate, while 69.6% reached a respiratory exchange ratio > 1.10 and 23.3% had a BORG rating of perceived exertion > 17. The accuracy of the OUES (i.e. the linear regression line between log VE and VO2) showed a significant mean correlation coefficient of r = 0.942 (SD 0.048).
|
Table I. Descriptive statistics of the patients with multiple sclerosis, measuring the oxygen uptake efficiency slope |
||||
|
Patient characteristics |
All n = 56 |
Low n = 25 |
Mild n = 22 |
Moderate n = 9 |
|
Sex, men/women, n |
19/37 |
7/18 |
8/14 |
4/5 |
|
Type of multiple sclerosis, n |
||||
|
Relapsing remitting |
43 |
23 |
19 |
1 |
|
Primary progressive |
5 |
– |
2 |
3 |
|
Secondary progressive |
6 |
– |
1 |
5 |
|
Other/unknown |
2 |
2 |
– |
– |
|
Age, years, mean (SD) |
44.8 (10.6) |
40.9 (10.3) |
45.3 (9.3) |
54.6 (9.9)c |
|
BMI, mean (SD) |
24.8 (3.7) |
24.6 (3.3) |
25.0 (4.2) |
24.8 (3.9) |
|
Time to diagnosis, mean (SD) |
10.3 (7.2) |
8.5 (7.3) |
10.8 (7.3) |
14.4 (5.6) |
|
EDSS, mean (SD) |
2.8 (1.6) |
1.5 (0.6) |
3.1 (0.5)a |
5.7 (0.5)b,c |
|
CPET outcomes, mean (SD) |
||||
|
OUES |
24.2 (7.2) |
26.7 (6.2) |
23.2 (7.8) |
19.3 (5.5)c |
|
VO2peak |
21.4 (7.1) |
24.2 (6.1) |
20.8 (7.2) |
15.0 (5.4)c |
|
Wmax |
149.6 (54.6) |
160.6 (34.4) |
166.1 (55.7) |
78.3 (44.1)b,c |
|
%HRmax |
90.6 (10.9) |
94.9 (9.0) |
90.1 (10.1) |
80.7 (11.6)c |
|
RER |
1.18 (0.15) |
1.18 (0.15) |
1.20 (0.13) |
1.14 (0.21) |
|
BORG |
16.3 (1.8) |
16.2 (1.7) |
16.3 (1.8) |
16.6 (2.1) |
|
aLow vs mild; p < 0.05; bmild vs moderate; p < 0.05; clow vs moderate; p < 0.05. BMI: body mass index; EDSS: Expanded Disability Status Scale; OUES: oxygen uptake efficiency slope; VO2peak: peak oxygen consumption (ml·min·kg–1); Wmax: maximal power output (Watt); %HRmax: maximal heart rate relative to predicted heart rate (%); RER: respiratory exchange ratio; BORG: Borg Scale of Perceived Exertion; SD: standard deviation; EDSS: Kurtzke’s Expanded Disability Status Scale. |
||||
Concurrent validity of the OUES
Table II shows the correlation matrix of the patient characteristics and commonly used CPET outcomes with the OUES. Oxygen uptake efficiency (OUES) was significantly lower at higher BMI (r = –0.392, p < 0.01), age (r = –0.427, p < 0.01), level of disability (r = –0.476, p < 0.01) and RER (r = –0.274, p < 0.05). Regarding the commonly used outcomes of CPET, the OUES was higher in subjects with a higher Wmax (r = 0.514, p < 0.01) and higher VO2peak (r = 0.857, p < 0.01).
