Ellen Marie Bardal, PhD1, Karin Roeleveld, PhD1 and Paul Jarle Mork, PhD2
From the 1Department of Neuroscience and 2Department of Public Health and General Practice, Norwegian University of Science and Technology, Trondheim, Norway
OBJECTIVE: To investigate whether moderate intensity endurance exercise has similar effects on cardiovascular fitness and autonomic function in patients with fibromyalgia and healthy controls.
DESIGN: Case-control intervention study.
SUBJECTS: Twenty-five female patients with fibromyalgia and 25 age- and sex-matched healthy controls (age range 40–64 years) were recruited to the study. Fifteen patients and 19 controls participated at both pre- and post-test.
METHODS: Supervised spinning workouts of moderate intensity (~75% of age-predicted maximum heart rate) were performed twice a week for 12 weeks. Cardiovascular fitness was evaluated by an incremental ergometer cycling test to anaerobic threshold. Autonomic function was assessed by heart rate recovery after exercise, resting blood pressure, and resting heart rate variability. Pain was scored on a visual analogue scale, while overall symptom level was assessed by the Fibromyalgia Impact Questionnaire.
RESULTS: Linear regression analysis with adjustments for baseline level and attendance rate showed a similar dose-dependent increase in patients and controls in oxygen uptake and workload after the 12-week intervention. Indices of autonomic function remained unchanged in both groups. Neck/shoulder pain decreased in patients, while overall symptom level remained unchanged.
CONCLUSIONS: Female patients with fibromyalgia have similar cardiovascular adaptations to moderate intensity endurance exercise as healthy controls.
Key words: fibromyalgia; chronic pain; aerobic exercise; physical fitness; blood pressure.
J Rehabil Med 2015; 47: 639–646
Correspondence address: Paul Jarle Mork, Department of Public Health and General Practice, Norwegian University of Science and Technology (NTNU), NO-7491 Trondheim, Norway. E-mail: paul.mork@ntnu.no
Accepted Feb 9, 2015; Epub ahead of print Jun 1, 2015
INTRODUCTION
Fibromyalgia (FM) is a chronic pain syndrome that often involves comorbid symptoms, such as sleep disturbance, undue fatigue, headache, psychological disorders and gastrointestinal disorders (1, 2). The prevalence of FM in the general adult population is approximately 3–5%, with a 3- to 7-fold higher prevalence among women than men (3, 4). Research indicates that the aetiology of FM involves deficiencies in the regulation of the autonomic nervous system and the hypothalamic-pituitary-adrenal axis (5–7), along with altered central pain processing (8, 9). Deconditioning and physical inactivity are commonly reported in FM (10–13), and it has been hypothesized that a deficit in autonomic regulation is partly explained by poor physical fitness (7).
Several randomized controlled trials have shown that physical exercise has a positive effect on pain and physical fitness in patients with FM (14–18); however, few studies have investigated whether an increase in physical fitness in these patients is associated with improved autonomic function. A research group investigated the effect of resistance exercise on resting heart rate variability (HRV) as a measure of autonomic function in patients with FM (19, 20). Progressive whole-body resistance exercise was carried out twice a week for 16 (19) or 12 weeks (20), respectively, and included comparable training loads, i.e. 8–12 repetitons progressing from approximately 50% to 80% of 1 repetition maximum during the intervention period. The 2 studies reported conflicting results, i.e. improved (19) and unchanged (20) HRV.
Regarding the effect of endurance exercise, there is ample evidence showing that cardiovascular fitness improves in patients with FM, provided that the exercise programme fulfils minimum recommendations to maintain or improve cardiovascular fitness (14). However, the effect of endurance exercise on cardiovascular fitness has been assessed by comparing groups of exercising and non-exercising patients (14–17). It is therefore unknown whether patients with FM display similar cardiovascular adaptations to endurance exercise as those of healthy subjects. Morever, there is a lack of studies investigating whether endurance exercise is associated with improved autonomic function in patients with FM. In healthy subjects, there is some evidence showing a positive effect of moderate intensity endurance exercise on autonomic function (21). Moderate intensity endurance exercise is commonly defined as exercise intensity at approximately 70% of maximum heart rate (22), and studies have shown that this type of exercise is well tolerated by patients with FM (23).
The aim of the present study was to investigate whether moderate intensity endurance exercise has a similar effect on cardiovascular fitness and indices of autonomic function in female patients with FM and in age- and sex-matched healthy controls (HCs). Our hypothesis was that patients with FM would display similar aerobic and cardiovascular autonomic adaptations to moderate intensity endurance exercise as those of HCs.
