Ecaterina Vasluian, MSc1, Iris van Wijk, MD, PhD2, Pieter U. Dijkstra, PhD1,3,
Heleen A. Reinders-Messelink, PhD1,4 and Corry K. van der Sluis, MD, PhD1
From the 1Department of Rehabilitation Medicine, University of Groningen, University Medical Center Groningen,
Groningen, 2Rehabilitation Center De Hoogstraat, Utrecht, 3Department of Oral and Maxillofacial Surgery,
University of Groningen, University Medical Center Groningen, Groningen and 4Rehabilitation Center
“Revalidatie Friesland”, Beetsterzwaag, The Netherlands
OBJECTIVE: To evaluate use of, satisfaction with, and social adjustment with adaptive devices compared with prostheses in young people with upper limb reduction deficiencies.
METHODS: Cross-sectional study of 218 young people with upper limb reduction deficiencies (age range 2–20 years) and their parents. A questionnaire was used to evaluate participants’ characteristics, difficulties encountered, and preferred solutions for activities, use satisfaction, and social adjustment with adaptive devices vs prostheses. The Quebec User Evaluation of Satisfaction with assistive Technology and a subscale of Trinity Amputation and Prosthesis Experience Scales were used.
RESULTS: Of 218 participants, 58% were boys, 87% had transversal upper limb reduction deficiencies, 76% with past/present use of adaptive devices and 37% with past/present use of prostheses. Young people (> 50%) had difficulties in performing activities. Of 360 adaptive devices, 43% were used for self-care (using cutlery), 28% for mobility (riding a bicycle) and 5% for leisure activities. Prostheses were used for self-care (4%), mobility (9%), communication (3%), recreation and leisure (6%) and work/employment (4%). The preferred solution for difficult activities was using unaffected and affected arms/hands and other body parts (> 60%), adaptive devices (< 48%) and prostheses (< 9%). Satisfaction and social adjustment with adaptive devices were greater than with prostheses (p < 0.05).
CONCLUSION: Young people with upper limb reduction deficiencies are satisfied and socially well-adjusted with adaptive devices. Adaptive devices are good alternatives to prostheses.
Key words: physical and rehabilitation medicine; self-help devices; assistive devices; assistive technology; orthotic devices; prosthesis, upper extremity deformities; congenital.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Ecaterina Vasluian, Rehabilitation Medicine, University of Groningen, University Medical Centre Groningen, NL-9700 RB Groningen, The Netherlands. E-mail: e.golea.vasluian@umcg.nl
Accepted Sep 29, 2014; Epub ahead of print Feb 12, 2015
INTRODUCTION
Young people with an upper limb reduction deficiency (ULRD) are generally able to perform activities of daily living (ADL) (1–3) by finding solutions to facilitate difficulties in activities and participation (2). However, some ADL pose more functional limitations; for example, lifting heavy objects, engaging in sports, cycling or driving (3, 4). Although prostheses are usually prescribed for activity limitations (5–7), they are rejected by 35–45% of young people with ULRD (8) due to the weight, lack of functional gain and loss of or reduced sensory feedback, or discomfort of the prostheses (3, 9–12). Terminal devices, mountable on a prosthesis (4), seem to be specifically useful to children with ULRD for activities that require bimanual handling (e.g. lifting barbells, playing the violin) (13). These prosthetic terminal devices are expensive (13). Depending on the activity requirements (e.g. a more stable fixation to the residual limb), the terminal device might require construction of a new prosthesis/socket to accommodate the terminal device (13). Moreover, some young people (or their relatives) develop homemade adaptations that are better suited to their needs (13).
Much of the functionality of young people with ULRD, irrespective of the use of a prosthesis, is enabled by adaptive movements with the residual limb, head/face, trunk, or legs (14), use of creative solutions (e.g. ligature of the object on the residual limb with tape) or by adaptive (or assistive) devices (ADs) (2). An AD is defined as “any item, piece of equipment, or product system, whether acquired commercially, modified, or customized, that is used to increase, maintain, or improve functional capabilities of individuals with disabilities” (15). In this study, prostheses or terminal devices mounted on a prosthesis, were not considered ADs.
In the Netherlands, it is common practice for rehabilitation teams, comprising physicians, therapists and technicians, to design and provide young people with ULRD, whether or not they are using a prosthesis, with some kind of AD. These devices increase the independence of young people in ADL (16) and are usually lightweight, easy to don and doff, and inexpensive. Recently, we evaluated the activities and participation (2), prosthetic use, and rehabilitation care (3) of young people with below-elbow ULRD. It was found that many young people with below-elbow ULRD use ADs for activities such as eating, cycling, engaging in sports or playing a musical instrument (2, 3). To our knowledge, no study has addressed the use of and satisfaction with ADs in young people with ULRD and compared users’ satisfaction with ADs with satisfaction with a prosthesis. Furthermore, young people with below-elbow ULRD seem to wear prostheses to achieve social acceptance and integration (3), but the social adjustment of young people with ULRD using ADs is unknown.
The first aim of this study is to evaluate the use of ADs for facilitating difficult ADL in young people with ULRD and the factors influencing the use of ADs and prostheses. The second aim is to compare the use of, satisfaction with, and social adjustment with ADs with that of prostheses.
METHODS
A cross-sectional study using questionnaires was used for data collection (between February and June 2013). Ethical approval was granted by the University Medical Ethical Committee (M12.128982). Informed consent was obtained from all participants: from the parent/guardian of a child younger than 12 years old, from the parent and the child if the young person was 12–17 years old, and from the adolescent only when over 17 years of age. Participants were informed that data would be anonymized and access to data was restricted only to involved researchers. After returning the fully completed questionnaire, the participant was given a gift voucher (EUR 10).
Recruitment and participants
Participants were recruited from 9 rehabilitation centres throughout the Netherlands. In addition, the adoption association of children with birth defects sent invitation e-mails with a link to the electronic version of the questionnaire as an extra reminder to participate (most adopted children with ULRD were also registered in rehabilitation centres participating in this study).
Participants, both young people and parents of children younger than 12 years, were included if the young person was between 2 and 20 years old, and had a transverse (wrist and hand, below-elbow, or above/through-elbow level) or longitudinal ULRD. Complex symbrachydactyly (very short webbed fingers) was also included under transversal reduction deficiencies. Participants who had mild symbrachydactyly or ULRD at the hand level with fewer than 4 fingers missing were excluded as they were considered having low-degree of functional impairment. Participants with poor command of the Dutch language were excluded.
