Amar Awad, MD1,2, Richard Levi, MD, PhD3, Lenita Lindgren, PhD1,2, Claes Hultling, MD, PhD5, Göran Westling, PhD2, Lars Nyberg, PhD1,2,4 and Johan Eriksson, PhD1,2
From the 1Umeå Center for Functional Brain Imaging (UFBI), 2Department of Integrative Medical Biology (Physiology), 3Department of Community Medicine and Rehabilitation (Rehabilitation Medicine), 4Department of Radiation Sciences (Radiology), Umeå University, Umeå and 5Department of Neurobiology, Care Sciences and Society (Neurorehabilitation), Karolinska Institute, Stockholm, Sweden
OBJECTIVE: Neurophysiological investigation has shown that patients with clinically complete spinal cord injury can have residual motor sparing (“motor discomplete”). In the current study somatosensory conduction was assessed in a patient with clinically complete spinal cord injury and a novel methodology for assessing such preservation is described, in this case indicating “sensory discomplete” spinal cord injury.
METHODS: Blood oxygenation level-dependent functional magnetic resonance imaging (BOLD fMRI) was used to examine the somatosensory system in a healthy subject and in a subject with a clinically complete cervical spinal cord injury, by applying tactile stimulation above and below the level of spinal cord injury, with and without visual feedback.
RESULTS: In the participant with spinal cord injury, somatosensory stimulation below the neurological level of the lesion gave rise to BOLD signal changes in the corresponding areas of the somatosensory cortex. Visual feedback of the stimulation strongly modulated the somatosensory BOLD signal, implying that cortico-cortical rather than spino-cortical connections can drive activity in the somatosensory cortex. Critically, BOLD signal change was also evident when the visual feedback of the stimulation was removed, thus demonstrating sensory discomplete spinal cord injury.
CONCLUSION: Given the existence of sensory discomplete spinal cord injury, preserved but hitherto undetected somatosensory conduction might contribute to the unexplained variability related to, for example, the propensity to develop decubitus ulcers and neuropathic pain among patients with clinically complete spinal cord injury.
Key words: fMRI; spinal cord injury; complete; non-conscious; somatosensory cortex.
J Rehabil Med 2015; 47: 426–431
Correspondence address: Johan Eriksson, Department of Integrative Medical Biology (physiology section), Umeå University, SE-901 87 Umeå, Sweden. E-mail: johan.eriksson@umu.se
Accepted Jan 13, 2015; Epub ahead of print Mar 26, 2015
INTRODUCTION
Traumatic spinal cord injury (SCI) is typically a devastating, life-changing event, as it impairs or abolishes conduction of sensory and motor signals across the lesion site, leaving the person severely disabled with paralysis and loss of sensation (1). In order to operationalize and standardize the clinical description of lesions, the International Standards for Neurological Classification of SCI (ISNCSCI) has been adopted and is widely accepted internationally (2). However, as the ISNCSCI is based on a purely clinical assessment, only observable voluntary motor activity and conscious somatosensory perception is evaluated. Thus, any preserved subclinical sensorimotor function cannot be taken into account by the current classification.
Apart from some instances of penetrating trauma, a total anatomic transection of the spinal cord is uncommon (3). By utilizing neurophysiological recordings, Dimitrijevic et al. coined the term discomplete SCI to describe clinically complete lesions accompanied by neurophysiological evidence of residual brain influence on infra-lesional spinal motor function (4, 5). According to their criteria, 84% of the participants with clinically complete SCI had a so-called motor discomplete SCI. However, it is not known whether “discomplete” injuries are of clinical significance. From a neurobiological perspective, the current clinical classification, which dichotomizes lesions into “complete” and “incomplete”, must be considered to be relatively crude and possibly insufficient (6).