METHODS
Subjects
Twenty-five female patients with FM and 25 age- and sex-matched HCs were included in the study. The patients were recruited through the local FM association and through advertisements in the local newspaper. HCs were recruited among university staff and through advertisements in the local newspaper. Inclusion criteria were that participants should not exercise on a regular basis, but had to confirm that they were able to perform moderate intensity endurance exercise on a spinning bike and participate in group sessions. Exclusion criteria were: (i) cardiorespiratory, cerebrovascular, neurological, neuromuscular, endocrine, infectious, metabolic, lung, or cancer disease; (ii) injury that affected function; (iii) connective tissue disorder; (iv) high blood pressure (i.e. systolic pressure > 140 mmHg or diastolic pressure > 90 mmHg) or taking anti-hypertensive medication; or (v) if they were taking medication that might interact with neural, vascular, or muscular function or the physiological measurements to be performed (e.g. antidepressants, anti-epileptics, β-blockers). Twenty-eight patients and 35 HCs volunteered to participate in the study. Based on a pre-screening phone interview about health status, medication and exercise status, 3 patients were excluded due to other disease and medication (see exclusion criteria), 5 HCs were excluded due to exercise status, and 5 HCs were excluded because their age did not match the patient sample. The remaining 25 patients underwent a clinical examination upon inclusion in the study in order to verify the FM diagnosis as defined by the American College of Rheumatology (24). The study protocol was approved by the Regional Committee for Ethics in Medical Research (project number 4.2008.2115) and all subjects signed an informed consent before enrolment. The study was carried out according to the principles of the Declaration of Helsinki.
Test procedure
The pre- and post-test procedure was identical. Aerobic and anaerobic thresholds were estimated using an incremental cycling test (25, 26). The test was performed with the subject seated upright on a computer-controlled cycle ergometer (939 E, Monark, Vansbro, Sweden), which generates constant power independent of cadence. Heart rate (HR; Polar RS800, Polar, Kempele, Finland) and gas exchange variables (Metamax® MMX II 1.0, Cortex Biophysik GmbH, Leipzig, Germany) were recorded continuously throughout the test. The VO2 and VCO2 gas analysers were calibrated before each test day using high-precision gases (16.00 ± 0.04 O2 and 5.00 ± 0.01 CO2, Riessner-Gase GmbH & Co, Lichtenfels, Germany) while the inspiratory flow meter was calibrated with a 3 L volume syringe (Hans Rudolph Inc., Kansas City, MO, USA). The test started with a 6-min warm-up period of steady state low-intensity cycling, followed by a stepwise increase in workload (10 W/min) until blood lactate concentration (bLa) reached >5 mmol/l (Fig. 1). bLa was measured for each workload and at the end of the test in 5 µl blood samples taken from the fingertip using lactate Pro LT-1710t (ArkRay Inc., Kyoto, Japan). Subjects were also asked to rate their physical exertion on Borg’s scale of perceived exertion (RPE) for every increase in workload (27). The exertion scale ranges from 6 (no exertion at all) to 20 (maximal exertion). The scale values are thought to denote heart rates ranging from 60 to 200 beats/min, and a score of 13 would indicate an exertion denoted as “somewhat hard” or “moderate” (heart rate ~130 beats/min), while a score of 15 would correspond to “hard” (heart rate ~150 beats/min).
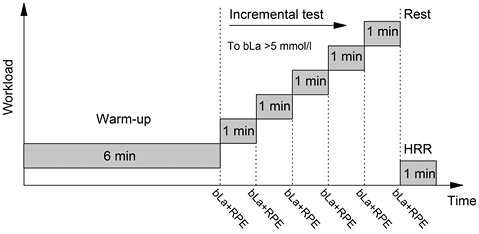
Fig. 1. Protocol for testing of aerobic capacity and heart rate recovery (HRR). The warm-up period with steady state low-intensity cycling was followed by a stepwise increase in workload (10 W/min) until blood lactate concentration (bLa) reached > 5 mmol/l. Rate of perceived exertion (RPE) was noted for every increase in workload.
