Sanam Pourhabib, MSc1, Amanda C. Kentner, PhD2 and Sherry L. Grace, PhD1, 3
From the 1York University, 2MCPHS University and 3University Health Network, Toronto, Canada
OBJECTIVE: Secondary prevention programs such as cardiovascular rehabilitation significantly decrease the burden of cardiovascular disease, yet are under-used. The most successful strategy to promote cardiovascular rehabilitation utilization is systematic referral with a patient-provider discussion. This study investigated: (i) the elements of patient-provider discussions related to patient cardiovascular rehabilitation enrollment, and (ii) the frequency and correlates of these discussion elements.
Design/PARTICIPANTS: This was a prospective study of cardiovascular patients and their healthcare providers. Discussions about “secondary prevention” were audio-recorded. Utterances were coded using the Roter Interaction Analysis System. Two months later, cardiovascular rehabilitation enrollment was ascertained.
RESULTS: Discussions between 26 healthcare providers and 50 patients were recorded, of whom 27 (54.0%) enrolled in cardiovascular rehabilitation. Participants were significantly more likely to enroll in cardiovascular rehabilitation when their healthcare providers offered less reassurance and optimism (odds ratio (OR) = 0.81), and when the patient asked more questions related to lifestyle (OR = 4.98). These were not common.
CONCLUSION: While caution is warranted due to the number of comparisons undertaken such that associations observed may be chance associations, these novel findings suggest that not overstating the beneficial effects of acute treatment, and allowing patients more time to ask questions about needed lifestyle changes should be investigated in future research.
Key words: health communication; cardiovascular disease; rehabilitation; patient-centered care.
J Rehabil Med 2014; 46: 00–00
Correspondence address: Dr. Sherry L. Grace, PhD, York University, 368 Norman Bethune, 4700 Keele Street, Toronto, ON, Canada M3J 1P3. E-mail: sgrace@yorku.ca
Accepted Apr 17, 2014; Epub ahead of print Aug 6, 2014
Introduction
Cardiovascular disease, including coronary artery disease (CAD) and stroke, are among the leading causes of morbidity and mortality globally (1). CAD and transient ischemic attack or mild, non-disabling stroke have similar atherosclerotic etiology and modifiable risk factors. As such, similar to secondary prevention for CAD, recurrent vascular events in stroke patients can be prevented with an exercise-based, lifestyle intervention in combination with medication therapies (2, 3).
Comprehensive chronic disease management programs, such as cardiovascular rehabilitation (CR), play an integral role in augmenting recovery. CR involves structured exercise training, education, risk factor reduction and behavior change counseling. Participation in CR programs have been shown to reduce mortality by about 25%–30% and to have favorable effects on re-hospitalization rates, functional capacity, and quality of life (4, 5). Emerging evidence supports the feasibility, safety and benefits of CR for transient ischemic attack/mild non-disabling stroke patients as well (2, 6, 7).
However, despite the evidence of CR benefit (8) and clinical guideline recommendations to refer patients (9), only 15–30% of CAD patients access CR (10). One of the most consistent factors shown to affect patient utilization is healthcare provider (HCP) encouragement or endorsement of CR (11, 12). However, to date, the verbal and non-verbal aspects of patient-HCP discussions regarding CR have not been characterized, and thus it is unknown how the nature of these discussions may influence patient enrollment. Accordingly, the objectives of this study were to: (i) investigate the elements of patient-provider discussions related to patient CR enrollment, and (ii) the frequency and correlates of these discussion elements.
Methods
Design and procedure
This was an observational, prospective study of cardiovascular patients and their HCPs recruited between September 2011 to November 2012 from 3 hospitals (two academic), in Southern Ontario. Ethics approval was granted by all participating organizations’ research ethics boards. A diagram depicting study flow is shown in Fig. 1.
All HCPs on the cardiovascular units and at the Stroke Prevention Clinic were approached via email and in-services to solicit informed consent to participate. Upon HCP consent, cardiovascular patients were approached to participate in the study on the days the HCP was working, until an interaction was audio-recorded. Willing HCPs and/or patients were asked to carry a numbered digital recorder throughout the day, and to turn it on and off at the beginning and end of their interaction, respectively. For those patients undergoing intervention, discussions were only recorded post-procedure.
After the patient-HCP dialogue had been recorded, patients were asked to complete a self-report survey. It assessed sociodemographic characteristics, as well as their CR awareness and intentions to enroll. Clinical characteristics were extracted from patient charts. The participating HCPs were similarly asked to complete a self-report survey, assessing their work characteristics, CR referral practices and awareness.