Procedure
An electronic and a paper version of the questionnaire were available. Envelopes containing the paper version of the questionnaire, an invitation letter from the physician, an information letter from the researchers, and an informed consent form were posted to participating rehabilitation centres. Because researchers did not have access to participant’s personal details the questionnaire may have been sent twice to some participants. Participating centres were asked to select current patients, not those who had been transferred to another centre, to avoid doubles, and to post the envelopes with the information and questionnaires.
Parents of children between 2 and < 7 years old, parents together with young people of 7–< 13 years old, and adolescents of 13–20-year-olds were instructed to complete the questionnaire.
Questionnaire
Data about young people with ULRD and ADs, collected from our previous studies (2, 3), were used to develop the main part of the 37-item questionnaire. In addition to participants’ characteristics, the questionnaire assessed difficulties in ADL, types of and use of ADs (maximum 5 ADs), use of prostheses in daily activities, user’s satisfaction with ADs and prostheses, social adjustment with ADs and prostheses, and suggestions for improving the use of ADs. The majority of questions had a single answer option (Likert scale or “yes/no” answers). Two questions had multiple answer options (Appendix I).
To evaluate user’s satisfaction with ADs compared with prosthesis, the Dutch version of the Quebec User Evaluation of Satisfaction with assistive Technology (D-Quest) questionnaire was used (17). The D-Quest evaluates 2 domains: satisfaction with the device and satisfaction with the rehabilitation services. Questions on satisfaction with rehabilitation services were answered only by participants with ADs that were developed in a rehabilitation centre or an orthopaedic workshop.
Social adjustment was assessed with a subscale of the Trinity Amputation and Prosthesis Experience Scales questionnaire (TAPES, upper limb version, social adjustment subscale of psychosocial adjustment) (18, 19). The minimum-maximum scores for TAPES social adjustment subscale are 0–4 points (poor to very good social adjustment). Studies on internal consistency and factor structure recommended the use of TAPES in upper limb amputees (18, 20). Participants were asked to choose their most important AD and then answer the questions about their satisfaction and social adjustment with that device and the prosthesis (if applicable, Appendix I). “Most important” AD could be related to its necessity in performing activities or its frequent use, independent of appearance. A professional editor with extensive experience in developing questionnaires for paediatric and adult populations reviewed the questionnaire. The wording of D-Quest and TAPES questions was simplified to enable understanding of the questions by participants of all ages. The entire questionnaire was tested for clarity and conciseness on a group of 4 parents and 7 unimpaired children. Two independent healthcare professionals (an occupational therapist and a prosthetist) working with children with ULRD reviewed the questionnaire. The comments and suggestions received were used to improve the formulation of the questions.
Statistical analysis
The ADLs were grouped according to the International Classification of Functioning, Disability and Health (ICF) component – activities and participation – and its domains: self-care, mobility (including transportation methods), communication, recreation and leisure, and domestic life and work/employment (21). Domestic life and work/employment were considered as a single category. Age was grouped (2–< 7, 7–< 13, and 13–20 years old) to provide insight into the difficulties experienced in ADL and ADs by different age groups.
To facilitate analyses and data presentation, answers regarding experienced difficulties in ADL and satisfaction with the appearance of the most important AD/prosthesis were dichotomized (Appendix I). “Yes/no” variables were created for each preferred solution used in ICF domains, denoting use or non-use of the respective solution.
Binary logistic regressions were used to determine the factors predicting the use of ADs or prostheses. The outcome variables were past/present use of ADs and past/present use of prostheses. The predictor variables were age, gender, number of difficulties in ADL, ULRD type, and level of transversal ULRD (0 = above/through-elbow, 1 = below-elbow; wrist and hand level was excluded because prostheses are not prescribed for young people with this ULRD level).
Paired t-tests were used to determine the differences in satisfaction (D-Quest) and social adjustment (TAPES) between most important AD and prosthesis. According to D-Quest instructions for analysis (22), overall and per-item satisfactions were assessed.
The significance level was set at p ≤ 0.05 and all analyses were performed with IBM SPSS Statistics for Windows, version 20.0 (IBM Corp. Armonk, NY, USA).
RESULTS
In total, 523 questionnaires were sent out and 223 (43%) were returned. Two uncompleted questionnaires were returned due to outdated address and 3 questionnaires were excluded because the participants did not meet the inclusion criteria (mild symbrachydactyly, radioulnar synostosis, and partially amputated little finger). In total, 218/523 (42%) questionnaires were included, of which 30 questionnaires were completed online. All participants gave consent and no double completion of the questionnaires was identified.
Participants’ characteristics and adaptive devices/prostheses use
Of the 218 participants, 58% were boys, 52% had a below-elbow ULRD, 76% with past/present use of an AD and 37% with past/present use of a prosthesis (Table I). The reasons for never using an AD were being able to perform any ADL independently (60% of n = 52), performing activities in a different manner (35%), being currently too young (10%), or never having heard about ADs (4%). Of the young people with past/present use of an AD (n = 166), 27% had 1 AD, 45% had 2 ADs, and 28% had 3 or more ADs. In total, 360 ADs were used by the participants (Table II, Fig. 1).