Prior to further analysis, HR and gas exchange variables were averaged over the last 30 s of each workload. Anerobic threshold (AT) was defined as bLa = 4 mmol/l and AT values for HR, gas exchange variables and workload were estimated by interpolation of bLa (26). The aerobic response at AT was used as an indicator of cardiovascular fitness, since previous studies have shown that patients with FM are unable to reach maximal oxygen consumption (10, 28). The use of bLa = 4 mmol/l as a definition of AT does not necessarily reflect the real AT in all subjects, but gives a reliable reference of intensity to compare pre- and post-test measurements (26). Furthermore, the 1st and 2nd ventilatory threshold (VT) were estimated by the slope of the curves of the ventilatory equivalents of oxygen and carbon dioxide (29) and used to determine the individual exercise intensity (cf. exercise programme, described below).
Measurements of HRV, HR recovery (HRR), and blood pressure were used as indices of autonomic function. HRR was calculated as the decrease in HR during the first minute after termination of the incremental cycle test with subjects sitting erect on the bike. For calculation of HRV, electrocardiography (ECG) was recorded (Delsys Myomonitor IV, Boston, USA) with a sample frequency of 1000 Hz during 30 min of supine rest. The subjects were instructed to relax, but not fall asleep during the rest period. The environment was calm with dimmed lights and a room temperature of 23ºC.
HRV was analysed with LabChart software (AD Instruments, Oxford, UK). R–R intervals were extracted from the detected QRS complex. Normal-to-normal (NN) heart beat intervals were thereafter extracted by omitting all intervals that resulted from ectopics or artefacts (non-sinus beats). The standard deviation of the NN intervals (SDNN), the root mean square successive difference (RMSSD), and the low-frequency (LF; 0.04–0.15 Hz) and high-frequency (HF; 0.15–0.4 Hz) heart period power spectra were calculated for the last 5 min of the 30 min supine rest period. Blood pressure (Heine, Gamma XXL LF, Germany) was measured in supine position at the end of the 30 min resting period.
Pressure pain threshold (PPT) was measured with a Somedic type II digital algometer (SBMEDIC Electronics, Solna, Sweden) with a probe size of 1 cm2. The subjects were informed that the investigation aimed at determining PPT and not pain tolerance. PPT was measured bilaterally at the suboccipital muscle insertion, origin of supraspinatus, medial border of trapezius, rectus femoris tendon 1 cm proximal of patella, and belly of rectus femoris 8 cm proximal of patella. The probe of the algometer was held perpendicular to the skin surface and the pressure was increased by 40 kPa/s. The subjects were instructed to press a button when the pressure started to be painful, upon which the pressure was immediately released. Subjects were seated during all PPT measurements and the mean of 2 successive measurements was used to determine PPT at each site. The PPTs from the suboccipital muscle insertion, supraspinatus, and trapezius were thereafter averaged to indicate a PPT score for the upper body, while the PPTs recorded at the rectus femoris tendon and belly was used to indicate a PPT score for the lower body.
All subjects answered questionnaires on pain intensity and physical activity. Pain intensity in the neck/shoulders and low back were assessed by visual analogue scale (VAS; 0–100 mm) anchored by “no pain at all” and “worst pain imaginable”. VAS scores were obtained before and after each exercise session and at the pre- and post-test. Physical activity level was estimated using the Norwegian short version of the International Physical Activity Questionnaire (30). In addition, the FM patients were asked to complete the Fibromyalgia Impact Questionnaire (FIQ) at the pre- and post-test to assess the severity of FM symptoms (31).
Exercise programme
The exercise programme consisted of supervised spinning workouts of moderate intensity performed twice a week for 12 weeks. Exercise intensity zones were defined for each subject according to the VTs determined during the pre-test (26). HR limits were determined for the low lactate zone (below 1st VT), lactate accommodation zone (between 1st and 2nd VT), and lactate accumulation zone (above 2nd VT). The 1st VT corresponds to 50–58% of maximal oxygen consumption (VO2max) and the 2nd VT to 75% of VO2max in sedentary adults (26). Each exercise session lasted from 45 to 60 min and consisted of a warm-up period (~10 min), 3–4 intervals (~8–10 min) separated by 2-min active rest, and an active cool-down period of 3–5 min. The target exercise intensity of the intervals was between 1st and 2nd VT, while the target intensity of the warm-up and active rest periods was at or slightly below the 1st VT. The relative exercise intensity and the length of the interval periods was the same throughout the intervention period. To assure adherence to the target intensity all training sessions were monitored with HR monitor watches, frequent random samples of bLa and subjective assessments of RPE.