All audio-recordings of the HCP-patient discussions were anonymized. These were then emailed through a secure file portal for external coding based on the Roter Interaction Analysis System (RIAS) (13, 14). RIAS is a standardized method of coding medical dialogue. One RIAS coder categorized interactions according to the 41 standard RIAS categories (described below). A second RIAS coder audited the coding trail on a random subset of audio-recordings, to ensure data quality and to establish the RIAS’ reliability in this setting. Finally, CR charts were audited at the institutional programs two months later to ascertain CR enrollment.
Participants
Participants and HCPs were approached on the cardiovascular units and at the Stroke Prevention Clinic to participate. HCP participants included those working on the cardiac inpatient units, including surgical and interventional wards, as well as the outpatient Stroke Prevention Clinic. This included physicians, nurse-practitioners, nurses, and allied healthcare professionals (e.g., physiotherapists). In addition, peer mentors from the surgical ward who were registered with volunteer services were approached. While only physicians can sign-off on CR referrals in Ontario, it is generally nurses or allied health professionals who discuss CR with patients and draft CR referral forms for physician signature (15). The exclusion criterion was that the HCPs were not involved in direct patient care (i.e., nurse managers).
Patient inclusion criteria were: age ≥ 18, and having a clinical indication for CR based on practice guidelines (e.g., acute coronary syndrome, post-procedure such as percutaneous coronary intervention or coronary artery bypass grafting surgery) (16). In the case of stroke patients, those with transient ischemic attacks and mild non-disabling strokes were eligible. Exclusion criteria were: (i) patients who were not eligible for CR due to comorbid musculoskeletal, neuromuscular, visual, cognitive or non-dysphoric psychiatric conditions (i.e., schizophrenia, advanced dementia), (ii) being discharged to long-term care, (iii) any serious or terminal illness not otherwise specified which would preclude CR participation (16), and (iv) limited English-language proficiency. In addition, stroke patients who were unable to ambulate, and hence participate fully in CR, were excluded.
Measures
Healthcare providers characteristics. HCPs were asked to report their profession, highest degree obtained, year they graduated from their most advanced degree, sex, and estimated average number of patients they treat daily.
Patient sociodemographic and clinical characteristics. On the survey, patients were asked to report their age, sex, marital status, racial/ethnic background, work status, and highest level of education. The survey also included the MacArthur Scale of Subjective Socioeconomic Status (SES) (17), where participants were asked to demarcate their perceived status compared to others in Canada, on an arbitrary scale. This scale is presented as a ladder where each rung represents a socioeconomic level, the scores ranging from 1 to 10, with higher scores indicating greater subjective SES. A median split was computed, to categorize participants as high versus low subjective SES.
With regard to clinical characteristics, the survey also included the Duke Activity Status Index (18), a brief 12-item self-administered survey used to determine functional capacity (19). Finally, clinical variables abstracted from patient medical charts included: index cardiovascular condition, risk factors, and previous history of cardiovascular disease.
Healthcare providers and patient awareness of cardiovascular rehabilitation. The HCP survey assessed the percentage of patients they refer (0–100%), and their CR awareness. The patient report survey also assessed their awareness of CR and intentions to enroll into a CR program. These latter variables were assessed on a 5-point Likert scale, with greater scores indicating higher awareness/intentions.
Interaction analysis. To quantify the dialogue between HCPs and their patients, audio-recordings were analyzed by RIAS-trained coders externally. RIAS is a standardized method of coding medical dialogue. It has been validated in several countries and healthcare settings (16) including in cardiac surgery patients (20). The RIAS has been shown to be both reliable and valid (16).
The unit of analysis was an utterance, defined as the smallest discriminable speech segment to which a coder could assign a classification, and which expressed or implied a complete thought. This could vary from a single word, to a phrase, or a complete sentence. The broad categories are: data gathering, patient education and counseling, facilitation and patient activation, rapport-building and procedural utterances.
Finally, RIAS coders rated the global affect (i.e., the tonal qualities of the interaction) of each audio-recording. This transmits the emotional context of the audio-recording beyond the significance of the words spoken. Coders rated anger, anxiety, dominance, interest, friendliness, and interactivity for example, on a 5-point Likert scale from “low” to “high”.
Dependent variable. CR charts were audited at the institutions’ programs, to ascertain whether enrollment into the program was made or not (yes/no). Where a patient did not enroll, patients were telephoned at home to ascertain whether they had been enrolled to another CR program.
Statistical analyses
SPSS version 20.0 was used for all analyses. Since the assumption of homogeneity of variance could not be assumed, non-parametric tests were applied. An initial descriptive analysis of HCP and patient characteristics was performed.