Table I. Characteristics of the participants, upper limb reduction deficiency, and use of adaptive device and prostheses for the age groups and the total group | ||||
Characteristics | 2–< 7 years old n (%) | 7–< 13 years old n (%) | 13–20 years old n (%) | Total n (%) |
Total | 64 (29.4) | 102 (46.8) | 52 (23.9) | 218 (100.0) |
Boys | 43 (19.7) | 56 (25.7) | 28 (12.8) | 127 (58.3) |
Girls | 21 (9.6) | 46 (21.1) | 24 (11.0) | 91 (41.7) |
ULRD location | ||||
Unilateral | 61 (28.0) | 94 (43.1) | 46 (21.1) | 201 (92.2) |
Bilateral | 3 (1.4) | 8 (3.7) | 6 (2.8) | 17 (7.8) |
ULRD type | ||||
Longitudinal | 13 (6.0) | 11 (5.0) | 5 (2.3) | 29 (13.3) |
Transversal | 51 (23.4) | 91 (41.7) | 47 (21.6) | 189 (86.7) |
Above/ | 3 (1.4) | 6 (2.8) | 7 (3.2) | 16 (7.3) |
Below-elbow | 30 (13.8) | 53 (24.3) | 30 (13.8) | 113 (51.8) |
Wrist and hand | 18 (8.3) | 32 (14.7) | 10 (4.6) | 60 (27.5) |
Past/present use of ADs (total) | 41 (18.8) | 90 (41.3) | 35 (16.1) | 166 (76.1) |
Currently using | 37 (17.0) | 70 (32.1) | 25 (11.5) | 132 (60.6) |
Not using anymore | 4 (1.8) | 20 (9.2) | 10 (4.6) | 34 (15.6) |
ADs never used | 23 (10.6) | 12 (5.5) | 17 (7.8) | 52 (23.9) |
Past/present use of prosthesis (total) | 15 (6.9) | 33 (15.1) | 32 (14.7) | 80 (36.7) |
Currently using | 7 (3.2)a | 13 (6.0)a | 10 (4.6) | 30 (13.8) |
Myoelectric | 2 (0.9) | 5 (2.3) | 5 (2.3) | 12 (5.5) |
Body-powered | 3 (1.4) | 3 (1.4) | 2 (0.9) | 8 (3.7) |
Cosmetic/passive | 1 (0.5) | 3 (1.4) | 3 (1.4) | 7 (3.2) |
Others | 0 | 1 (0.5) | 0 | 1 (0.5) |
Not using anymore | 8 (3.7) | 20 (9.2) | 22 (10.1) | 50 (22.9) |
Myoelectric | 0 | 6 (2.8) | 12 (5.5) | 18 (8.3) |
Body-powered | 0 | 3 (1.4) | 1 (0.5) | 4 (1.8) |
Cosmetic/passive | 8 (3.7) | 9 (4.1) | 8 (3.7) | 25 (11.5) |
Others | 0 | 2 (0.9) | 1 (0.5) | 3 (1.4) |
Prosthesis never used | 49 (22.5) | 69 (31.7) | 20 (9.2) | 138 (63.3) |
AD and prosthesis | 9 (4.1) | 26 (11.9) | 21 (9.6) | 56 (25.7) |
AD and no prosthesis | 32 (14.7) | 64 (29.4) | 14 (6.4) | 110 (50.5) |
No AD nor prosthesis | 17 (7.8) | 5 (2.3) | 6 (2.8) | 28 (12.8) |
Prosthesis and no AD | 6 (2.8) | 7 (3.2) | 11 (5.0) | 24 (11.0) |
aProsthesis type not specified in 1 participant. AD(s): adaptive device (s); ULRD: upper limb reduction deficiency. | ||||
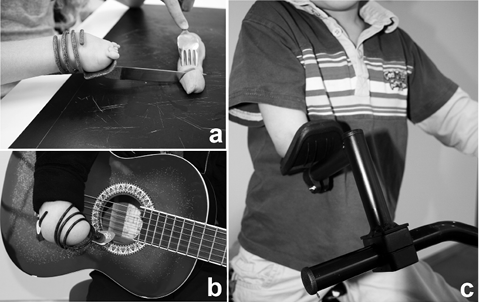
Fig. 1. Examples of adaptive devices used for: (a) eating, (b) playing a musical instrument, and (c) riding a bike.
Difficulties in ADL/described types of ADs. More than half of participants experienced difficulties in the ICF domains self-care (using cutlery (73%) and tying shoelaces (60%)), in recreation and leisure (playing a musical instrument (69%)), and in household activities (60%) (Table II). Of the 360 ADs, 43% were used for eating with cutlery, 28% for riding a bicycle, 5% for leisure activities, 4% for doing/engaging in sports, and 4% for playing a musical instrument (Table II). Most ADs were used always or very often (64% of ADs).
|
Table II. Difficulties and adaptive devices used in activities of daily living grouped into ICF domains for the age groups and the total group |
|||||||||
|
ICF domains and ADL |
Difficulties |
ADs used |
|||||||
|
2–<7 years old n/v (%) |
7–<13 years old n/v (%) |
13–20 years old n/v (%) |
Total n/v (%) |
2–<7 years old n (%) |
7–<13 years old n (%) |
13–20 years old n (%) |
Total n (%) |
||
|
Self-care |
|||||||||
|
Using cutlery |
47/64 (73.4) |
81/102 (79.4) |
30/52 (57.7) |
158/218 (72.5) |
34 (9.4) |
95 (26.4) |
27 (7.5) |
156 (43.3) |
|
|
Dressing or undressing |
34/61 (55.7) |
16/102 (15.7) |
4/52 (7.7) |
54/215 (25.1) |
3 (0.8) |
7 (1.9) |
3 (0.8) |
13 (3.6) |
|
|
Tooth brushing |
3/62 (4.8) |
3/100 (3.0) |
0/52 |
6/214 (2.8) |
– |
– |
– |
– |
|
|
Self-washing/taking a shower |
13/58 (22.4) |
15/101 (14.9) |
1/52 (1.9) |
29/211 (13.7) |
– |
2 (0.6) |
1 (0.3) |
3 (0.8) |
|
|
Using the toilet |
17/58 (29.3) |
8/102 (7.8) |
3/52 (5.8) |
28/212 (13.2) |
– |
3 (0.8) |
– |
3 (0.8) |
|
|
Tying shoelaces |
35/41 (85.4) |
56/95 (58.9) |
22/51 (43.1) |
113/187 (60.4) |
– |
1 (0.3) |
– |
1 (0.3) |
|
|
Mobility |
|||||||||
|
Riding a bicycle |
33/59 (55.9) |
19/101 (18.8) |
10/52 (19.2) |
62/212 (29.2) |
34 (9.4) |
52 (14.4) |
15 (4.2) |
101 (28.1) |
|
|
Riding a moped, a scooter or driving |
– |
– |
9/22 (40.9) |
9/22 (40.9) |
– |
– |
5 (1.4) |
5 (1.4) |
|
|
Communication |
|||||||||
|
Writing |
8/50 (16.0) |
18/102 (17.6) |
3/52 (5.8) |
29/204 (14.2) |
1 (0.3) |
2 (0.6) |
1 (0.3) |
4 (1.1) |
|
|
Using a computer keyboard |
14/39 (35.9) |
33/100 (33.0) |
7/52 (13.5) |
54/191 (28.3) |
– |
2 (0.6) |
6 (1.7) |
8 (2.2) |
|
|
Recreation and leisure |
|
||||||||
|
Doing/engaging in sports |
19/49 (38.8) |
40/102 (39.2) |
15/51 (29.4) |
74/202 (36.6) |
1 (0.3) |
9 (2.5) |
5 (1.4) |
15 (4.2) |
|
|
Handcrafting |
34/64 (53.1) |
46/102 (45.1) |
12/49 (24.5) |
92/215 (42.8) |
3 (0.8) |
5 (1.4) |
– |
8 (2.2) |
|
|
Playing a musical instrument |
15/19 (78.9) |
43/61 (70.5) |
14/24 (58.3) |
72/104 (69.2) |
1 (0.3) |
8 (2.2) |
5 (1.4) |
14 (3.9) |
|
|
Leisure activitiesa |
37/62 (59.7) |
41/101 (40.6) |
13/48 (27.1) |
91/201 (43.1) |
4 (1.1) |
13 (3.6) |
2 (0.6) |
19 (5.3) |
|
|
Domestic life and work/employment |
|||||||||
|
Household activitiesb |
9/17 (52.9) |
38/59 (64.4) |
28/50 (56.0) |
75/126 (59.5) |
1 (0.3) |
2 (0.6) |