Statistical analysis
Descriptive statistics, including mean and standard deviation (SD), are reported for the main outcome variables. The FIQ score is presented as median with interquartile range (IQR). The independent samples t-test was used for group comparisons, while the paired samples t-test was used for within-subject comparisons. Spearmans rho or Pearson’s r was used to assess correlations between variables. Linear regression analysis with adjustments for baseline level and attendance was used to calculate β-coefficients for the change in indices of cardiovascular fitness and autonomic regulation per exercise session. A general linear model was used to test interaction between attendance and group, i.e. to test the hypothesis that changes occurring due to the intervention did not differ between patients and HCs. Baseline level was included as covariate in all interaction analysis. Statistical analyses were performed using SPSS statistical programme for Windows (version 20.0). Statistical significance was set at p < 0.05 for all analysis.
RESULTS
Drop-outs from the exercise programme
Eight patients and 6 controls dropped out of the exercise programme. Two patients dropped out due to worsening of pain and undue fatigue during the initial 2–3 weeks. In addition, 5 patients (1 wrist fracture, 1 worsening of chronic pelviolysis, 1 viral infection, 1 symptoms of arrhythmia, and 1 intestinal catarrh) and 1 HC (mononucleosis) dropped out due to other conditions or diseases. One patient and 5 HCs dropped out due to personal reasons not related to FM symptoms or other somatic diseases. One patient was excluded from further analysis due to poor quality of the post-test spirometric data. Consequently, data from 15 patients and 19 HCs were available for comparisons of the pre- and post-test results (Table I). There was no difference in age or physical activity level between the patients and HCs who participated at both the pre- and post-test.
|
Table I. Characteristics the patients with fibromyalgia (FM) and healthy controls (HCs) participating at pre- and post-test |
|||
|
Characteristic |
FM (n = 16) |
HCs (n = 19) |
p-value |
|
Age, years, mean (SD) [range] |
54 (7.3) [40–63] |
52 (8.8) [40–64] |
0.35 |
|
IPAQ, MET, mean (SD) [range] |
1,509 (946) [330–3,066] |
1,619 (1,228) [231–3,930] |
0.79 |
|
BMI, kg/m2, mean (SD) [range] |
28.1 (3.4) [21–33] |
25.7 (3.4) [19–32] |
0.06 |
|
Body mass, kg, mean (SD) [range] |
75.4 (9.2) [63–92] |
71.9 (10) [54–86] |
0.31 |
|
FIQ score, median (IQR) |
51.9 (21.6) |
NA |
|
|
Years since diagnosis, mean (SD) |
8.3 (6.5) (1–20) |
NA |
|
|
BMI: body mass index: FIQ: Fibromyalgia Impact Questionnaire; IPAQ: International Physical Activity Questionnaire; IQR; interquartile range; MET: metabolic equivalent; NA: not applicable. |
|||
Attendance and exercise intensity
Table II shows attendance rate and exercise intensity during the spinning workout sessions. Attendance rate did not differ between patients and HCs, but varied considerable within groups. Attendance was significantly correlated with pre- to post-test improvements in VO2 (r = 0.58, p = 0.03) and workload (r = 0.61, p = 0.02) at AT in patients (data not shown). A similar tendency was observed in HCs for VO2 (r = 0.39, p = 0.09) and to a lesser extent for workload (r = 0.35, p = 0.15). Exercise intensity during the spinning sessions, indicated by HR calculated as percent of pre-test 2nd VT or age-predicted maximum HR (i.e. 220-age), did not differ between groups. Likewise, there was no group difference in the RPE scored at the exercise sessions.
|
Table II. Attendance rate and exercise intensity in patients with fibromyalgia (FM) and healthy controls (HCs) |
|||
|
FM (n = 16) Mean (SD) [range] |
HCs (n = 19) Mean (SD) [range] |
p-value |
|
|
Attendance rate (%) |
71 (26) [20–100] |
81 (28) [16–100] |
0.30 |
|
Exercise intensity (%HR 2nd VT) |
91 (5.5) [84–99] |
89 (4.5) [80–98] |
0.37 |
|
Exercise intensity (%HRmax)* |
74 (6.4) [62–88] |
78 (8.2) [64–91] |
0.13 |
|
Rate of perceived exertion |
13.7 (2.0) [9.9–17.0] |
13.6 (1.2) [11.5–15.4] |
0.91 |
|
*Age-predicted HRmax. AT: anaerobic threshold; HR: heart rate; VT: ventilatory threshold. |
|||
Aerobic capacity characteristics
Table III shows aerobic capacity characteristics at AT for patients and HCs at the pre- and post-test, crude difference between the pre- and post-test, and adjusted mean change per exercise session. VO2 tended to be lower in patients compared with HCs at the pre-test, while post-test values of VO2 and both pre- and post-test values of workload were significantly lower in patients. The adjusted mean change in VO2 and workload were significant in patients and tended to be significant in HCs. Tests of interaction (attendance × group) showed no evidence of difference between patients and HCs in the adjusted mean change in VO2 (p = 0.60) or workload (p = 0.28). Adjusted HR and RPE remained unchanged and, accordingly, there was no difference between groups in the mean change per exercise session (p-value for interaction ≥ 0.20 for both associations).