To test the first objective, a descriptive examination of the RIAS coding categories was performed and the CR enrollment rate was described. Next, patient sociodemographic and clinical characteristics as well as RIAS codes were compared by CR enrollment, using Mann-Whitney U and chi-square tests as appropriate. Then, binary logistic regression analysis was used to examine the association of the patient characteristics and RIAS codes identified as significantly related with CR enrollment (dependent variable) through the previous analysis.
To test the second objective, the frequency of the RIAS codes significantly related to CR enrollment was described. Finally, patient sociodemographic and clinical characteristics were compared by the RIAS utterances shown to be related to CR enrollment, using Mann-Whitney U and Spearman correlations, as appropriate.
Results
Respondent characteristics
A diagram of study flow is shown in Fig. 1. Of the 101 HCPs approached, 60 consented to participate in the study (59.4% response rate). Of these, valid audio-recordings were obtained with 26 (43.3%) HCPs. Their sociodemographic and work-related characteristics are summarized in Table I. The primary healthcare professional audio-recorded was nurses (n = 13, 50.0%). Other professions represented in the sample were: nurse-practitioners (n = 5, 19.2%), cardiologists (n = 2, 7.7%), physiotherapists (n = 2, 7.7%), peer mentors (n = 2, 7.7%), a dietitian (n = 1, 3.8%), and a pharmacist (n = 1, 3.8%).
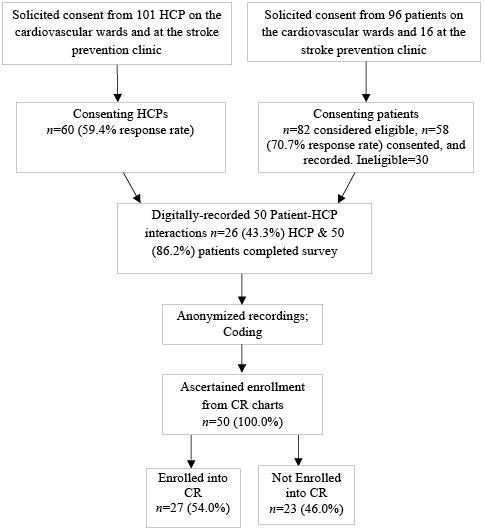
Fig. 1. Study Flow Diagram. CR: cardiovascular rehabilitation; HCP: healthcare provider.
|
Table I. Participating healthcare provider characteristics and perceptions related to patient cardiovascular rehabilitation (CR) enrollment (n = 50) |
|||
|
Patient CR enrollment |
p-value |
||
|
Yes n = 27 (54%) |
No n = 23 (46%) |
||
|
Sex, female, n (%) |
6 (66.7) |
13 (76.5) |
0.59 |
|
Highest degree obtained, undergraduate degree, n (%) |
3 (33.3) |
12 (70.6) |
0.07 |
|
Year obtained highest academic qualification, year (SD) |
1994 (14) |
1990 (16) |
0.55 |
|
Profession, nurse, n (%) |
4 (44.4) |
9 (52.9) |
0.68 |
|
Estimated number of patients seen/day, mean (SD) |
6.11 (1.69) |
9.29 (6.46) |
0.55 |
|
% of eligible patients referred or recommended to CR by HCP, mean (SD) |
78.89 (31.40) |
77.20 (29.00) |
0.98 |
|
CR awareness, mean (SD)a |
4.33 (0.71) |
3.76 (0.75) |
0.07 |
|
aCR awareness was evaluated on a 5-point Likert scale. HCP: healthcare provider; SD: standard deviation. |
|||
Of the 112 patients who were approached, 82 were considered eligible for our study, of whom 58 (70.7% response rate) consented, and were recorded. Twenty-four (21.4%) patients declined to participate, and 30 (26.8%) were considered ineligible, for the following reasons: insufficient English-language proficiency (n = 21, 70.0%), imminent discharge (n = 3, 10.0%), patient already referred to CR (n = 2, 6.7%), vision problems (n = 2, 6.7%), and patient not cognitively-oriented to time and place (n = 2, 6.7%). Of the participating patients, for two (6.7%) the tape quality was insufficient for coding both speakers, two (6.7%) patient’s HCP changed, two (6.7%) patients were transferred to another hospital, and two (6.7%) patients did not have an interaction with a consenting HCP before discharge, and thus these 8 patients were subsequently excluded. The resultant sample size is 50 patients. Their sociodemographic and clinical characteristics are summarized in Table II.