4 (1.1) |
7 (1.9) |
|
|
Work/employmentc |
0/1 |
2/5 (40.0) |
10/38 (26.3) |
12/44 (27.3) |
– |
– |
– |
– |
|
|
Other or multiple ADL |
1/1 (100.0) |
6/6 (100.0) |
– |
7/7 (100.0) |
– |
3 (0.8) |
– |
3 (0.8) |
|
|
Total ADs |
82 (22.8) |
204 (56.7) |
74 (20.6) |
360 (100) |
|||||
|
aLeisure activities such as playing Wii, jumping rope, or swinging. bHousehold activities such as peeling potatoes, washing, making pancakes. cWork such as (part-time) job, summer job. Percentages for “Difficulties” represent the number of young people having difficulties (n) out of the number or valid responses per age category (v); percentages for “ADs used” are calculated from the total number of ADs, n = 360. ICF: International Classification of Functioning Disability and Health; ADL: activities of daily living; AD(s): adaptive device(s); “–”: no difficulty or no AD was reported. |
|||||||||
Of the 166 participants who had used ADs in the past or were still using ADs, 165 described their most important AD. Of these 166 participants, 56 had used a prosthesis in the past or were currently using a prosthesis as well. Due to non-use of his AD, 1 participant did not complete this section of the questionnaire. The most important AD was mostly used for the ADL using cutlery (52% of 165), riding a bicycle (33%), engaging in sports (4%), dressing or undressing (3%), or playing a musical instrument (3%).
Participants acquired their most important AD and prostheses when they were younger than 5 years of age (46%, 61%, respectively) or between 5 and 8 years of age (37% and 18%, respectively). The most important AD was used for several consecutive years, on average for 4.6 years, standard deviation (SD) = 3.2 (67% of participants) or it was used for less than 3 months (12%). Prostheses were used for several consecutive years, on average for 6.7 years, SD = 4.2 (30%), less than 3 months (25%), and 18% used their prosthesis intermittently. The most important AD as well as prostheses were used everywhere (44%, 41%, respectively), at home only (34% and 9%), or at home and in environments with acquaintances; school, family or friends (19% and 34%).
Manufacturer of ADs. The ADs were mostly made in rehabilitation centres by specialized professionals (79% of 360 ADs), particularly by rehabilitation teams comprising a technician and an occupational therapist or physiotherapist. The remaining ADs were developed by the young people themselves or by a family member (16%), or were acquired from other sources (4%).
Use of ADs in the context of preferred solutions to facilitate difficult ADL. The most preferred solution to facilitate difficult ADL was using unaffected and affected upper limbs and other body parts (39–96% of participants in different ADL, Table III). A considerable proportion of young people preferred ADs (12–48%). The most preferred solution for using cutlery was using ADs (46%, Table III). External help was preferred more than ADs for tying shoelaces (46% of respondents) and for domestic life and work/employment activities (21%). Prostheses were the least preferred solution (over all ICF domains ≤ 9%).
|
Table III. Preferred solutions for performing activities of ICF domains |
||||
|
ICF domains (v) |
Preferred solutions |
|||
|
AD n (%) |
Prosthesis n (%) |
Hands n (%) |
Help n (%) |
|
|
Self-carea (214) |
103 (48.1) |
9 (4.2) |
186 (86.9) |
106 (49.5) |
|
Using cutlery (211) |
96 (45.5) |
6 (2.8) |
82 (38.9) |
27 (12.8) |
|
Tying shoelaces (169) |
2 (1.2) |
6 (3.6) |
83 (49.1) |
78 (46.2) |
|
Mobilitya (191) |
58 (30.4) |
17 (8.9) |
117 (61.3) |
2 (1.0) |
|
Riding a bicycle (186) |
54 (29.0) |
17 (9.1) |
113 (60.8) |
2 (1.1) |
|
Communicationa (181) |
7 (3.9) |
6 (3.3) |
174 (96.1) |
3 (1.7) |
|
Recreation and leisurea (210) |
40 (19.0) |
13 (6.2) |
183 (87.1) |
36 (17.1) |
|
Playing a musical instrument (75) |
16 (21.3) |
1 (1.3) |
56 (74.7) |
2 (2.7) |
|
Domestic life and work/employmenta (128) |
16 (12.4) |
5 (3.9) |
90 (69.8) |
27 (20.9) |
|
aEach solution used per ICF domain was coded as a dichotomous variable (yes, when at least 1 of the activities contributing to the ICF domain was performed with the corresponding solution). Percentages are calculated from the total number of valid responses (v). AD: adaptive device; Hands: unaffected hand and affected arm and/or other body parts; Help: with help from somebody; n: number of children; v: total number of children with valid responses in each activity or ICF domain. The answer category “sometimes adaptive device or prosthesis” was not presented in the table due to low numbers. ICF: International Classification of Functioning; “not applicable” answers for all of the activities within an ICF-domain were excluded. |
||||
Factors influencing the use of ADs/prostheses. Results of logistic regression showed that, when controlling for age, gender and ULRD type, the ADs were more likely to have been used when experiencing difficulties in ADL (odds ratio (OR) = 1.17, Table IV).
In the case of young people with transversal ULRD at a more proximal level than wrist and hand level, an AD was more likely to have been used by young people experiencing difficulties in ADL (OR = 1.25). ADs were less likely to have been used by young people with transversal ULRD if they have had a prosthesis (OR = 0.36).