|
Table III. Effect of endurance exercise on aerobic capacity characteristics at anaerobic threshold (i.e. blood lactate concentration = 4 mmol/l) in patients with fibromyalgia (FM) and healthy controls (HCs) |
||||||||
|
Pre-test Mean (SD) |
Post-test Mean (SD) |
Crude difference (pre-post) |
p-value (crude difference) |
Adjusted mean change per exercise session* |
95% CI |
p-value (adjusted mean change) |
||
|
VO2 (l/min) |
||||||||
|
FM |
1.45 (0.28) |
1.52 (0.26) |
0.08 |
0.07 |
0.013 |
0.004 to 0.023 |
0.01 |
|
|
HCs |
1.64 (0.29) |
1.78 (0.28) |
0.14 |
0.001 |
0.010 |
–0.001 to 0.020 |
0.08 |
|
|
p-value |
0.07 |
0.01 |
0.20 |
|||||
|
Workload (W) |
||||||||
|
FM |
68.5 (21.8) |
77.1 (24.0) |
8.5 |
0.04 |
1.35 |
0.22 to 2.48 |
0.02 |
|
|
HCs |
84.8 (22.6) |
98.5 (23.2) |
13.3 |
< 0.001 |
0.67 |
–0.14 to 1.47 |
0.09 |
|
|
p-value |
0.04 |
0.01 |
0.26 |
|||||
|
HR (bpm) |
||||||||
|
FM |
134 (13.7) |
134 (12.1) |
0.27 |
0.91 |
0.43 |
–0.31 to 1.16 |
0.23 |
|
|
HCs |
140 (17.1) |
143 (15.7) |
2.63 |
0.22 |
0.38 |
–0.15 to 0.91 |
0.15 |
|
|
p-value |
0.25 |
0.09 |
0.46 |
|||||
|
RPE (6–20) |
||||||||
|
FM |
14.7 (2.5) |
15.0 (2.5) |
0.32 |
0.45 |
0.06 |
–0.09 to 0.21 |
0.40 |
|
|
HCs |
14.2 (1.5) |
14.4 (1.2) |
0.28 |
0.68 |
–0.04 |
–0.13 to 0.04 |
0.27 |
|
|
p-value |
0.51 |
0.35 |
0.80 |
|||||
|
*Adjusted for attendance and baseline level. CI: confidence interval; HR: heart rate; bpm: beats per min; RER: respiratory exchange ratio; RPE: rate of perceived exertion; VO2: oxygen consumption; W: watt. |
||||||||
Cardiovascular autonomic function
Table IV shows HRR, blood pressure (systolic and diastolic) and HRV (SDNN, RMSSD, and LF/HF ratio) at the pre- and post-test, crude difference between the pre- and post-test, and adjusted mean change per exercise session. Baseline diastolic blood pressure was higher in patients, while systolic blood pressure, HRR and HRV did not differ between groups. Both the crude and adjusted analyses indicated that all indices of cardiovascular autonomic function remained essentially unchanged in both patients and HCs. Tests of interaction (attendance × group) indicated no difference between patients and HCs in the adjusted mean change in HRR, blood pressure, or HRV (p-value ≥ 0.13 for all associations).