|
Table II. Pearson’s correlations of the oxygen uptake efficiency slope (OUES) with patient characteristics and cardiopulmonary exercise test (CPET) outcomes (n = 56) |
||||||||||
|
OUES |
BORG |
RER |
%HRmax |
Wmax |
VO2peak |
EDSS |
Time to diagnosis |
BMI |
Age |
|
|
Age |
–0.427** |
0.215 |
0.030 |
–0.280 |
–0.325* |
–0.564** |
0.472** |
0.488** |
0.065 |
1.000 |
|
BMI |
–0.392** |
0.002 |
0.025 |
–0.208 |
0.050 |
–0.269* |
–0.021 |
0.003 |
1.000 |
|
|
Time to diagnosis |
–0.119 |
0.123 |
–0.180 |
–0.109 |
–0.270* |
–0.211 |
–0.278* |
1.000 |
||
|
EDSS |
–0.476** |
0.093 |
–0.063 |
–0.454** |
–0.586** |
–0.583** |
1.000 |
|||
|
VO2peak |
0.857** |
–0.059 |
0.043 |
0.422** |
–0.684** |
1.000 |
||||
|
Wmax |
0.514** |
0.073 |
0.323* |
0.537** |
1.000 |
|||||
|
%HRmax |
0.251 |
0.213 |
0.405** |
1.000 |
||||||
|
RER |
–0.274* |
0.087 |
1.000 |
|||||||
|
BORG |
–0.130 |
1.000 |
||||||||
|
*p < 0.05; **p < 0.01; Significant correlations shown in bold. BMI: body mass index; EDSS: Expanded Disability Status Scale; OUES: oxygen uptake efficiency slope; VO2peak: peak oxygen consumption (ml × min × kg–1); Wmax: maximal power output (Watt); %HRmax: maximal heart rate relative to predicted heart rate (%); RER: respiratory exchange ratio; BORG: Borg Scale of Perceived Exertion. |
||||||||||
Predictive validity of the OUES50
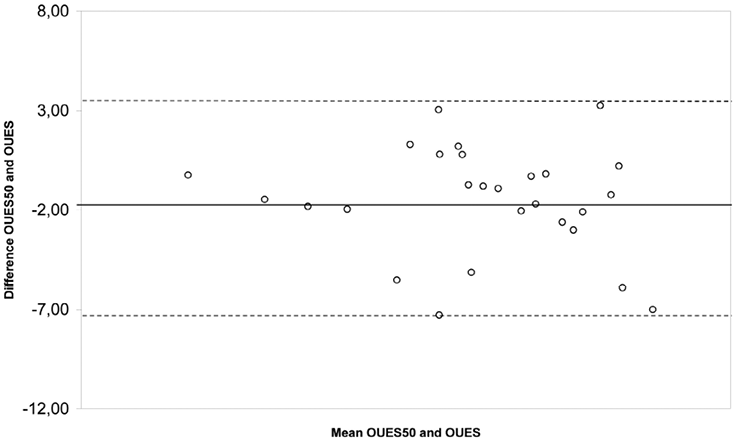
A total of 27 patients reached a heart rate greater than 90% of their age-predicted maximal heart rate. For these subjects, a submaximal OUES was calculated using only 50% of the exercise duration. The mean OUES50 was 23.6 ± 6.9 (n = 27). There was a significant correlation between OUES50 and OUES (r = 0.928; p < 0.01) A Bland-Altman analysis (Fig. 2) showed a mean difference of –1.8 (95% CI –7.1 to 3.5) between OUES50 and OUES.
Discussion
This study was designed to assess the concurrent validity of the OUES with commonly used outcomes of cardiopulmonary exercise testing (i.e. Wmax and VO2peak) in patients with low to moderate MS. In addition, we tested the predictive validity of a submaximal OUES derived using only 50% of the exercise duration (OUES50) vs that of an OUES derived using the complete exercise duration. The OUES values we found were markedly lower than those previously reported for healthy persons, even for patients with minimal disability due to MS (10). The present study shows that a higher OUES is moderately to highly associated with higher levels of peak oxygen consumption (VO2peak) and a higher power output. The results also showed, in a subset of patients, that OUES50 is highly correlated with the OUES when derived from full exercise duration, which explained 84% of the variance of outcome. These findings show that the OUES correlates well with commonly used CPET outcomes and can be determined by using submaximal exercise testing in MS. The proposed generic properties of the OUES, i.e. being independent of test observer, test protocol and patient effort, make it a promising parameter of physical fitness in patients with MS, which can be more easily compared with other reference populations and between different studies (8, 9).
The mean OUES in our sample (24.2 (SD 7.2)) was considerably lower than that found for healthy (46.0 (SD 9.0)) (10) and overweight adolescents (45.1 (SD 8.7)) (16). It should be noted that the members of the healthy reference group (10) were younger (mean age 28 years (SD 6)) and had a lower mean body mass index (BMI) (22.1 kg/m2 (SD 1.9)) than our sample. The mean OUES we found for patients with MS is comparable to that for patients with chronic obstructive pulmonary disorder (30.0 (SD 7.7)) (17) or heart failure (19.0 (SD 5.2)) (18–20). As stated above, the OUES relies on the combined action of cardiovascular, musculoskeletal, and respiratory functions (9). Due to the inter- and intra-individual variety in demyelination, each of these components may be substantially reduced in patients with MS. For example, as regards cardiovascular function, Saari et al. (4) showed that, compared with healthy controls, patients with MS demonstrated reduced heart rate variation and decreased blood pressure reactions, indicating disturbed cardiovascular regulation. As regards muscle function, Ng et al. (5) demonstrated that maximum voluntary muscle contraction was significantly lower than in healthy controls (–27%), while muscle cross-sectional area was similar. These findings suggest that the reduced muscle strength could be attributable mainly to an impaired temporal-spatial activation of muscles by the central nervous system. In addition, it has also been suggested that muscles of patients with MS may have reduced oxidative capacity (21, 22). Intervention studies have shown that the reduced muscle strength can, at least partly, be regained, and that this may lead to improved functioning (23) and also may restore the oxidative capacity of the working muscle. As regards respiratory function, Bosnuk-Guclu et al. (3) demonstrated that patients with MS have considerable respiratory muscle weakness and that this is related to functional exercise capacity. These are some, but not all, of the mechanisms that may reduce the OUES in patients with MS.