|
Table II. Sociodemographic and clinical characteristics of patients |
||||
|
Characteristics |
Patient CR enrollment |
|||
|
Total n = 50 |
Yes n = 27 (54%) |
No n = 23 (46%) |
p-valuea |
|
|
Sociodemographic |
||||
|
Age, years, mean (SD) |
65.48 (12.95) |
65.59 (10.35) |
65.35 (15.71) |
0.82 |
|
Sex, female, n (%) |
14 (28.0) |
7 (25.9) |
7 (30.4) |
0.72 |
|
Marital status, married, n (%) |
33 (66.0) |
19 (70.4) |
14 (60.9) |
0.48 |
|
Ethnicity, white/Caucasian, n (%) |
27 (54.0) |
15 (55.6) |
12 (52.2) |
0.81 |
|
Work status, retired, n (%) |
35 (70.0) |
18 (66.7) |
17 (73.9) |
0.58 |
|
Education, post-secondary, n (%) |
17 (34.0) |
8 (29.6) |
9 (39.1) |
0.48 |
|
Subjective SES, mean (SD) |
6.55 (1.31) |
6.77 (1.37) |
6.30 (1.22) |
0.06 |
|
Clinical |
|
|
|
|
|
Cardiac indication, n (%) |
||||
|
PCI, yes, n (%) |
23 (46.0) |
12 (44.4) |
11 (47.8) |
0.81 |
|
Stroke, yes, n (%) |
8 (19.5) |
5 (23.8) |
3 (15.0) |
0.48 |
|
HF, yes, n (%) |
7 (14.0) |
4 (14.8) |
3 (13.0) |
0.86 |
|
MI, yes, n (%) |
4 (8.2) |
2 (7.7) |
2 (8.7) |
0.90 |
|
BMI, mean (SD) |
27.36 (5.35) |
27.71 (5.37) |
26.96 (5.41) |
0.44 |
|
Previous CAD, yes, n (%) |
24 (48.0) |
13 (48.1) |
11 (47.8) |
0.98 |
|
Diabetes, yes, n (%) |
15 (30.6) |
8 (30.8) |
7 (30.4) |
0.98 |
|
HTN/HTN medication, yes, n (%) |
33 (66.0) |
21 (77.8) |
12 (52.2) |
0.06 |
|
Dyslipidemia/Lipid-lowering medication, yes, n (%) |
32 (64.0) |
19 (70.4) |
13 (56.5) |
0.31 |
|
DASI, mean (SD) |
29.58 (15.56) |
28.92 (16.33) |
30.36 (14.92) |
0.82 |
|
CR |
|
|
|
|
|
Intention to enrol, mean (SD) |
3.49 (1.44) |
3.84 (1.18) |
3.09 (1.63) |
0.15 |
|
CR awareness, mean (SD) |
3.22 (1.34) |
3.35 (1.16) |
3.09 (1.53) |
0.57 |
|
aChi-square test for categorical variables and Mann-Whitney U were performed for continuous variables by CR enrollment. BMI: body mass index; CAD: coronary artery disease; CR: cardiovascular rehabilitation; DASI: Duke Activity Status Index; HCP: healthcare provider; HF: heart failure; HTN: hypertension; MI: myocardial infarction; PCI: Percutaneous Coronary Intervention; SD: standard deviation; SES: socioeconomic status. |
||||
Patient-healthcare provider discussions
Of the 50 recorded discussions, there were 12 (46.2%) HCPs recorded once, 7 (26.9%) recorded twice (i.e., with 2 different patients), 4 (15.4%) recorded 3 times, 3.8% from one HCP recorded 4 times, and one (3.8%) HCP recorded 6 and another 7 times. The mean discussions were 8.93 min in length (standard deviation 8.84), and length was unrelated to patient enrollment (p = 0.76).
Overall, CR was mentioned in 41 (82.0%) discussions, during which the HCP raised the conversation about CR and encouraged patient participation. CR referral was discussed in 35 (70.0%) recordings. Twenty-nine (58.0%) of the discussions regarding CR were 2-way discussions.
Table III displays the median frequency (interquartile range) and global affect ratings of each RIAS-coded element of the discussions. A second RIAS coder audited the coding trail on a random subset (n = 7 cases) of audio-recordings, to ensure data quality and to establish the RIAS’ reliability in the CR setting. The mean inter-rater reliability was 0.90 for HCP talk and 0.92 for patient talk. Reliability of global affect ratings was reported at 100% agreement (within one-point on the rating scale).
Cardiovascular rehabilitation enrollment
Of the 35 (70.0%) patients referred to CR, 27 (54.0%) ultimately enrolled. To test the first objective, differences in CR enrollment rates were explored. HCP sociodemographic and work-related characteristics were unrelated to CR enrollment (Table I). However, there was a trend towards greater enrollment where HCPs were more educated and had greater CR awareness (i.e., 0.05 < p > 0.10). With regard to patient characteristics, there were no significant differences in sociodemographic or clinical characteristics between patients who enrolled and those who did not (Table II). However, there were trends toward greater CR enrollment among patients with higher subjective SES and those who had hypertension.