|
Table IV. Effect of endurance exercise on heart rate recovery (HRR), blood pressure (BP) and heart rate variability (HRV) in fibromyalgia patients (FM) and healthy controls (HCs) |
||||||||
|
Pre-test Mean (SD) |
Post-test Mean (SD) |
Crude difference (pre-post) |
p-value (crude difference) |
Adjusted mean change per exercise session* |
95% CI |
p-value (adjusted mean change) |
||
|
HRR |
||||||||
|
FM |
–29 (11) |
–28 (12) |
0.6 |
0.77 |
0.1 |
–2.0 to 2.2 |
0.95 |
|
|
HCs |
–33 (9.5) |
–35 (6.9) |
–2.5 |
0.13 |
0.4 |
–0.8 to 1.7 |
0.45 |
|
|
p-value |
0.36 |
0.07 |
0.23 |
|||||
|
Systolic BP |
||||||||
|
FM |
125 (14) |
117 (14) |
–7.5 |
0.11 |
2.1 |
–0.8 to 5.0 |
0.14 |
|
|
HCs |
117 (8.1) |
113 (11) |
–4.0 |
0.09 |
–0.4 |
–2.6 to 1.8 |
0.72 |
|
|
p-value |
0.10 |
0.42 |
0.42 |
|||||
|
Diastolic BP |
||||||||
|
FM |
76 (10) |
73 (7.0) |
–3.0 |
0.21 |
–0.1 |
–1.5 to 1.5 |
0.97 |
|
|
HCs |
68 (6.6) |
69 (7.6) |
1.7 |
0.27 |
–0.4 |
–1.8 to 1.1 |
0.59 |
|
|
p-value |
0.01 |
0.19 |
0.08 |
|||||
|
SDNN |
||||||||
|
FM |
54 (30) |
58 (30) |
3.8 |
0.51 |
–2.2 |
–7.1 to 2.6 |
0.30 |
|
|
HCs |
55 (18) |
57 (24) |
2.2 |
0.75 |
1.4 |
–5.3 to 8.2 |
0.65 |
|
|
p-value |
0.89 |
0.98 |
0.87 |
|||||
|
RMSSD |
||||||||
|
FM |
36 (17) |
40 (22) |
3.7 |
0.51 |
–1.6 |
–6.9 to 3.6 |
0.48 |
|
|
HCs |
45 (23) |
44 (27) |
–0.6 |
0.92 |
–0.1 |
–4.9 to 4.6 |
0.95 |
|
|
p-value |
0.36 |
0.82 |
0.70 |
|||||
|
LF/HF ratio |
||||||||
|
FM |
1.2 (0.8) |
1.4 (0.8) |
0.18 |
0.63 |
0.19 |
–0.02 to 0.40 |
0.07 |
|
|
HCs |
1.7 (2.2) |
1.5 (1.1) |
–0.26 |
0.62 |
0.08 |
–0.18 to 0.34 |
0.50 |
|
|
p-value |
0.51 |
0.80 |
0.68 |
|||||
|
*Adjusted for baseline level and attendance rate. BP: blood pressure; CI: confidence interval; HF: high frequency; HRR: heart rate recovery; LF: low frequency; RMSSD: root mean square successive difference; SDNN: standard deviation of normal-to-normal heart beat intervals. |
||||||||
Pressure pain threshold and subjective symptom scores
Table V shows PPT in the upper and lower body in patients and HCs at the pre- and post-test, crude difference between the pre- and post-test, and adjusted mean change per exercise session. The patients had lower PPT in the upper and lower body compared with HCs at both the pre- and post-test. Both the crude and adjusted mean change in PPT for the upper body remained unchanged in both patients and HCs. For the lower body, the crude difference indicated no change, while the adjusted analysis indicated that PPT tended to increase in patients. Tests of interaction (attendance rate × group) indicated a tendency of larger change per exercise session in lower body PPT in patients than HCs (p = 0.09). This tendency was not present for the upper body (p = 0.23)
|
Table V. Pressure pain threshold (PPT) in the upper and lower body at pre- and post-test in patients with fibromyalgia (FM) and healthy controls (HCs) |
||||||||
|
Pre-test Mean (SD) |
Post-test Mean (SD) |
Crude difference (pre-post) |
p-value (crude difference) |
Adjusted mean change per exercise session* |
95% CI |
p-value (adjusted mean change) |
||
|
PPT upper body |
||||||||
|
FM |
186 (50) |
194 (66) |
8.0 |
0.72 |
3.2 |
–16 to 22 |
0.70 |
|
|
HCs |
313 (131) |
303 (85) |
–10.0 |
0.60 |
–7.8 |
–18 to 2.3 |
0.13 |
|
|
p-value |
0.008 |
0.002 |
0.54 |
|||||
|
PPT lower body |
||||||||
|
FM |
322 (188) |
328 (148) |
6.3 |
0.88 |
22.0 |
–5.3 to 49 |
0.09 |
|
|
HCs |
551 (213) |
567 (188) |
16.0 |
0.62 |
–14.0 |
–41 to 12 |
0.27 |
|
|
p-value |
0.01 |
0.002 |
0.85 |
|||||
|
*Adjusted for attendance and baseline level. PPT: pressure pain threshold. |
||||||||
Fig. 2 shows pain in: (A) the neck/shoulders; and (B) the low back in patients scored on the VAS at the pre- and post-test and before and after the exercise sessions. The HCs scored zero or very low throughout the intervention period, and only data from patients are included in Fig. 2. Paired comparisons within the patient group showed that pain in neck/shoulders decreased significantly from pre- to post-test (–14 ± 2.3 mm, p = 0.04), while the change in low back pain did not reach statistical significance (–10 ± 2.3 mm, p = 0.11). There was no significant correlation between improvement in VO2 from pre- to post-test and reduction in neck/shoulder pain (r = –0.37, p = 0.17) or low back pain (r = –0.33, p = 0.23). FIQ score (median, IQR) remained unchanged from pre- to post-test (median [IQR] 51.9 [21.6] vs 51.9 [32.2], p = 0.48) within the patient group.