To date, few investigations of somatosensory preservation following SCI have been presented, possibly due to a perceived lack of clinical applications. We believe, however, that variability of preserved subclinical somatosensory function may shed light on hitherto unexplained variation in complication patterns in patients with clinically complete SCI. Hypothetically, non-conscious sensory input from infra-lesional body regions may influence behaviour, e.g. by promoting regular pressure relief and bladder emptying, and by triggering spasticity or neuropathic pain.
Preserved motor cortex functionality in SCI patients has been studied extensively, but only a few studies have reported preserved sensory cortex activity related to below-lesion stimulation, which would support the notion of sensory discomplete SCI (7–9). For example, Sabbah et al. (7) investigated sensorimotor cortical activity in patients with clinically complete SCI using functional magnetic resonance imaging (fMRI). With eyes closed, the patients’ feet were inflected by the experimenter, which elicited weak activation “posterior to the central sulcus” in 3 out of 9 patients. Interestingly, 2 additional patients showed sensory activity when the inflection was performed with eyes open. While the possibility of persistent anatomical conduction was postulated, the sensorimotor activity reported in Sabbah’s and other studies could alternatively be driven by other cortical areas rather than by infra-lesional stimulation per se, since the participants were aware of the stimulation events. The mere anticipation of a sensory stimulation can, by itself, activate sensory cortical areas (10, 11). Thus, in order to properly evaluate residual sensory input through a clinically complete SCI, the contribution from cortico-cortical modulation needs to be considered; something that has not previously been attempted. The current study used fMRI to search for evidence of preserved somatosensory function across a clinically complete cervical SCI, and describe a useful methodology for assessing such preservation in a manner that also considers cortico-cortical modulation.
METHODS
Subjects
A 59-year-old, right-handed male with a complete post-traumatic cervical SCI (American Spinal Injury Association Impairment Scale [AIS] grade A) at the C6–C7 level, acquired 29 years previously in a diving accident, was included in Experiments 1, 2 and 3. No zone of partial preservation was present below the neurological level of lesion. The neurological status of the subject was confirmed by an expert spinal cord physician prior to Experiment 1, and was found to be identical to those previously documented in the medical records since 1984. A 24-year-old, right-handed neurologically healthy male participant was included in Experiment 1 in order to verify the experimental protocol and expected outcomes.
Procedure
Experiment 1. In order to evaluate the influence of visual input on activity in somatosensory cortex, Experiment 1 was constructed as a 2×2 factorial design, with somatosensory stimulation (touch or no touch) and vision (presence or absence of visual feedback) as factors. Somatosensory stimulation was applied on the anterior surface of the left upper leg, with and without visual feedback though a tilted mirror attached to the head coil. A touch device was used to guide the experimenter to the required pressure, velocity and onset/offset of the stimulation conditions. During application of skin-to-skin stimulation, the experimenter also applied mirrored stimulations with the contralateral hand to a dummy arm at which forces and movements were measured (perpendicular force = 2.5 N, range 2–3 N; tangential force 2.5 N, range 2–3 N; movement velocity 5 cm/s, range 3–8 cm/s). A stimulation event was defined as a perpendicular force > 0.5 N. A more detailed description of the stimulation procedure and physiological effects from this type of stimulation in healthy volunteers has been published previously (12).
During conditions with no visual feedback, a curtain was pulled in front of the scanner bore to prevent the participants from seeing their own legs. During the condition of no touch but visual feedback, the experimenter moved the hand just above the leg at the same pace as during actual stimulation. Each stimulation lasted for 20 s, followed by a 10 s response period during which the participant was asked to give a verbal evaluation of the sensory experience related to the tactile stimulation, according to the Perceptual Awareness Scale (PAS). PAS is an introspective measure by which participants indicate the experienced intensity of a stimulus (13). Three grades were used: 1 = no experience, 2 = weak experience, and 3 = distinct experience. The verbal reports were given through a magnetic resonance (MR)-compatible microphone. Each condition was repeated 6 times in an unpredictable order, such that each condition was preceded by all other conditions at least once.