Based on the RIAS codes, some elements of the discussions were also related to CR enrollment (Table III). There was greater CR enrollment where HCPs provided less reassurance and optimism to patients, and where patients asked more questions regarding their lifestyle.
The logistic regression model testing the effects of these variables in relation to CR referral is presented in Table IV. The logistic regression model was significant overall (χ2(4) = 19.28, p = 0.001), and accounted for 43.4% of the variance in enrollment (Nagelkerke R2). As shown, the odds of CR enrollment were almost 5 times greater when patients discussed and asked questions related to lifestyle, and 19% lower when their HCP offered greater reassurance and optimism.
With regard to the second objective, the median frequency of these significant RIAS-coded utterances in each discussion is shown in Table III. These utterances were not common in the CR discussions recorded. Greater HCP reassurance and optimism during the discussion was related to greater patient socioeconomic status, lower patient body mass index and not having hypertension. No correlates of patients asking more lifestyle questions were identified.
|
Table III. Median frequency (interquartile range) of RIAS-coded utterances and global affect ratingsa per discussion by cardiovascular rehabilitation (CR) enrollment, descending order |
||||
|
Code |
Total n = 50 Median (IQR) |
Patient CR enrollment |
p-value |
|
|
Enrolled in CR n = 27 (54%) Median (IQR) |
Not enrolled in CR n = 23 (46%) Median (IQR) |
|||
|
HCP: Gives information – therapeutic |
26 (12–50) |
34 (20–58) |
20 (8.0–46) |
0.12 |
|
Pt: Shows agreement, understanding |
22 (11–46) |
29 (11–50) |
18 (9.0–41) |
0.34 |
|
HCP: Counsels – medical/therapeutic |
6.0 (1.0–18) |
7.0 (1.0–14) |
4.0 (1.0–19) |
0.71 |
|
HCP: Shows agreement, understanding |
8.5 (4.8–13) |
9.0 (5.0–13) |
7.0 (4.0–13) |
0.64 |
|
Pt: Gives information – lifestyle |
4.5 (1.8–15) |
4.0 (1.0–13) |
7.0 (2.0–22) |
0.15 |
|
HCP: Back-channels |
8.5 (3.0–14) |
7.0 (2.0–12) |
10.0 (3.0–17) |
0.11 |
|
Pt: Gives information – medical |
5.0 (0.8–11) |
4.0 (0.0–8.0) |
7.0 (1.0–12) |
0.24 |
|
Pt: Gives information – therapeutic |
6.0 (2.0–11) |
6.0 (2.0–8.0) |
7.0 (3.0–12) |
0.29 |
|
HCP: Counsels – lifestyle/psychosocial |
2.5 (0.0–5.0) |
2.0 (0.0–8.0) |
3.0 (0.0–4.0) |
0.98 |
|
HCP: Paraphrase, checks for understanding |
3.0 (1.0–10) |
3.0 (1.0–8.0) |
4.0 (2.0–14) |
0.17 |
|
HCP: Gives information – medical |
1.5 (0.0–9.3) |
2.0 (0.0–9.0) |
1.0 (0.0–10) |
0.93 |
|
HCP: Gives information – lifestyle |
3.0 (0.0–8.3) |
5.0 (1.0–10) |
2.0 (0.0–6.0) |
0.17 |
|
HCP: Reassures, optimism |
3.0 (1.0–7.0) |
2.0 (1.0–4.0) |
5.0 (2.0–9.0) |
0.02 |
|
HCP: Gives orientation, instructions |
1.5 (1.0–6.0) |
1.0 (1.0–6.0) |
3.0 (1.0–6.0) |
0.33 |
|
HCP: Interest/attentiveness |
5.0 (4.0–5.0) |
5.0 (4.0–5.0) |
5.0 (4.0–5.0) |
0.64 |
|
HCP: Asks for understanding |
2.0 (1.0–5.0) |
2.0 (1.0–4.0) |
2.0 (0.0–6.0) |
0.36 |
|
Pt: Interest/attentiveness |
4.0 (4.0–5.0) |
4.0 (4.0–5.0) |
5.0 (4.0–5.0) |
0.70 |
|
Pt: Paraphrase, checks for understanding |
2.0 (0.8–5.0) |
2.0 (0.0–5.0) |
2.0 (1.0–6.0) |
0.80 |
|
HCP: Friendliness/warmth |
4.0 (3.0–4.0) |
4.0 (3.0–4.0) |
4.0 (3.0–4.0) |
0.41 |
|
HCP: Interactivity |
4.0 (3.0–4.3) |
4.0 (3.0–5.0) |
3.0 (3.0–4.0) |
0.30 |
|
Pt: Friendliness/warmth |
4.0 (3.0–4.0) |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
0.15 |
|
HCP: Responsiveness/engagement |
3.5 (3.0–4.0) |
4.0 (3.0–5.0) |
3.0 (3.0–4.0) |
0.54 |
|
HCP: Sympathetic/empathetic |
4.0 (3.0–4.0) |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
0.33 |
|
Pt: All questions – therapeutic |
2.0 (1.0–4.3) |
2.0 (1.0–6.0) |
2.0 (1.0–3.0) |
0.46 |
|
HCP: Dominance/assertiveness |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