Prostheses were more likely to have been used by older young people (OR = 1.14) and less likely to have been used by boys (OR = 0.44), and by young people who have had an AD (OR = 0.35, Table IV).
|
Table IV. Results of logistic regression with the use of adaptive devices or prostheses as outcome variable and the participants’ characteristics as predictors |
||||||
|
Past/present use of ADs or prostheses |
Yes |
No |
β (SE) |
p |
OR (95% CI) |
|
|
ADsa (all ULRD levels) |
n = 166 |
n = 52 |
||||
|
Age (centred at 2 years old), mean (SD) |
8.3 (4.3) |
7.9 (6.0) |
0.03 (0.04) |
0.374 |
1.03 (0.96; 1.11) |
|
|
Gender (male), n (%) |
97 (58.4) |
30 (57.7) |
0.07 (0.33) |
0.841 |
1.07 (0.56; 2.05) |
|
|
Number of difficulties in ADL, n (%) |
4.7 (3.0) |
3.6 (2.8) |
0.16 (0.06) |
0.010* |
1.17 (1.04; 1.32) |
|
|
ULRD type (transversal), n (%) |
147 (88.6) |
42 (80.8) |
0.73 (0.45) |
0.104 |
2.08 (0.86; 5.05) |
|
|
Constant, n (%) |
–0.42 (0.62) |
0.505 |
0.66 (0.19; 2.24) |
|||
|
ADsa,b (ULRD levels higher than the wrist) |
n = 99 |
n = 30 |
||||
|
Age (centred at 2 years old), mean (SD) |
8.6 (4.5) |
8.9 (6.0) |
0.05 (0.05) |
0.315 |
1.05 (0.95; 1.16) |
|
|
Gender (male), n (%) |
57 (57.6) |
16 (53.3) |
–0.14 (0.45) |
0.763 |
0.87 (0.36; 2.12) |
|
|
Number of difficulties in ADL, n (%) |
4.8 (3.0) |
3.1 (2.6) |
0.23 (0.10) |
0.017* |
1.25 (1.04; 1.51) |
|
|
Transversal ULRD (below-elbow), n (%) |
85 (85.9) |
28 (93.3) |
0.11 (0.87) |
0.897 |
1.12 (0.21; 6.10) |
|
|
Past/present use of prostheses, n (%) |
49 (49.5) |
22 (73.3) |
–1.02 (0.52) |
0.048* |
0.36 (0.13; 0.99) |
|
|
Constant, n (%) |
0.50 (1.13) |
0.658 |
1.65 (0.18; 15.23) |
|||
|
Prosthesesa,b (ULRD levels higher than the wrist) |
n = 71 |
n = 58 |
||||
|
Age (centred at 2 years old), mean (SD) |
10.0 (4.9) |
7.1 (4.4) |
0.13 (0.04) |
0.004* |
1.14 (1.04; 1.24) |
|
|
Gender (male), n (%) |
33 (46.5) |
40 (69.0) |
–0.82 (0.40) |
0.038* |
0.44 (0.20; 0.96) |
|
|
Number of difficulties in ADL, n (%) |
3.8 (3.0) |
5.0 (2.9) |
–0.04 (0.07) |
0.513 |
0.96 (0.84; 1.09) |
|
|
Past/present use of ADs, n (%) |
49 (69.0) |
50 (86.2) |
–1.06 (0.51) |
0.038* |
0.35 (0.13; 0.95) |
|
|
Constant, n (%) |
0.64 (0.65) |
0.324 |
1.90 (0.53; 6.79) |
|||
|
aAge was centred at 2 years old. Reference categories for gender – female, for ULRD type – longitudinal ULRD, for transversal ULRD – above/through-elbow level. bIncluded: 22 participants were with past/present use of a prosthesis, 50 participants were with past/present use of an AD, 49 participants were with past/present use of both, and 8 participants used neither. Excluded: transversal ULRD at the wrist and hand level because prostheses are not prescribed for children with wrist or hand ULRD; and longitudinal ULRD. Due to low cell numbers, the variable “Transversal ULRD” has been excluded from the analysis conducted for prosthetic use. *p<0.05. Percentage are calculated from the total number of “Yes” (past/present use of ADs or past/present use of prostheses) or “No” category (never used ADs/never used prostheses). AD(s): adaptive device(s); ULRD: upper limb reduction deficiency; β: coefficient showing weighting of each factor in the model; SE: standard error; OR: odds ratio; 95% CI: 95% confidence interval for the estimated odds ratio; “ever used”: devices that were used in the past or currently. |
||||||
Satisfaction and social adjustment with adaptive devices vs prostheses
Satisfaction with most important AD compared with satisfaction with prostheses (D-Quest). Participants were more satisfied with their most important AD than with a prosthesis (p < 0.01, Table V). Higher satisfaction was recorded for their most important AD compared with a prosthesis (Table V) in the D-Quest items: dimensions, weight, adjustment, ease of use, and comfort (p < 0.01). No difference was seen between the satisfaction with rehabilitation services for most important AD and the satisfaction with rehabilitation services for prostheses.
Participants were (very) satisfied with the appearance of their most important AD (87%) and of the prosthesis (66%; question not part of D-quest).
Social adjustment with most important AD compared with social adjustment with prostheses. The social adjustment with the AD was significantly higher than with the prosthesis (p = 0.044, Table V).
Suggestions for improving the use of adaptive devices
Of 218 participants, 48% wished for special online facilities to exchange ideas about ADs and to see the ADs; 36% wanted more information about AD types; 25% suggested that more workshops and/or meetings about ADs should be organized together with other children with ULRD. Other suggestions were more colours (18%), more diversity for ADs (17%), more ADs for sports (11%; e.g. for hockey, horseback riding, or judo), a short training for ADs (8%) and cheaper ADs (6%).
DISCUSSION
This study investigated, for the first time, the use of, satisfaction with, and social adjustment with ADs vs prostheses in young people with ULRD. More than half of the young people with ULRD reported having difficulties in ADL for which they used different solutions. Along with preferentially using their unaffected and affected upper limbs and other body parts as a natural process in motor learning (23), young people with ULRD used ADs much more than prostheses. The ADs were important for performing ADL of self-care (using cutlery), enabling mobility (riding a bicycle), or for recreation and leisure, and were mainly developed by healthcare professionals. ADs appeared to be especially useful in children who encounter many difficulties in ADL performance. Satisfaction with the ADs was greater than satisfaction with prostheses. No difference was seen between ADs and prostheses regarding satisfaction with rehabilitation services. Social adjustment was somewhat better with the ADs than with the prostheses.
