Shamay S. M. Ng, PhD1, Susanna Y. Cheung, MPH1, Lauren S. W. Lai, BSc (Hons)1, Ann S. L. Liu, BSc (Hons)1, Selena H. I. Ieong, BSc (Hons)1 and Shirley S. M. Fong, PhD2
From the 1Department of Rehabilitation Sciences, The Hong Kong Polytechnic University and 2Institute of Human Performance, The University of Hong Kong, Pokfulam, Hong Kong (SAR), China
OBJECTIVE: To investigate the interaction of seat height and arm position with completion times for the Five Times Sit-To-Stand test (FTSTS) in older women.
DESIGN: Cross-sectional study.
SETTING: University-based rehabilitation centre.
SUBJECTS: Thirty-three women (mean age 61.8 years, standard deviation 5.3) participated in this cross-sectional study.
METHODS: Time taken to complete the FTSTS with different seat heights (85%, 100% and 115% of knee height) and arm positions (arms across chest, or hands on thighs) was measured with a stopwatch.
RESULTS: FTSTS completion times differed significantly between seat heights of 85% and 115% knee height and between seat heights of 100% and 115% knee height for both arm positions. There was no significant difference between FTSTS completion times for the 2 arm positions at any seat height.
CONCLUSION: A lower seat height resulted in longer FTSTS completion times in women over 55 years of age, whereas arm position did not significantly affect FTSTS completion times.
Key words: sit-to-stand; female; rehabilitation.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Shamay S. M. Ng, Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong (SAR), China. E-mail: Shamay.Ng@ polyu.edu.hk
Accepted Sep 15, 2014; Epub ahead of print Dec 1, 2014
INTRODUCTION
The ability to perform sit-to-stand (STS) is a fundamental prerequisite for mobility and functional independence. The STS movement becomes mechanically demanding as people get older, since it requires sufficient lower limb muscle strength and precise postural control to transfer the body’s centre of mass (COM) forwards and upwards within a limited base of support (1). Performance of STS has been shown to be associated with muscle strength in the lower limbs (2), balance control (3–5), sensation (6), and movement strategies adopted during the manoeuvre (1).
Various STS tests have been developed to assess functional lower limb muscle strength (7), including the 10-s and 30-s chair stand tests (8, 9) and the ten times STS test (7, 10). The Five Times Sit-To-Stand test (FTSTS) is now a common functional test used to measure lower limb muscle strength (7, 11) and assess fall risk and disability (12, 13).
The FTSTS has been shown to be a reliable functional tool for use with older adults (6, 14–16) and patients with osteoarthritis (17), stroke (3, 4) or Parkinson’s disease (18). FTSTS completion times correlate moderately well with the maximal isometric knee extension force generated by healthy community-dwelling individuals aged 50–85 years (2). The FTSTS test has also been shown to be 81% effective in discriminating between older people (age range 63–90 years) with and without balance dysfunction (5). Buatois et al. (13) showed that healthy older subjects aged 65 years and over who took longer than 15 s to complete the FTSTS test had a 74% greater risk of recurrent falls than those who completed the test in a shorter time.
Although the FTSTS test is commonly used with older adults, seat height is not standardized in the assessment protocol. Csuka & McCarty (7) first used a seat height of 44.5 cm from the floor. Other seat heights, e.g. 43 (5, 6), 45 (19) and 46 cm (20), have been used in published studies. Some researchers adjust the seat height to the height of the subject’s knee (21, 22), or to a height of 90–105° knee flexion (23). Although greater knee extensor moment is clearly required in standing up from a lower seat (24), the effect of seat height on FTSTS times has not been investigated.
The arm position of the subjects in FTSTS testing has also varied in different studies. Subjects are asked to fold or cross their arms across their chest (5, 6, 21, 22), to place their hands at their waist (23), or simply to stand up without using their arms (20). One published study did not specify arm position (21). Although arm position could affect the momentum produced and influence the forward and upward shift of the body’s centre of gravity during rising from a chair (25), the effect of arm position on FTSTS completion times has also not been investigated.
Seat height and arm position during FTSTS would be expected significantly to affect FTSTS completion times among older adults. The objectives of this study were therefore to investigate the association of seat height (85%, 100% and 115% of knee height) and arm position (arms across chest or hands on thighs) with FTSTS completion times among older women.
METHODS
Participants
Thirty-three elderly women (mean age 61.8 years, standard deviation (SD) 5.3) were recruited from a local community centre (Table I). Inclusion criteria were: (i) over 55 years old; (ii) able to rise from a chair with no arm support; (3) Abbreviated Mental Test (26) score of 7 or above. Exclusion criteria were: diseases or disabilities, including heart, vascular, lung, bone or joint conditions, that might preclude standing from a chair or might hinder proper assessment.