3.0 (3.0–4.0) |
0.31 |
|
Pt: Interactivity |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
3.0 (3.0–4.0) |
0.75 |
|
Pt: Responsiveness/engagement |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
3.0 (3.0–4.0) |
0.88 |

|
Table III. Contd. |
||||
|
Code |
Total n = 50 |
Patient CR enrollment |
p-value |
|
|
Enrolled in CR n = 27 (54%) |
Not Enrolled in CR n = 23 (46%) |
|||
|
HCP: Hurried/rushed |
3.0 (3.0–4.3) |
4.0 (3.0–4.0) |
3.0 (3.0–5.0) |
0.86 |
|
Pt: Dominance/assertiveness |
3.0 (3.0–4.0) |
4.0 (3.0–4.0) |
3.0 (3.0–3.0) |
0.87 |
|
HCP: Concern, worry |
1.0 (0.0–3.0) |
1.0 (0.0–3.0) |
1.0 (0.0–2.0) |
0.94 |
|
Pt: Reassures, optimism |
3.0 (1.0–4.3) |
2.0 (1.0–4.0) |
3.0 (1.0–6.0) |
0.09 |
|
HCP: Respectfulness |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
0.36 |
|
Pt: Respectfulness |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
0.32 |
|
Pt: Sympathetic/empathetic |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
3.0 (3.0–3.0) |
0.36 |
|
HCP: Approval – direct |
2.0 (0.8–4.0) |
1.0 (0.0–3.0) |
3.0 (1.0–5.0) |
0.25 |
|
Pt: Laughs, tell jokes |
1.0 (0.0–3.3) |
1.0 (0.0–3.0) |
1.0 (0.0–4.0) |
0.85 |
|
HCP: Closed question – medical |
0.50 (0.0–3.0) |
0.0 (0.0–2.0) |
2.0 (0.0–5.0) |
0.26 |
|
HCP: Gives information – psychosocial |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.64 |
|
HCP: Closed question – lifestyle |
1.0 (0.0–2.0) |
1.0 (0.0–3.0) |
1.0 (0.0–2.0) |
0.82 |
|
HCP: Transitions |
1.0 (0.0–3.0) |
2.0 (0.0–3.0) |
1.0 (0.0–2.0) |
0.37 |
|
HCP: Closed question – therapeutic |
1.0 (0.0–2.3) |
1.0 (0.0–2.0) |
1.0 (0.0–3.0) |
0.48 |
|
Pt: Approval- direct |
1.0 (0.0–3.0) |
1.0 (0.0–3.0) |
1.0 (0.0–3.0) |
0.62 |
|
Pt: Unintelligible utterance |
1.0 (0.0–2.3) |
1.0 (0.0–2.0) |
2.0 (0.0–3.0) |
0.08 |
|
Pt: Gives information – psychosocial |
0.50 (0.0–2.0) |
0.0 (0.0–1.0) |
1.0 (0.0–3.0) |
0.36 |
|
Pt: Concern, worry |
1.0 (0.0–3.0) |
0.0 (0.0–3.0) |
1.0 (0.0–4.0) |
0.19 |
|
HCP: Laughs, tells jokes |
1.0 (0.0–2.3) |
1.0 (0.0–2.0) |
1.0 (1.0–3.0) |
0.07 |
|
HCP: Personal remarks |
0.0 (0.0–3.0) |
0.0 (0.0–2.0) |
0.0 (0.0–3.0) |
0.43 |
|
HCP: Asks for opinion |
1.0 (0.0–2.3) |
1.0 (0.0–3.0) |
1.0 (0.0–2.0) |
0.76 |
|
Pt: Anxiety/nervousness |
1.0 (1.0–2.0) |
1.0 (1.0–2.0) |
1.0 (1.0–2.0) |
0.52 |
|
Pt: Personal remarks |
0.0 (0.0–2.0) |
0.0 (0.0–2.0) |
0.0 (0.0–2.0) |
0.45 |
|
Patient: Anger/irritation |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
0.36 |
|
HCP: Anxiety/nervousness |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.00 |
|
HCP: Anger/irritation |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.00 |
|
Pt: Emotional distress/upset |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.00 |
|
Pt: Depression/sadness |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.0 (1.0–1.0) |
1.00 |
|
Pt: Transitions |
0.50 (0.0–1.0) |
0.0 (0.0–1.0) |
1.0 (0.0–1.0) |
0.25 |
|
HCP: Gives information – other |
0.0 (0.0–1.0) |
0.0 (0.0–0.0) |
0.0 (0.0–1.0) |
0.28 |
|
HCP: Open question – medical |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.46 |
|
Pt: All questions – lifestyle |
0.0 (0.0–1.0) |
1.0 (0.0–2.0) |
0.0 (0.0–1.0) |
0.03 |
|
Pt: All questions – medical |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.91 |
|
HCP: Unintelligible |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.77 |
|
Pt: Asks for understanding |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.71 |
|
Pt: Gives orientation, instructions |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.41 |
|
HCP: Open question – therapeutic |
0.0 (0.0–1.0) |
0.0 (0.0–1.0) |
0.0 (0.0–0.0) |
0.22 |
|
Pt: Gives information – other |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.83 |
|
Pt: Disagreement, criticism – direct |
0.0 (0.0–0.3) |
0.0 (0.0–1.0) |
0.0 (0.0–0.0) |
0.83 |
|