We showed that the OUES significantly related to VO2peak (r = 0.857, p < 0.01). These results indicate that the OUES can be considered a measure of cardiorespiratory fitness. Other studies in different populations have found similar correlations between OUES and VO2peak. For instance, in their original introduction of the OUES, Baba et al. (7) found a similar strong correlation between OUES and VO2peak in patients with heart failure (r = 0.871, p < 0.01) (7). A similar correlation was found for overweight adolescents (r = 0.774, p < 0.01) (16).
Compared with VO2peak, we found that the OUES can also be measured using only 50% of the exercise duration (i.e. submaximal). Others studies have used different exercise durations, for example 70% (10) or at RER = 1.00 (18, 24). These studies also confirmed the predictive validity of a submaximal OUES (10, 16–18, 24). The above findings make the OUES a promising, direct (i.e. not predicted) measure of physical fitness that does not require maximal exercise. In addition, we found that the OUES50 slightly underestimated the OUES, which is in line with other studies using limited exercise duration (24). The minor underestimation of OUES by the OUES50 also suggests, for clinical practice, that the maximal OUES is preferred in those cases when the criteria for maximal exercise testing are applicable.
From the field of sports medicine other submaximal physiological outcomes can be considered in patients with MS. For instance, gas exchange thresholds, such as the anaerobic or ventilatory threshold, the critical power or oxygen kinetics during exercise. We are aware of one intervention study that used the aerobic threshold as an outcome to study the effect of exercise therapy in patients with MS (25). They found that, following a brief moderate exercise programme, the aerobic threshold shifted rightwards, indicating an increase in aerobic capacity. To our knowledge the critical power has not been studied in patients with MS. As regards the oxygen kinetics, we are aware of one study that assessed these in patients with MS. Hansen et al. (21) looked at the oxygen uptake kinetics during exercise onset and offset. They found significantly slower onset kinetics in patients with MS compared with healthy controls suggestive of reduced oxidative capacity of muscles in patients with MS. This may also, in part, explain the increased cost of walking in patients with MS (26, 27). Walking tests are often used in patients with MS, since they are easy to administer and walking capacity is of great clinical relevance. However, we feel that, unless an additional outcome of fitness is derived during the walking test, the achieved distance solely cannot be considered an index for physical fitness. In addition, the cost of walking may only be a measure of fitness if the walking pattern is more or less identical to the reference sample. If not, the cost of walking is a measure of walking capacity rather than physical fitness.
This study had some limitations. First, a large proportion of the included sample had been recruited at baseline for an exercise-related intervention trial. These selected patients had given their informed consent to participate and may have had a predisposition to engage in exercise and so be less representative of patients with MS in general. Secondly, the participants in this study had no previous experience in maximal exercise testing. This may have introduced some reservations to truly deliver a maximal exercise effort. Thirdly, being participants of the TREFAM-ACE trial, these patients also experienced substantial levels of fatigue. The OUES may be different in patients without fatigue, especially since fatigue is considered one of the most frequent and disabling symptoms (28). Fourthly, we subjectively chose %HRmax as a criterion to calculate a submaximal OUES. This was based on the hypothesis that, compared with the RER and BORG scale, the achieved maximal heart rate would be more susceptible to the level of neurological disability. Using different criteria (e.g. BORG scale or RER) might change the predictive validity of OUES50. Finally, the current study did not allow us to examine the reliability of the OUES in patients with MS. Further research is required to establish the cross-validity of submaximal OUES in an independent sample.
Based on the findings of this study and taking its limitations into account, we can conclude that the oxygen uptake efficiency slope is a promising fitness parameter for patients with MS. It can be established, using submaximal exercise duration, thereby increasing its suitability for patients with MS and decreasing the burden of maximal exercise testing. However, it does not take away the need for gas-exchange measurements. Since the latter requires special equipment and staff training, this reduces its feasibility in clinical practice.
Unfortunately, the body of knowledge regarding the OUES and other submaximal fitness outcomes in patients with MS is small. Further research is needed to improve our understanding of the OUES values found in these patients and its relation to clinically relevant measures of body function (or dysfunction), activity, and participation, as well as its sensitivity to change. Other submaximal exercise outcomes should be studied to improve our understanding of the (submaximal) exercise physiology specific for patients with MS and how these outcomes may be used in clinical practice.
Acknowledgements
The authors would like to thank the staff at the St Antonius Hospital Multiple Sclerosis Center, Nieuwegein and Erasmus Medical Center, Rotterdam for their efforts in finding eligible subjects for the present study. In addition, the authors would like to thank the TREFAMS-ACE study group for their respective role in the TREFAMS-ACE trial.
The TREFAMS-ACE study is funded by the Fonds NutsOhra (ZonMw 89000005).
The authors declare no conflicts of interest.
References