Difficulties in activities of daily living and use of adaptive devices
Activities posing difficulties in young people with ULRD are those requiring both hands to maintain a stable position (24). Our participants reported difficulties in activities requiring bilateral manipulation, such as using cutlery to cut food while stabilizing it with a fork, tying shoelaces, playing a musical instrument, or riding a bike. The last activity has to be performed with both arms for stability and safety reasons. The use of ADs has been recommended for children experiencing difficulties in activities, and to improve participation (16), to diminish physical effort, or to reduce the risk of injuries (24). However, the heterogeneity in terminology, data-collection methods, and outcomes in studies about assistive devices in young people with impairments (16) hampers comparison with our results. The studies about ADs were mostly descriptions of devices or rehabilitation with devices (4, 13, 25, 26). Data on actual use and satisfaction with ADs in children with ULRD were lacking.
A variety of ADs has been described in adults (≥ 18 years old) with different impairments (17). ADs were used for personal care (19% of 2002 participants), communication (5%), mobility (9%), and 15% had prostheses (since prostheses were considered as ADs in that study) (17). People with cerebral palsy (CP) use upper-limb ADs for personal care and communication (between 23% and 79% of people with CP) (26). Although many of the devices resembled the devices in our study such as pencil holders, adapted cutlery or dressing sticks, the people with CP had bilateral upper-limb impairments and were older (14–77 years old) than our participants. Regardless of differences in the literature and types of impairment, ADs seem to be used predominantly for personal care (self-care) as also found in our study.
The majority of young people with ULRD in the present study, 80% of 166 participants, had either used or are currently using ADs. In contrast, in persons with CP, 46% stopped using ADs after the first year of usage due to improvement in function or other alternatives found (26). Another study also reported lower rates for abandonment of ADs in impaired Dutch persons when compared with the rates in the literature (27). The authors speculated that a number of investigated devices were difficult to obtain and therefore these devices were less likely to be rejected (27). This explanation does not apply to our users because it is easy and inexpensive to obtain an AD in the Netherlands and the costs are often covered by insurance companies.
Preferred solutions for activities of daily living
Although our participants experienced difficulties in ADL, their preferred solution to facilitate ADL performance was using their unaffected and affected upper limbs or other body parts. This finding supports the literature outcomes suggesting that young people with ULRD can perform most ADL without help accessories (prostheses) (1, 28). What seems to contribute to the use of ADs is the number of difficulties experienced in ADL: the more difficulties, the higher the chance of using ADs. The use or non-use of ADs by young people with ULRD also seems to be task- and age-specific according to clinical observations, although this was not found in our study. As such, ADs are used especially during the life phases when new skills are learned. For example, young people need an AD when learning to ride a bike. At an older age, they develop skills that allow them to ride a bike without an AD. Note that there are some cultural specifics regarding the ADs used for mobility because riding a bicycle is a common and popular means of transport in the Netherlands.
Prostheses were more likely to be used with increasing age, although this observation contradicts other findings (29). From the literature on the use of prostheses, it is known that young people with ULRD, using or not using prostheses, behave differently. At puberty, some use a prosthesis to appear “bodily-complete” or for functionality purposes, while other young people who used a prosthesis reject it because of people staring at them, poor cosmesis or lack of functional gain (3, 9, 12). The use of ADs and the use of prostheses seem to inter-influence each other. Young people with more proximal ULRD than the wrist are less likely to use ADs if they use a prosthesis and vice versa. When interpreting these results, consider that our analyses on factors influencing the use of ADs or prostheses included participants (n=49) with past/present use of both. These participants were included once in the analysis as users of ADs and once as users of prosthesis, indicating that these analyses are not independent. Future studies should examine the abandonment of ADs and the influence of socio-emotional development of young people with ULRD on the use of ADs.
Satisfaction with adaptive devices compared with satisfaction with prostheses
Our results demonstrated that satisfaction with ADs was significantly greater than satisfaction with prostheses in several aspects: dimensions, weight, adjustment, ease of use, comfort, and effectiveness (Table V). These aspects have been reported as reasons for prosthesis rejection in previous research (3, 9–12). ADs seem to provide the user with the needed functionalities and appropriate device properties. As such, healthcare professionals working with young people with ULRD should regard the provision of ADs as an efficient treatment. Furthermore, ADs are a cost-efficient option because they do not require sophisticated materials and technologies or extended training programmes, as is the case with prostheses (6, 7, 30–32). The manufacture of ADs is also a relatively fast process with minimal waiting times for users.
Social adjustment
Considering our previous findings that young people with below-elbow ULRD use prostheses to avoid being stared at (3), we expected satisfaction with prostheses to be better than satisfaction with ADs. However, this was not the case in the current participants, which might be explained by greater increase in ADL independence when using ADs compared with prostheses. Being independent in activities gives young people a sense of fulfilment and equality with their peers (33, 34). As such, ADs contribute to some extent to the normality of young people with ULRD. The importance of normality in impaired young people has been stressed previously in the literature (33–35).
Compared with their peers, young people with ULRD appear to be happier overall (1), perceive their physical appearance as their peers perceive it (36), and are similarly psychosocially adjusted (37). Using a prosthesis was suggested to be beneficial for psychosocial adjustment (37). Although we did not evaluate psychosocial adjustment extensively, our results seem to support the above-mentioned findings. Young people with ULRD are socially well adjusted, and ADs as well as prostheses may contribute to that.
Clinical implications and suggestions
The findings of this study have highlighted the impact of the use of ADs in young people with ULRD, which advocates for confidently introducing ADs in the current treatment options of young people with ULRD. Online facilities with visual presentations and more information about different types of ADs should be created, as suggested by our participants. Importantly, healthcare professionals should clarify the functional benefits of both ADs and prostheses to rule out unrealistic expectations (3).
Researchers should also assess the differences between ADs and prostheses regarding compensatory movements and overuse complaints.
Study limitations
A limitation of this study might be the somewhat low response rate. It is possible that young people with ULRD were disinterested in participating because they generally function well and do not perceive themselves as impaired. However, a decreasing trend for response rates to surveys in the last decade has been reported (38, 39).