Pt: Open question – lifestyle |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.32 |
|
HCP: Closed question – other |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.83 |
|
HCP: Disagreement, criticism – direct |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.42 |
|
HCP: Self-disclosure |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.84 |
|
HCP: Asks for reassurance |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.81 |
|
HCP: Legitimation statements |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.76 |
|
Pt: Asks for reassurance |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.31 |
|
Pt: Compliment – general |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.76 |
|
Pt: All questions – psychosocial |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.36 |
|
HCP: Bid for repetition |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.26 |
|
HCP: Compliment – general |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.06 |
|
Pt: Disagreement, criticism – general |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.88 |
|
HCP: Closed question – psychosocial |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.84 |
|
HCP: Asks for permission |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.22 |
|
HCP: Open question – psychosocial |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.49 |
|
HCP: Partnership statements |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.84 |
|
Pt: All questions – other |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.26 |
|
HCP: Empathy statements |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.06 |
|
HCP: Disagreements, criticism – general |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.19 |
|
Pt: Bid for repetition |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.0 (0.0–0.0) |
0.28 |
|
RIAS coded-discussion elements not listed due to low frequency include: Pt: asks for service; Pt: legitimation statements; Pt: empathy statements; HCP: open question – other. aMann-Whitney U comparing mean frequency of RIAS utterances by CR enrollment. Pt: patient; HCP: healthcare provider; RIAS: Roter Analysis Interaction System; IQR: interquartile range. |
||||
|
Table IV. Logistic regression model testing significance of discussion perceptions and elements by cardiovascular rehabilitation enrollment |
|||||||
|
β |
SE |
Wald |
p-value |
OR |
95% CI |
||
|
Lower limit |
Upper limit |
||||||
|
SES |
0.18 |
0.28 |
0.44 |
0.51 |
1.20 |
0.70 |
2.07 |
|
HTN |
–1.24 |
0.82 |
2.25 |
0.13 |
0.29 |
0.06 |
1.46 |
|
HCP: Reassurance, optimism |
–0.21 |
0.10 |
4.04 |
0.04 |
0.81 |
0.67 |
0.99 |
|
Pt: All questions – lifestyle |
1.61 |
0.66 |
5.92 |
0.02 |
4.98 |
1.37 |
18.15 |
|
HCP: healthcare provider; HTN: hypertension; Pt: patient; SE: standard error; SES: socioeconomic status; OR: odds ratio; 95% CI: 95% confidence interval. |
|||||||
Discussion
This was the first study to our knowledge to have examined the nature of patient-HCP communication and how it relates to CR enrollment. The discussions most-often consisted of nurses and patients sharing therapeutic information about their care, and showing understanding and agreement. Trends suggested patients treated by HCPs with greater educational attainment and awareness of CR were more likely to enroll. While over-interpretation of these exploratory findings is cautioned, greater CR enrollment was related to receiving less reassurance and optimism, and the odds were 5 times greater when patients asked questions about lifestyle. Unfortunately the latter was infrequent in the recorded discussions, which were likely higher-quality conversations than unobserved “real-world” patient-HCP discussions. This suggests that despite the positive effects, the opportunity for inpatients to ask HCPs lifestyle-related questions is negligible.