The study was approved by the ethics committee of Hong Kong Polytechnic University and conducted according to Declaration of Helsinki guidelines for experiments with human subjects. All subjects provided written informed consent prior to study commencement.
|
Table I. Demographics of the subjects (n = 33) |
|
|
Characteristics |
Mean (SD) |
|
Age, years |
62.0 (5.3) |
|
Height, cm |
154.5 (6.1) |
|
Weight, kg |
57.9 (9.1) |
|
85% of knee height, cm |
37.9 (2.1) |
|
100% of knee height, cm |
44.7 (2.4) |
|
115% of knee height, cm |
51.4 (2.8) |
|
SD: standard deviation. |
|
Test procedure
An height-adjustable chair with no armrests, a 28.5 cm deep seat, and a backrest was used in the testing. All subjects wore their usual comfortable footwear. Subjects started in a seated position with their arms in the required position and their back against the chair backrest. The following verbal instructions were given: “Please stand up and sit down 5 times as quickly as possible. Straighten your knees when standing up, and lean your back against the backrest when sitting down.” Timing with a digital stopwatch was initiated manually at the “Go” instruction, and stopped when the subject’s back touched the backrest after the fifth stand.
Before the test, the subject was instructed to sit with the knees in 90° flexion. Their knee height was measured from the lateral knee joint line through the lateral malleolus to the ground. Each subject performed the test under 6 conditions as follows:
• Condition 1: seat height 85% of knee height, and arms across chest.
• Condition 2: seat height 85% of knee height, and hands on thighs.
• Condition 3: seat height 100% of knee height, and arms across chest.
• Condition 4: seat height 100% of knee height, and hands on thighs.
• Condition 5: seat height 115% of knee height, and arms across chest.
• Condition 6: seat height 115% of knee height, and hands on thighs.
The sequence of the 6 conditions was randomized by drawing lots. A practice trial was given at the beginning of the test. Each subject performed 2 trials for all of the 6 conditions. Subjects had a rest of at least 2 min between each trial, and longer on request, in order to prevent fatigue. The mean value of 2 trials in each experimental condition was used for data analysis.
Statistical analysis
The effects of the 3 different seat heights were analysed using 1-way repeated measures analysis of variance (ANOVA) followed by Bonferroni’s post-hoc multiple comparison test. Paired t-tests were used to examine the significance of any differences in FSTST times between the 2 arm positions. Two-way repeated measures ANOVA was used to test for any interaction between seat height and arm position in influencing the test results. Statistical Package for the Social Sciences (SPSS) software, version 18.0, was used for analysis.
RESULTS
The means and SDs of the FTSTS completion times observed in the 6 conditions are summarized in Table II. Significant differences were found between FTSTS completion times for different seat heights in both arm positions (Fig. 1). The post-hoc test showed statistically significant differences between FTSTS completion times at seat heights of 85% and 115% of knee height, and between seat heights of 100% and 115% of knee height in both the arms across chest and the hands on thighs position. A significant difference was found between the seat heights of 85% and 100% of knee height in the hands on thighs condition, but not in the arms across chest condition. There was no significant difference between FTSTS completion times for the 2 arm positions at any seat height tested. No significant interaction was found between seat height and arm position in determining FTSTS completion times.
|
Table II. Mean Five Times Sit-To-Stand test (FTSTS) times in each test condition |
|||
|
Seat height |
FTSTS times, s |
||
|
Arms folded Mean (SD) |
Hands on thighs Mean (SD) |
p-value |
|
|
85% of knee height |
12.03 (2.03) |
11.99 (2.17) |
0.830 |
|
100% of knee height |
11.51 (1.99) |
11.09 (1.83) |
0.081 |
|
115% of knee height |
10.54 (2.00) |
10.49 (2.17) |
0.805 |
|
SD: standard deviation. |
|||
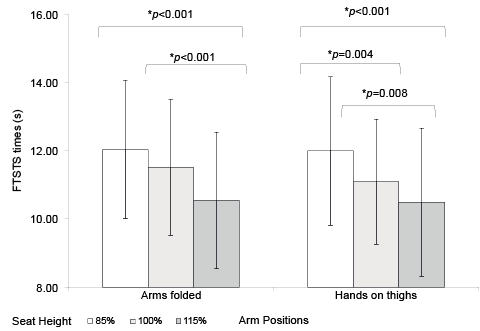
Fig. 1. Five Times Sit-To-Stand test (FTSTS) completion times for the different seat heights.
DISCUSSION
This was the first study to investigate the combined effect of seat height and arm position on FTSTS completion times in women over 55 years of age. The results showed that seat height affected FTSTS completion times, but arm position did not. FTSTS completion times were longer with lower seat height in either the arms across chest position or the hands on thighs position.
Five times sit-to-stand test completion times
Subjects took a mean of 10.49–12.03 s to complete the FTSTS, which is consistent with the times reported by other studies on older adults (7.8–12.5 s) (2, 3, 27–29). The seat heights used in those studies included 40–45 cm (2, 3, 27, 29) or 100% of the subject’s knee height with 60° hip flexion and 75° knee flexion (28). In one study subjects were instructed to place their hands on their thighs during the test (3), while the other studies used the arms-folded position (2, 27–29). The consistency between our result and those of previous studies (2, 3, 27–29) may be attributed to the similar age of the subjects (57.1–71.3 years).