Experiment 2. Only the participant with a SCI was included in Experiment 2. Somatosensory stimulation was applied as described in Experiment I, but no visual feedback was provided. The paradigm was instead expanded to include stimulation of the right and left leg (i.e. well below the lesion level), on skin areas with preserved conscious sensation on the right and left arm (i.e. above the lesion level), and also a no-stimulation condition that was used as a reference baseline (corresponding to the “no touch, no vision” condition in Experiment 1). Conditions were repeated 10 times and ordered as in Experiment 1.
During the response period, 2 questions were asked: (i) Did you feel anything? (ii) What body part was stimulated? For the first question the participant used the PAS. However, the subjective evaluation of somatosensory stimulation of the legs was this time not limited to somatic sensations in the legs, but included any sensation whatsoever that appeared to differ from the rest condition, including somatic sensations from other body parts, visual input, etc. For the second question, the participant was asked to guess which body part had been stimulated in the absence of conscious sensation, i.e. a forced-choice response. The questions were presented on a computer screen placed behind the participant’s head outside the scanner bore by using E-Prime 2 (Psychology Software Tools, Sharpsburg, PA, USA). The participant viewed the screen through a mirror mounted on the head coil. Thus, vision was restricted to the screen behind the scanner bore, and the participant could not see his own body. Responses were given using a pistol-grip device in each hand. Due to limited motor function in the fingers, only 1 button per grip could be used, so the 4-alternative (left/right leg/arm) forced-choice response was therefore administered using the following scheme: “left arm” – 1 press with the left button, “right arm” – 1 press with the right button, “left leg” – 2 presses with the left button, “right leg” – 2 presses with the right button.
To eliminate possible confounding effects from top-down cortico-cortical modulation, the participant was blinded as to which body part was being stimulated during the whole experiment. Furthermore, to prevent any movements during leg stimulation from being transmitted to the arms (where the participant could experience sensations) and vice versa, the arms were placed on a table fixed above the participant’s abdomen so that contact between the arms and the legs was prevented during the whole session.
Experiment 3. Only the participant with a SCI was included in Experiment 3. The procedure for Experiment 3 was identical to the procedure for Experiment 2, with the exceptions that 2 conditions were added (stimulation of the left and right foot), each condition was repeated 9 times, and responses (PAS, stimulated body part) were given orally.
Data acquisition
MRI data were obtained with a 3 Tesla GE Discovery MR750 MRI scanner with a 32-channel head coil. Blood oxygenation level-dependent (BOLD) signals were acquired using a T2*-weighted echo-planar imaging sequence covering the whole brain (37 slices, echo time = 30 ms, repetition time = 2 s, flip angle = 80°, matrix size = 96×96, slice thickness = 2.9 mm, field of view = 25 cm, in-plane resolution = 2.6 × 2.6 mm). One functional run was acquired per experiment and participant. The number of image volumes acquired was 510 in Experiment 1, 900 in Experiment 2, and 950 in Experiment 3. Ten dummy scans were run prior to each experimental run to allow the fMRI signal to reach equilibrium.
A high-resolution T1-weighted structural image was collected (TE = 3.2 ms, TR = 8.2 ms, TI = 450 ms and flip angle = 12°). Sagittal T2-weighted images were obtained over the cervical spinal cord (3-mm slice thickness).
Data pre-processing
Data were pre-processed using SPM8 (Wellcome Trust Centre for Neuroimaging, London, UK). All volumes were slice-timing corrected, realigned to the first volume of each time series, and unwarped to account for movement-induced distortions, normalized to the Montreal Neurological Institute (MNI) anatomical space, and smoothed spatially with an isotropic 8-mm full-width at half-maximum Gaussian kernel and high-pass filtered (cut-off = 128 s). Due to relatively large head motion during Experiment 2, we used the ArtRepair toolbox to counteract data distortion. Realigned functional volumes were first motion-adjusted and outlier volumes were replaced by linear interpolation between the closest non-outlier volumes (14).