The finding that HCP reassurance and optimism was conveyed approximately 5 times in each of the recorded interactions, and that greater reassurance and optimism was related to 19% lower odds of CR enrollment is highly novel. While replication in a larger sample is warranted, this certainly suggests the need for further investigation. HCPs likely convey reassurance and optimism to allay anxiety in their patients and their families. However, this may facilitate the perception in patients that they are “cured” following revascularization procedures. It is important that patients comprehend that their coronary and other arteries are still vulnerable to rupture and blockage. This should help patients understand the importance of adherence to secondary prevention medications, to make lifestyle changes and to participate in CR.
HCP endorsement of CR is found to be a principle factor for both CR referral and enrollment (11, 12, 21). Indeed, previous research has established the importance of interpersonal communication for patient health outcomes (20), and that HCPs can be successfully trained to improve the quality of their communication (22, 23). Even short-term training, of less than 10 h, is successful in improving HCP communication skills (22). While time is certainly limited in the current era of short hospital stays (24), given the substantive benefits of CR (5, 25), it is imperative that we develop evidence-based strategies to ensure CR enrollment-enhancing communication before every indicated patient is discharged.
Reasons for low CR enrollment are multi-factorial (26), but in an effort to overcome these barriers, numerous strategies such as systematic referral have been developed, and show promise in increasing CR enrollment (4, 27, 28). Future research is needed to learn to what degree optimizing patient-HCP communication at the bedside can augment CR utilization, and hence more intervention research in this line of work is necessary. It should first be tested whether nurse reassurance and patient questions around lifestyle are robustly related to patient enrollment, and the size of these effects. If significant, interventions to promote optimal communication by nurses with patients should be developed, standardized and rigorously evaluated, to see if the approach is acceptable and feasible for HCPs, and whether greater rates of enrollment can be achieved.
Caution is warranted when interpreting these results. First, this study was limited by the small number of audio-recorded discussions. It is possible that other conversational elements were related to CR enrollment, but that the study was under-powered to detect such differences. Second, the study is limited in its generalizability. Specifically, the study was conducted in an environment where CR is paid mostly through provincial health insurance, so the issues identified herein may not be applicable in systems with other payment models. Third, the results are potentially biased due to selection issues, particularly that HCPs who consented to participate may not be representative of all HCPs. Participating patients and HCP may have been more positive in their attitudes and perceptions of CR than those who did not participate. Fourth, in the absence of blinding, an expectation bias could have impacted the discussions. For instance, the recorded discussions may have been more likely to concern CR, than discussions that are not recorded. It is also possible that HCPs took extra care to optimize their communication, in a way that they would not have, if their discussions were not being recorded. It is likely that the frequency and quality of CR discussions is lower in the real-world. This is also supported by the relatively higher rate of CR referral and enrollment (10, 29) in this study than what is observed in population-based studies.
Fifth, the time-limited nature of the recordings meant that CR conversations that may have occurred at other points in the patient continuum of care. These other discussions or interactions with other HCPs may have influenced whether or not the patient was referred to CR. Sixth, the association between HCP characteristics and patient CR enrollment should be interpreted with caution, due to the nested nature of the data. With many HCPs being recorded with more than one patient, the p-values reported may be lower, thus over-emphasizing the significance of the findings. Future study should approach design and analyses with hierarchical strategies. Seventh, given the high number of RIAS categories, multiple comparisons were performed, increasing the chance of error. On the basis of chance alone, it would be expected to find more than the number of significant associations, which were observed herein. Therefore it cannot be concluded without further study that these utterances are truly related to CR enrollment. Finally, some patients may not have been referred to CR for valid personal or clinical reasons which were uncharted, and hence unmeasured in the current study. Similarly, some referred patients may not have enrolled due to unconsidered barriers such as distance to CR. Replication is warranted to ensure the findings are robust and not explained by alternative factors.
In conclusion, vast under-utilization of CR persists despite ever-growing evidence demonstrating its benefits. This study has identified some specific elements of patient-HCP discussion that may promote greater use of CR. In particular, HCPs should not over-state the effects of acute revascularization, but inform patients of the chronic nature of CAD and the health of their systemic vasculature. Patients should also be provided time to ask questions about their lifestyle. If patients have the time to fully comprehend the importance of behavioral self-management and the benefits of CR, they may be more likely to enroll and ultimately change their lifestyle and reap these benefits.
Acknowledgments
We gratefully acknowledge the statistical input of Mirka Ondrack, MSc, of York University and Yongyao Tan, of University Health Network. Also, we would like to express our appreciation to Tiziana Rivera, Pauline Glaves, Sheryl Alexandre, and Mary Attia for their support and participation. This study was funded by the Canadian Institutes of Health Research grant # TSH-112564.
References