In this study, women over 55 years of age were recruited in order to eliminate the effect of age and gender on FTSTS completion times. Age-related decline in muscle strength of the lower limbs occurs (30). Previous studies have demonstrated the effect of gender differences on muscle strength (31) and the performance of FTSTS (32, 33). Novy’s group (32) showed that the FTSTS completion times of women (7.6 s (SD 1.1)) were longer than those of men (7.1 s (SD 1.7)) in a study of 46 healthy adults (mean age 42.5–42.9 years). Bulter’s group (33) also showed that women ≥ 75 years took significantly longer to complete the FTSTS (p < 0.05) than men aged over 75 years.
Seat heights and Five Times Sit-To-Stand test completion times
Standing up is a mechanically demanding daily activity requiring the generation of higher moments at the hip than either walking on level ground or stair climbing (34). A higher chair decreases the degree of trunk flexion (25) and decreases the angular displacement of the trunk, hips, knees and ankles required to move the body mass forwards when rising from the chair (35). Thus, standing up from a higher chair reduces the muscle force required during the seat-off phase in order to accelerate the body mass vertically into the standing position (34, 35). In addition, a higher seat also reduces the demand on the knee extensors to stabilize the body when moving from sitting to standing (28). A biomechanical study (34) has shown that the maximum hip and knee flexion moments when rising increased by approximately 12% and 100%, respectively, from highest to lowest seat heights (115% and 65% of the subject’s knee joint height, respectively). Indeed, lowering the seat height has been found to increase the difficulty of a chair rise task, particularly when hand use is restricted (36). This could explain the longer FTSTS completion times required with a lower seat height.
Arm positions and Five Times Sit-To-Stand test completion times
Consistent with the results of previous studies with healthy individuals (25, 37–39) and those with functional limitations (40), our results also showed that there was no significant influence of arm position on FTSTS completion times.
In studies of biomechanical aspects of the STS task (41, 42), using armrests for support has been shown to result in 50% smaller hip and knee joint moments compared with not using armrests. Carr & Gentile (37) also found that the duration of the maximum support moment (defined as the percentage of the extension phase during which the support moment equals or exceeds 3 times the body weight) when rising with the hands between the knees was significantly shorter than that when the arms were restricted by holding a rod. Thus, using the hands for support may make the sit-to-stand task less demanding, but does not necessarily shorten FTSTS completion times.
Another study analysing the biomechanical factors involved in STS showed that a longer time was taken in rising from a chair using the arms to push up than rising with the arms across the chest (43). The optimum rising strategy adopted by a healthy adult involves the translation of forward momentum into vertical momentum in a coordinated manner by the trunk during the seat-off phase. For healthy subjects who can rise independently, using arms to push up could interfere with the optimum and coordinated use of the trunk and the hip extensors. This might interfere with the momentum transfer strategy (44). Neither arm position tested here involved using the arms for pushing up (subjects were explicitly told not to push against their thighs in the hands on thighs position) and all the subjects recruited were able to rise with no external support. Thus, no significant correlation was observed in this study between the 2 arm positions and FTSTS times.
Study limitations
This study has several limitations. The time taken to complete FTSTS was the main focus of the study, and quality of movement was not considered. The results could be generalized only to older women with similar inclusion criteria. Future studies should use a larger sample including men, subjects with different functional mobility, and older ages in order to broaden the generalizability of this study’s data. This study was a cross-sectional study and no causal relationships could be established. As each subject had to perform FTSTS in 6 conditions, there might have been a certain degree of learning and fatigue effect, although randomization of testing sequences by drawing lots and 2-min rest periods between each trial were intended to minimize such perturbations.
In order to simulate the rising tasks in the subjects’ daily life, some factors, such as foot position (44, 45) and weight-bearing asymmetry (44–46), which have been shown to affect STS performance, were not standardized. This study addressed only the effects of seat height and arm position on FTSTS completion times, but could not show which seat height and arm position was optimal for assessing older women.
Conclusion
Seat height has significant association with FTSTS completion times, but arm position does not. A lower seat height results in longer FTSTS completion times in women over 55 years of age.
To produce reliable assessment of changes in motor functions in older adults, it is recommended that a standard seat height should be used, at least for the same subject, when repeating FTSTS both in clinical practice and in academic research. Subjects can use their preferred arm position during the test, as arm position is not likely to be a confounding variable. Although this study was performed on women over 55 years of age, the findings could have implications for the use of FTSTS in clinical rehabilitation within geriatric, orthopaedic and neurological rehabilitation. Further studies are warranted to validate the test in different patient populations.
ACKNOWLEDGEMENTS
This study was supported by a General Research Grant (ref. 562413) from Research Grants Council to Dr Shamay S. M. Ng and her team.
The authors would like to thank Mr David Y. F. Fong for his assistance in data collection.
REFERENCES