Young people with bilateral ULRD might have had different functional needs, but a separate analysis was not possible because the group with bilateral ULRD was too small (n = 17). However, the results of post-hoc analyses (regression and t-tests), conducted only with the unilateral ULRD group, did not display substantial differences compared with the results in Table IV and Table V (Appendix II, the t-test results were similar to those in Table V).
|
Table V. Satisfaction (D-Quest)a and social adjustment (TAPES) with adaptive devices and prostheses |
|||||
|
Questionnaire |
AD |
Prosthesis |
Mean difference (SD) |
p-value |
|
|
Mean (SD) |
Mean (SD) |
||||
|
D-Quest – Devicesb (n = 46) |
4.30 (0.45) |
3.28 (0.82) |
1.02 (0.87) |
< 0.001* |
|
|
Dimensions (n = 49) |
4.49 (0.58) |
3.12 (1.30) |
1.37 (1.45) |
< 0.001* |
|
|
Weight (n = 48) |
4.46 (0.50) |
2.71 (1.13) |
1.75 (1.25) |
< 0.001* |
|
|
Adjustment (n = 43) |
4.09 (0.72) |
3.26 (1.09) |
0.84 (1.17) |
< 0.001* |
|
|
Safety (n = 45) |
4.33 (0.60) |
4.11 (0.88) |
0.22 (0.79) |
0.067 |
|
|
Durability (n = 45) |
4.20 (0.87) |
3.98 (0.92) |
0.22 (1.17) |
0.208 |
|
|
Ease of use (n = 47) |
4.28 (0.85) |
2.74 (1.33) |
1.53 (1.44) |
< 0.001* |
|
|
Comfort (n = 47) |
4.17 (0.67) |
3.47 (1.12) |
0.70 (1.30) |
0.001* |
|
|
Effectiveness (n = 47) |
4.49 (0.72) |
3.02 (1.29) |
1.47 (1.49) |
< 0.001* |
|
|
D-Quest – Rehabilitation servicesb (n = 37) |
4.21 (0.57) |
4.19 (0.62) |
0.02 (0.67) |
0.839 |
|
|
Service delivery (n = 38) |
4.26 (0.86) |
4.11 (0.92) |
0.16 (1.17) |
0.413 |
|
|
Repairs and servicing (n = 31) |
4.19 (0.60) |
4.16 (0.64) |
0.03 (0.60) |
0.768 |
|
|
Professional services (n = 38) |
4.29 (0.65) |
4.32 (0.77) |
–0.03 (0.72) |
0.822 |
|
|
Follow-up (n = 37) |
4.24 (0.49) |
4.22 (0.67) |
0.03 (0.60) |
0.786 |
|
|
TAPES – Social adjustment (n = 45) |
3.28 (0.68) |
3.12 (0.86) |
0.16 (0.50) |
0.044* |
|
|
aOverall and per D-Quest item scores were presented; n = 165 participants completed the D-Quest (one 18–20 years old participant had recall difficulties on D-Quest). bOverall score. In this analysis, participants who responded to ≥ 6 questions in the Devices section and ≥ 3 questions in the Rehabilitation services section (according to D-Quest instructions for analysis) were included (see reference 22). *p<0.05. AD: (most important) adaptive device; SD: standard deviation; n: number of participants with valid responses; D-Quest: Dutch version of Quebec User Evaluation of Satisfaction with assistive Technology; TAPES: Trinity Amputation and Prosthesis Experience Scales. |
|||||
Although the questionnaire was tested in a pilot environment and an experienced editor and healthcare professionals were consulted, it was not feasible to test its validity and reliability. Further studies are required to validate the questionnaire, as well as the D-Quest and TAPES questionnaires, in the Dutch paediatric patients.
Participants’ responses may have suffered from recall bias, especially in those who had stopped using their ADs or prostheses.
Conclusion
Young people with ULRD used ADs more than they used prostheses for facilitating ADL difficulties. Satisfaction with the device-related aspects of ADs was greater than satisfaction with prostheses. Social adjustment of children with ULRD was good. Between ADs and prostheses, young people with ULRD were somewhat better socially adjusted with ADs. Therefore, healthcare professionals should offer ADs as an alternative to prosthetic treatment.
ACKNOWLEDGEMENTS
The authors would like to thank the participants in this study and the pilot for their participation. The rehabilitation centres and professionals are acknowledged for finding participants and sending the questionnaires: Erasmus MC, Rotterdam – Wim Jansen; Revant, Breda – Suzanne Lambregts; St. Maartenskliniek, Nijmegen – Margriet Poelma; Revalidatie Friesland, Friesland – Ingrid de Bruijn; Roessingh, Enschede – Sytske Nawijn; Libra Revalidatie & Audiologie, Blixembosch te Eindhoven – Judit Kleijnen; and De Vogellanden, Zwolle – Yvette van de Laar. Maerian de Jong is acknowledged for reviewing the questions for clarity and age-appropriateness. The authors also thank Ellen Tieben for her support with sending invitation e-mails and Margreet Allema for her help with the graphic design of the questionnaire.
The authors declare no conflicts of interest.