Statistical analyses
Image analyses were performed offline using the SPM8 software package. Data were analysed voxel by voxel by applying a general linear model (GLM) on the pre-processed data. Analyses were set up by including stimulation conditions as regressors of interest in the GLM, convolved with the canonical haemodynamic response function. Covariates of no interest included the 6 movement parameters, and lower extremity stimulations where answers were omitted, or when the participant reported PAS > 1. The linear regression analyses produced beta-value images for each condition and participant, which were used to calculate t-tests. A statistical threshold of p < 0.001, cluster size k ≥ 20, was considered significant. Exceptions due to a priori hypotheses of effect locations are explicitly stated in the text.
RESULTS
Experiment 1
Consistent with previous research (12), stimulation on the left upper leg of the healthy control participant correlated with a BOLD signal change in bilateral post-central gyrus (S1) extending posteriorly into the superior parietal lobule (BA5), supramarginal gyrus (S2), insula, and the right anterior cingulate cortex (ACC; main effect of touch, Fig. 1a and b). The main effect of vision overlapped with the main effect of touch in S1, S2, and insula, demonstrating the potency of visual input to modulate the BOLD response in the somatosensory cortex. Furthermore, there was a significant touch-by-vision interaction in S1, S2, and insula, where visual input alone produced a larger increase in S1 BOLD signal than the effect from combined somatosensory and visual input (Fig. 1c). Post-experiment debriefing indicated that the participant on some occasions experienced sensations from the stroke of the hand across the cutaneous hairs. Thus, combined somatosensory and visual input may have been synergistic for the “visual input without touch” condition for the healthy participant.
The SCI participant reported no somatosensory perception following stimulation of the upper left leg (PAS = 1 on all trials), thus confirming the clinically complete SCI (AIS grade A). However, despite the lack of conscious sensations, the main effect of touch did elicit BOLD signal change in bilateral S1 and BA5, left S2, bilateral anterior insula, and left ACC (Fig. 1a and b). The main effect of vision overlapped with the effect of touch in bilateral S1, left S2, and right anterior insula. Moreover, there was a significant touch-by-vision interaction in bilateral S1 and right anterior insula, demonstrating a synergy from combined somatosensory and visual input (Fig. 1c). Critically, touch in the absence of visual input produced BOLD signal change in S1 within the areas displaying the main effect of touch, but at a lower level of significance (t = 2.45, p = 0.008; Fig. 1c), indicating partially preserved somatosensory conduction despite the AIS grade A clinical diagnosis.
Experiment 2
In line with previous research (15), the results from Experiment 1 demonstrated that visual input can modulate the BOLD signal in the somatosensory cortex. To verify whether touch alone could produce BOLD signal change in the SCI participant, we ran a second experiment in which care was taken to ensure that the participant could not know when the leg was being touched (see Methods). Also, we expanded the stimulation conditions to include the right leg and areas above the lesion level (in both arms proximal to the sensory lesion level). No visual feedback was provided during Experiment 2.
The SCI participant had nearly normal perception of arm stimulation, reporting slightly weaker sensory function in the left arm compared with the right. Stimulation of the arms was associated with somatosensory sensations (PAS = 3) and left/right judgments close to 100% correct, with the exception of 6 responses that were verified during debriefing as unintentional button presses (4 left/right judgments and 2 PAS responses; the participant reported some difficulty in using the pistol-grip buttons due to diminished hand function). Somatosensory stimulation of the left and right arm produced significant BOLD signal change in right and left S1, respectively (Fig. 1d). BOLD signal during left-arm stimulation was less pronounced relative BOLD signal during right-arm stimulation, probably reflecting the slightly oblique clinical lesion level, with more pronounced deficits in the left arm.