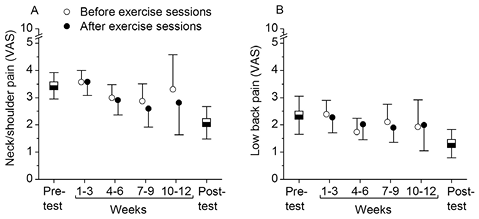
Fig. 2. Pain in neck/shoulders (A) and low back (B) scored on visual analogue scale (VAS) at pre- and post-test and during the intervention period in patients with fibromyalgia (FM) (values are mean with standard deviation). Values for the intervention period indicate averaged VAS scores over 3-week periods. Open and filled circles indicate pain level scored immediately before and after the exercise sessions, respectively.
DISCUSSION
The current study indicates that female patients with FM respond with similar aerobic and cardiovascular adaptations to moderate intensity endurance exercise as those of HCs. Exercise intensity and attendance rate did not differ between the patients and HCs; however, there was an extensive variation in attendance rate within both groups. The patients had lower baseline cardiovascular fitness than the HCs, but reported a similar level of physical activity on the IPAQ as HCs. Regression analysis with adjustments for attendance and baseline level showed that VO2 and workload at AT increased from pre- to post-test in patients and tended to increase in HCs; however, these improvements were of similar magnitude in both groups. Indices of cardiovascular autonomic function remained unchanged in both patients and HCs from pre- to post-test. PPT in lower and upper body remained essentially unchanged in both patients and HCs, while VAS score of neck/shoulder pain decreased significantly from pre- to post-test within the patient group.
Low-impact activity with low to moderate exercise intensity is recommended for patients with FM (17). The exercise programme was designed to accommodate these recommendations, while at the same time fulfil the recommended exercise dosage for maintaining or improving cardiovascular fitness (32), i.e. an attendance rate of ~70% or more was required to fulfil the recommended exercise dosage for maintaining or improving cardiovascular fitness in the current study. However, the attendance rate varied considerable both within the patients (20–100%) and HCs (16–100%). Attendance was significantly associated with improvements in cardiovascular fitness in patients and also tended to be associated with improvements in HCs, indicating a dose-dependent association between attendance and improvement in cardiovascular fitness. Regression analysis with adjustements for attendance and baseline level was therefore used to compare the response to the exercise programme between the patients and HCs. This analysis indicated a similar dose-dependent improvement in cardiovascular fitness in patients and HCs and no interaction between group and attendance. A similar observation has also been made for strength exercise, i.e. 21 weeks with progressive strength exercise was associated with similar strength improvements in HCs and premenopausal women with FM (33). Thus, patients with FM possess a similar ability as HCs for improving both strength and cardiovascular fitness and the common observation of low physical fitness in FM (10, 11, 13) is probably more closely related to deconditioning rather than to the illness per se (34). It has also been shown that the severity of FM symptoms is independent of muscle strength, which further supports the notion that low physical fitness in this patient group is independent of the illness (11).