REFERENCES
Appendix I. Description of the questionnaire | |||
Theme | Questions | Response options | Grouping for the analysis |
Demographic characteristics | Age | Complete: day/month/year | 2–< 7 years old; 7–< 13 years old; and 13–20 years old |
Gender | Girl or boy | ||
Education | List of 11 types of education (from daycare to university) | ||
Type of ULRD | Images demonstrating transversal or longitudinal ULRD and self-description of the affected arm | ||
Level of ULRD | Six levels for each left/right hand | ||
Functionality difficulties | ADL combined in ICF domains: self-care: using cutlery, dressing or undressing, tooth brushing, self-washing/taking a shower, using the toilet, tying shoelaces; mobility: riding a bicycle, riding a moped, a scooter or driving; communication: writing, using a computer keyboard; recreation and leisure: doing/engaging in sports, handcrafting, playing a musical instrument, leisure activities; domestic life household activities; and work/employment | Yes; a little; no; not applicable | “difficulties” = ”yes” +”a little” and “no difficulties” = ”no” Domestic life and work/employment were considered as 1 domain |
Use of ADs and prostheses | Reasons for non-use of AD | Multiple | |
Type of prosthesis (if multiple prostheses, answer required for only the one used for a long time or often) | |||
Preferred solutions for ADL | AD; prosthesis; sometimes adaptive device or prosthesis; hand and affected arm and/or other body parts; with help from somebody; and not applicable | ||
Description of 5 ADs | Activity for which AD was used | ||
Appearance | |||
Manufacturer | |||
Last 2 months of use and reasons for use/non-use | |||
Frequency of use | Never; rarely; sometimes; very often; and always | ||
Most important AD | The choice for AD was determined by the participants’ opinion on which AD was most important to them. The subsequent questions were asked specifically for the most important AD and prosthesis (if applicable) | ||
Use of the most important AD/prosthesis | Age of onset | < 5 years old; 5–< 9 years old; 9–< 13 years old; and 13–20 years old | |
Duration | <3 months; half year; 1 year; several consecutive years (number of years); and alternating use, stopped for a while, used again for a period | ||
Location | At home; at home and in environments with acquaintances (at school/family/friends); and everywhere (also in environments with strangers) | ||

Appendix I. Contd. | |||
Theme | Questions | Response options | Grouping for the analysis |
Satisfaction with most important AD/prosthesis | D-Quest devices: dimensions, weight, adjustment, safety, durability, ease of use, comfort, effectiveness, overall. | Not at all satisfied; not satisfied; somewhat satisfied; satisfied; and very satisfied (a box for dissatisfaction reasons) | |
D-Quest rehabilitation services: service delivery, repairs and servicing, professionalism, services, follow-up, overall. | Not at all satisfied; not satisfied; somewhat satisfied; satisfied; and very satisfied (a box for dissatisfaction reasons) | ||
Appearance of the AD/prosthesis (not part of the D-quest). | Not at all satisfied; not satisfied; somewhat satisfied; satisfied; and very satisfied (a box for dissatisfaction reasons) | “somewhat (less) satisfied”= “not at all satisfied”+”not satisfied”+”somewhat satisfied” and “(very)satisfied”=”satisfied”+”very satisfied” | |
Social adjustment with most important AD/prosthesis | TAPES. The social adjustment subscale consisted of four questions: “I don’t care if somebody looks at my prosthesis”, “I find it easy to talk about my prosthesis”, “I don’t mind people asking about my prosthesis”, “I find it easy to talk about my limb loss in conversation.” One question was adapted to accommodate a person with ULRD: “I find it easy to talk about my missing (part of) arm.” The word “adaptive device/” was added before the word “prosthesis” in the questions above. | Strongly disagree; disagree; agree; strongly agree; and not applicable | |
Improvement on the use of ADs | An open question, also asked about suggestions to improve the use of ADs. | Multiple | |
AD(s): adaptive device(s); ULRD: upper limb reduction deficiency; D-Quest: Dutch version of Quebec User Evaluation of Satisfaction with assistive Technology; TAPES: Trinity Amputation and Prosthesis Experience Scale. | |||
Appendix II. Results of logistic regression based on cases with unilateral upper limb reduction deficiency (ULRD), with the use of adaptive devices or prostheses as outcome variable and the participants’ characteristics as predictors | ||||||
Past/present use of ADs or prostheses | Yes | No | β (SE) | p | OR (95% CI) | |
ADsa (all ULRD levels) | n = 154 | n = 47 |
|
|
| |
Age (centred at 2 years old), mean (SD) | 8.1 (4.3) | 8.0 (6.1) | 0.02 (0.04) | 0.651 | 1.02 (0.94; 1.10) | |
Gender (male), n (%) | 92 (59.7) | 26 (55.3) | 0.22 (0.35) | 0.522 | 1.25 (0.63; 2.46) | |
Number of difficulties in ADL, n (%) | 4.4 (2.8) | 3.6 (2.8) | 0.12 (0.07) | 0.079 | 1.13 (0.99; 1.28) | |
ULRD type (transversal), n (%) | 143 (92.9) | 40 (85.1) | 0.89 (0.53) | 0.098 | 2.42 (0.85; 6.91) | |
Constant, n (%) | –0.34 (0.69) | 0.622 | 0.71 (0.18; 2.76) | |||
ADsa,b (ULRD levels higher than the wrist) | n = 96 | n = 28 | ||||
Age (centred at 2 years old), mean (SD) | 8.5 (4.5) | 8.6 (6.0) | 0.06 (0.05) | 0.233 | 1.06 (0.96; 1.17) | |
Gender (male), n (%) | 55 (57.3) | 15 (53.6) | –0.16 (0.47) | 0.730 | 0.85 (0.34; 2.13) | |
Number of difficulties in ADL, n (%) | 4.6 (3.0) | 3.0 (2.5) | 0.22 (0.10) | 0.027* | 1.25 (1.03; 1.53) | |
Transversal ULRD (below-elbow), n (%) | 85 (88.5) | 27 (96.4) | –0.44 (1.12) | 0.696 | 0.65 (0.07; 5.78) | |
Past/present use of prostheses, n (%) | 49 (51.0) | 21 (75.0) | –1.08 (0.54) | 0.045* | 0.34 (0.12; 0.98) | |
Constant, n (%) | 1.05 (1.34) | 0.432 | 2.87 (0.21; 39.82) | |||
Prosthesesa,b (ULRD levels higher than the wrist) | n = 70 | n = 54 | ||||
Age (centred at 2 years old), mean (SD) | 10.0 (4.9) | 6.6 (4.1) | 0.16 (0.05) | 0.001* | 1.18 (1.07; 1.30) | |
Gender (male), n (%) | 33 (47.1) | 37 (68.5) | –0.77 (0.41) | 0.063 | 0.46 (0.21; 1.04) | |
Number of difficulties in ADL, n (%) | 3.8 (3.0) | 4.8 (2.8) | –0.01 (0.07) | 0.934 | 0.99 (0.86; 1.15) | |
Past/present use of ADs, n (%) | 49 (70.0) | 47 (87.0) | –1.25 (0.56) | 0.024* | 0.29 (0.10; 0.85) | |
Constant, n (%) | 0.39 (0.68) | 0.562 | 1.48 (0.39; 5.57) | |||
aOnly young people with unilateral ULRD were included. Age was centred at 2 years old. Reference categories for gender – female, for ULRD type – longitudinal ULRD, for transversal ULRD – above/through-elbow level. bIncluded: 21 participants were with past/present use of a prosthesis, 47 were with past/present use of an AD, 49 were with past/present use of both, and 7 used neither. Excluded: transversal ULRD at the wrist and hand level because prostheses are not prescribed for children with wrist or hand ULRD; and longitudinal ULRD. Due to low cell numbers, the variable “Transversal ULRD” has been excluded from the analysis conducted for prosthetic use. *p<0.05. Percentage calculated from the total number of “Yes” (past/present use of ADs or past/present use of prostheses) or “No” category (never used ADs/never used prostheses). AD(s): adaptive device(s); ULRD: upper limb reduction deficiency; β: coefficient showing weighting of each factor in the model; SE: standard error; p: value showing the significance; OR: odds ratio; 95% CI: 95% confidence interval for the estimated odds ratio; “ever used”: devices that were used in the past or currently. | ||||||