The subjective evaluation of somatosensory stimulation of the legs during Experiment 2 (PAS) was not limited to somatic sensations in the legs, and the participant was instructed to report any sensation whatsoever that appeared to differ from rest, including somatic sensations from other body parts, visual input, etc. During leg stimulation, all but 2 PAS responses were “1”. Two responses were “2”, and the related BOLD signal from these responses was excluded from further analysis (see Methods). After the scanning session, the participant could not explain why he had given these PAS=2 answers. He confirmed, however, that they were not related to any somatosensory perception per se. When asked to guess which leg was stimulated, the participant did not perform better than chance (55%, p = 0.82, binomial test, trials with PAS = 2 included). Thus, the participant was not consciously aware of the leg stimulations according to both subjective and objective criteria (16). Nevertheless, stimulation of the left upper leg again produced significant BOLD signal change in BA5 bilaterally (Fig. 1d). Moreover, stimulation of the right upper leg produced significant BOLD signal change in BA5 and S2 bilaterally.
Experiment 3
In Experiment 3 the protocol was further extended to also include stimulation of the feet. For stimulation of the arms, all subjective ratings were PAS = 3 and performance was 100% correct regarding which body part was stimulated. Left and right arm stimulation evoked BOLD signal change in contralateral S1 for each arm, and left S2 for both arms (Fig. 1e).
For stimulation of the legs, most subjective ratings were PAS = 1 (13/18). Two responses were “2” and 3 were missing (no response made within the designated time-window). Body-part judgment (left/right foot or left/right leg) was no better than chance (27%, p = 0.54, binomial test against a 0.25 distribution). When the left leg was stimulated, there was a significant BOLD signal change in bilateral S1 (Fig. 1e). Right leg stimulation gave rise to a less significant BOLD signal change in left S1, though it was consistent with expected topology (t = 2.36, p = 0.01, Fig. 1f).
For stimulation of the feet, most subjective ratings were PAS = 1 (16/18, 1 “2” and 1 missing) and body-part judgment was no better than chance (12%, p = 0.16, binomial test against a 0.25 distribution). Stimulation of the right foot produced significant BOLD signal change in left S1 (Fig. 1e), whereas stimulation of the left foot was associated with less significant BOLD signal change, which was located in the ipsilateral S1 (t = 2.23, p = 0.02).
Structural imaging of the spinal cord
Inspection of the T2-weighted image of the SCI participant’s spinal cord revealed a severe structural lesion at the C6/C7 level, but also some apparent spinal cord tissue continuity bridging the lesion (Fig. 1g).
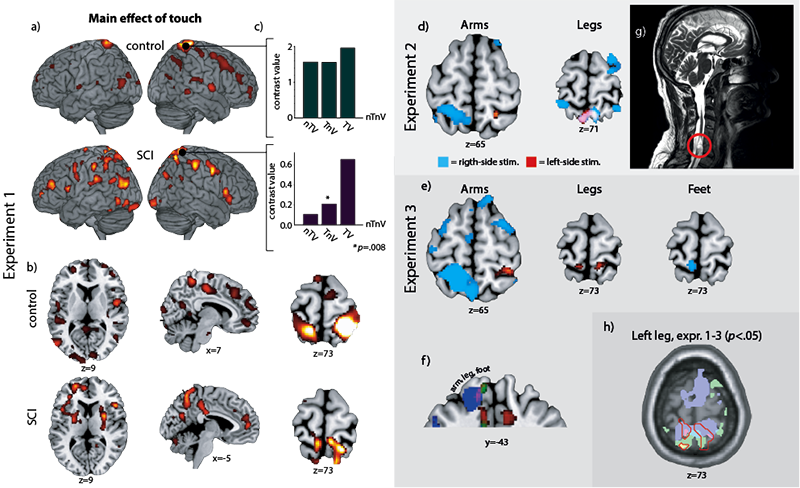
Fig. 1. Overview of functional magnetic resonance imaging (fMRI) results. (a) Both the healthy control and the spinal cord injury (SCI) participant had significant blood oxygenation level-dependent (BOLD) signal changes in S1, S2, insula and anterior cingulate cortex (ACC), and several other areas (b), related to the main effect of touch. (c) Bar graphs show contrast values in S1 for the conditions “no touch, vision” (nTV), “touch, no vision” (TnV), and “touch and vision” (TV), compared with the “no touch, no vision” (nTnV) baseline. Critically, the TnV condition was associated with significant BOLD signal change for the SCI participant. (d) In Experiment 2, stimulation of the right (blue colour) and left (red colour) arms produced BOLD signal changes in contralateral S1. Stimulation of the legs produced similar, but less lateralized, signal changes in BA5. (e) Results from Experiment 2 were replicated in Experiment 3, and extended with foot stimulation resulting in BOLD signal change in S1. Stimulation of the right leg produced weaker signal change in contralateral S1, but in a topographically appropriate location. (f) The different body parts are illustrated using different thresholds, such that arm and foot are shown with p < 0.001, whereas the leg is shown with p < 0.05, uncorrected. (g) T2-weighted image showing a potential sparing of the dorsal spinal cord (circled). (h) BOLD signal change from stimulation of the left leg in Experiments 1 (red, overlap with green is yellow, overlap with blue is pink), 2 (green, overlap with blue is turquoise) and 3 (blue), with the main effect of touch (Experiment 1) outlined in red, demonstrating overlap across experiments in S1 and BA5. Note: Left is left and right is right in all brain images.
DISCUSSION
Tactile stimulation of the left upper leg elicited BOLD signal change in somatotopically appropriate parts of S1/BA5, as well as in S2, insula and right ACC in the participant with SCI, despite the AIS grade A classification. These responses were comparable to those obtained in the healthy control participant. These findings demonstrate that somatosensory cortex function is, to some degree, maintained after more than 29 years without any conscious sensation from the lower extremities. Importantly, visual feedback of the somatosensory stimulation modulated BOLD signal in overlapping regions in both the able-bodied and the SCI participant, highlighting the significance of taking top-down effects into account when evaluating sensory input (i.e. bottom-up processes). Critically, even when tactile stimulation was applied on the SCI participant while excluding top-down effects, there were significant BOLD signal changes in the somatosensory cortex. Thus, the current results demonstrate a case of sensory discomplete SCI, where the residual conduction of somatosensory signals is not sufficient to give rise to conscious sensory experiences, but nevertheless elicit cortical responses.
The activity in the somatosensory cortex in the participant with SCI might be a result of residual somatosensory fibre connections to the brain either bypassing the lesion or going through it, as suggested by the T2-weighted spinal cord image (Fig. 1g). The location of the tissue continuity, running dorsally in the spinal cord, might indicate that it is part of the posterior column-medial lemniscus pathway, although differentiation between nerve and scar tissue is not possible by this method. As it is generally rare for the spinal cord to be anatomically transected by closed spinal trauma (3), it might not be unusual to find residual physiological or anatomical continuity of central nervous system tracts across what clinically are classified as complete lesions. Subclinical preserved conduction of somatosensory impulses, like the one observed here, speculatively might contribute to the hitherto largely unexplained variations in the prevalence of post-traumatic conditions such as excessive spasticity and neuropathic pain, why some tetra- and paraplegic subjects experience semen extraction procedures as pleasurable while others do not, and the unexplained variations in prevalence of complications such as decubitus ulcers and incontinence within the category of patients with clinically complete injuries.