A weakness in many interventional exercise studies that include patients with FM is the lack of precise intensity prescription and monitoring of exercise intensity (14, 17). Controlling exercise intensity, frequency and duration is of particular importance for patients with FM, since too much exercise may exacerbate symptoms, while too little exercise will not benefit the patient (17). In the current study, exercise intensity was monitored both by subjective assessment (i.e. RPE) and recordings of HR during the exercise sessions. Importantly, neither RPE nor HR differed between the patients and HCs, indicating that the perceived effort as well as the actual physical exertion were similar in both groups. Moreover, the subjects received continuous supervision and feedback on exercise intensity, ensuring that all subjects were within their individual pre-set HR range for moderate exercise intensity during the spinning workout sessions. The mean exercise intensity in the current study was 74% and 78% of maximum age-predicted HR in patients and HCs, respectively, placing our subjects above or in the higher end of the previous definitions of moderate exercise intensity (22). Nevertheless, the target exercise intensity used in the current study is well below the AT and was well tolerated by most patients (only 2 patients had to withdraw from the exercise programme because of exacerbation of symptoms). Others have reported that patients with FM tolerate exercise with moderate to high exercise intensity well (23). However, whether higher exercise intensities have a more positive impact on FM symptoms than low-intensity exercise is uncertain (17, 35).
Several studies have shown that regular physical exercise has a favorable effect on autonomic function, as indicated by increased parasympathetic modulation of resting HRV (36, 37) and faster HRR after strenuous physical exercise (38). Although we observed a significant improvement in cardiovascular fitness there was no change in HRR, blood pressure or HRV between the pre- and post-test in either the patients or HCs. A similar observation was made in an interventional study that investigated the effect of 12 weeks of strength exercises on HRV, i.e. patients with FM and HCs both improved significantly in strength, but there was no change in cardiac autonomic regulation between before and after the intervention (20). A recent randomized controlled trial investigated the effect of 16 weeks of either strength or flexibility exercise on symptoms and quality of life in patients with FM (18). The study showed significant improvements in strength, cardiovascular fitness and FM symptoms in the strength exercise group; however, despite the overall improvement in physical fitness there was no change in HRV before to after the intervention and the authors concluded that clinical improvements in patients with FM can be achieved without changes in autonomic regulation. Thus, the association between autonomic (dys)regulation, cardiovascular fitness and FM remain controversial and more research is needed to elucidate whether this association is of importance for understanding the aetiology of FM.
There is strong evidence that low to moderate aerobic exercise improves physical capacity and symptom severity in FM (8, 39). Despite improvement in cardiovascular fitness we only observed a significant but moderate reduction in neck/shoulder pain. Low back pain, FIQ score and PPT in the upper and lower body remained unchanged. The modest effect on FM symptoms may relate to the relatively short intervention period and the large variation in attendance within the patient group. The reduction in neck/shoulder pain was not correlated with improvement in VO2 at AT. Valim and co-workers (40) reported a similar finding, showing that reduction in FM symptoms after 20 weeks with moderate intensity endurance exercise was independent of gain in cardiovascular fitness. Thus, endurance exercise may induce psychological and biological changes (beyond improved cardiovascular fitness) that are of importance for a reduction in the severity of FM symptoms.
Study limitations
There are some limitations to the current study, primarily related to the study sample and the limited generalizability of our findings. In our study, 9 of 25 patients (36%) and 6 of 25 HCs (24%) resigned from the exercise programme and did not participate at the post-test. The drop-out among the patients is in the higher end of the attrition rates (i.e. 16–44%) described in other exercise interventions with FM patients (14). However, it should be noted that only 2 patients resigned due to worsening of pain during the initial 2–3 weeks of the exercise programme, while the other drop-outs were mainly related to other somatic diseases (5 patients) or personal reasons not related to FM symptoms (2 patients). One patient was excluded from analysis due to technical problems with post-test recording of the spirometric data. Thus, the high drop-out was mainly related to the general ill-health commonly observed in this patient group (1, 2) rather than to worsening of FM symptoms related to participation in the exercise programme. Nevertheless, the relatively low FIQ score may indicate that our study sample may represent the more healthy part of the FM population, and therefore the generalizability of our results may be limited.
Conclusion
The current findings suggest that female patients with FM possess a similar ability for improvement in cardiovascular fitness to that of HCs. This finding lends further support to the notion that peripheral muscular abnormalities commonly observed in patients with FM may be more closely related to deconditioning than to the illness per se. Despite improvements in cardiovascular fitness in both patients and HCs we observed no change in cardiac autonomic regulation.
REFERENCES