Decubitus ulcers are a common and serious secondary complication of SCI (17). The completeness of the SCI is a major risk factor for developing decubitus ulcers (18). Patients with complete injuries (AIS grade A) are associated with a higher risk of developing pressure ulcers, partially as a result of these individuals’ inability to feel pain in a pressure area (sensory loss) and inability to alternate position naturally (motor loss) (6, 19). Approximately two-thirds of patients with SCI AIS grade A develop decubitus ulcers (6). One explanation for rehabilitative training success and rarely developing decubitus ulcers for the remaining one-third could be coupled to residual communication between the brain and the body parts innervated below the injury level. Albeit insufficient to give rise to a conscious sensory experience, such neural impulses may alter behavioural patterns toward more protective activities, such as frequently alternating position and avoiding prolonged positional immobilization. The lack of conscious perception does not exclude the possibility that such non-conscious sensory input nevertheless influences behaviour adaptively (20).
Neuropathic pain is another major cause of disability and a significant problem following SCI (21). Two main types of neuropathic pain are observed following SCI: at-level (corresponding to the segment of injury); and below-level (corresponding to segments below the segment of injury) neuropathic pain (22). The mechanisms of spontaneous below-level SCI pain are not entirely understood, despite a large number of theories about the underlying pathology (23). Wrigley et al. investigated the association between neuropathic SCI pain and somatosensory cortical reorganization, finding that cortical reorganization was correlated with pain intensity (24). Thus, preserved somatosensory conduction, as we have seen in our participant, may contribute to maintaining somatotopic organization in S1 and might add to the underlying biological variability that explains why some patients with clinically complete SCI experience neuropathic pain while others do not.
The results of BOLD signal change in somatosensory cortex from tactile stimulation were replicated across the 3 experiments, but in no situation did the stimulation below the level of injury evoke conscious sensory experiences. While the neural correlates of conscious experiences remain unclear, a common observation is co-activation of both sensory and frontoparietal regions specifically during conscious perception (25). Although the main effect of touch during Experiment 1 did produce signal changes in sensory and frontoparietal regions (Fig. 1), no consistent signal change was seen in frontoparietal regions during stimulation of lower extremities when controlling for top-down effects. It is possible that lack of such sensory-frontoparietal co-activation may explain the absence of conscious sensory experiences despite significant BOLD signal change in the sensory cortex. However, no consistent frontoparietal activity was seen during stimulation of the arms either, although such stimulation was associated with clear sensations. Correspondingly, it has been suggested that sensory-frontoparietal co-activation is only necessary for consciousness in situations where perception is difficult or ambiguous (26). Thus, it remains unclear what would be required for the residual somatosensory signals to be accompanied by conscious sensory experiences.
This study is based on a single case, which limits the possibility to generalize our conclusions. Nevertheless, the demonstration of preserved somatosensory conduction across a clinically complete lesion falsifies the assumption that a clinically complete spinal lesion always entails a complete functional discontinuity between the body parts below the lesion and the brain. We propose, therefore, that sensory discomplete lesions are at least a possibility among patients classified as somatosensory complete. Thus, our findings should encourage larger-scale studies examining the somatosensory system in patients with clinically complete SCI. It is possible that the present clinical SCI classification could be refined to also include a motor and/or sensory discomplete subcategory within the present AIS A category.
In summary, we found that, in a patient with a clinically complete cervical SCI, somatosensory stimulation applied on dermatomes innervated below the SCI gave rise to BOLD signal changes in the corresponding areas of the somatosensory cortex. These findings indicate preserved nerve impulse communication between body parts innervated by segments located below the lesion and the brain. Albeit insufficient to give rise to a sensory experience, this preserved somatosensory conduction is presumably reaching the brain and might contribute to explain behavioural variability and the risks of developing complications, such as decubitus ulcers and neuropathic pain, within the category of patients who are currently classified as having complete injuries.
ACKNOWLEDGEMENTS
This research was supported by grants from Torsten and Ragnar Söderberg’s Foundation (LN), the Swedish Research Council (JE), and the medical faculty at Umeå University (LL). We thank the MR staff for assistance during scanning, and Micael Andersson for data analyses support.
REFERENCES

