Willeke J. Kruithof, MD1, Marcel W. M. Post, PhD1, Christel M. van Leeuwen, PhD1, Vera P. M. Schepers, PhD1, Geertrudis A. M. van den Bos, PhD2 and Johanna M. A. Visser-Meily, PhD1
From the 1Brain Center Rudolf Magnus and Center of Excellence for Rehabilitation Medicine, University Medical Center Utrecht and De Hoogstraat Rehabilitation, Utrecht and 2Department of Social Medicine, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands
OBJECTIVE: To describe the course of social support (everyday support, support in problem situations and esteem support) from initial inpatient rehabilitation until 3 years post-stroke and to examine the cross-sectional and longitudinal relationships of social support with depressive symptoms.
DESIGN: Prospective cohort study.
SUBJECTS: A total of 249 stroke patients.
METHODS: Depressive symptoms were measured with the Center of Epidemiologic Studies Depression Scale. Perceived social support was assessed with the Social Support List-Interaction. Pearson correlations and multilevel analysis were performed.
RESULTS: More than one-third of participants had depressive symptoms. Social support and its 3 subtypes declined significantly over time. Divergent relationships were found between subtypes of social support and depressive symptoms. Everyday support and esteem support had negative associations with depressive symptoms, whereas support in problem situations had a positive association. Social support in problem situations was a predictor of depressive symptoms over time. No effect-modification by participants with physical or cognitive limitations was found.
CONCLUSION: Stroke survivors experience a decline in social support over time. Various subtypes of support show distinct relationships with depressive symptoms. Healthcare professionals should focus on the various subtypes of support when supporting patients to improve and maintain an adequate social support network.
Key words: stroke; depression; social support.
J Rehabil Med 2015; 47: 599–604
Correspondence address: J. M. A. Visser-Meily, University Medical Center Utrecht, Huispost W 01.121, PO Box 85500, NL-3508 GA Utrecht, The Netherlands. E-mail: j.m.a.visser-meily@umcutrecht.nl
Accepted Mar 3, 2015; Epub ahead of print Jun 12, 2015
INTRODUCTION
Post-stroke depression is a major problem (1–3); approximately one-third of all stroke survivors worldwide suffer from depression (1). The underlying aetiology of post-stroke depression is poorly understood; both biological and psychological mechanisms are thought to play a role (4–6). The biological mechanism may include several neurological factors, such as lesion location (left hemisphere, basal ganglia), neurotransmitters and inflammatory cytokines (4, 6). Stroke is, however, also an overwhelming psychological event and stroke survivors face the challenge of adapting to a new situation. This may trigger depressive feelings.
Lack of social support is consistently associated with post-stroke depression (4, 5). Social support seems to have a “protective effect” against developing post-stroke depressive symptoms, buffering the negative consequences of stroke and reducing depressive symptoms (5, 7). It is a broad concept and can be defined as any support given outside formal settings, i.e. not by health professionals or social services (8). To make this concept more concrete, social support can be divided into 3 different subtypes: “everyday support”, “support in problem situations” and “esteem support” (9).
It is important to consider both the type and the timing of social support (10, 11). However, most stroke studies measure social support with a single total score, as if it were a one-dimensional factor. Consequently, there is insufficient knowledge about the impact of different subtypes of social support. Furthermore, most studies are cross-sectional, so that the course of social support and the longitudinal relationships of social support with stroke outcome are rarely investigated. It is possible that this lack of detailed knowledge about type and timing of social support resulted in the generally disappointing effectiveness of social support interventions for post-stroke depression published in a review in 2010 (12).
The aims of this study are therefore: (i) to describe the course of stroke survivors’ social support and 3 subtypes of social support (i.e. everyday social support, social support in problem situations and esteem support) from the start of initial inpatient rehabilitation until 3 years post-stroke; (ii) to examine the cross-sectional relationships between social support, including the 3 subtypes, and depressive symptoms at various times post-stroke; and (iii) to examine the longitudinal relationships between social support, including the 3 subtypes, and depressive symptoms over time, correcting for potential confounding and effect modification.
Our first hypothesis is that social support and the 3 subtypes will decline over time, because the disabilities resulting from stroke (e.g. sensomotoric, communicative and cognitive) make it a major challenge for stroke survivors to maintain an adequate social network. Furthermore, we expect that less social support is associated with more depressive symptoms at all measurement occasions (4, 5). However, because of the different aspects of the subtypes the strength of the associations might differ; this has not yet been investigated. With regard to the third aim of our study, we hypothesize that all subtypes of social support are negatively associated with depressive symptoms over time. Finally, the theory that social support buffers the negative consequences of stroke (5, 7) predicts that the association between social support and post-stroke depression will be stronger in stroke survivors with relatively severe disabilities than in stroke survivors with relatively minor disabilities. Therefore, we hypothesize that the association between social support and depression will be stronger in stroke survivors scoring below established cut-off points for physical and cognitive disability than in stroke survivors scoring above these cut-off points.
METHODS
Participants
Study subjects were selected from stroke patients who participated in the “Functional Prognosis after Stroke” (FuPro-Stroke) study (13). They were recruited through 9 Dutch rehabilitation centres between April 2000 and July 2002. Inclusion criteria were: first-ever stroke; 1-sided supratentorial lesion; and age above 18 years. Exclusion criteria were: disabling comorbidity (defined as a pre-stroke Barthel Index <18); and inability to speak Dutch.
For the present analysis patients with aphasia were excluded, since they were unable to complete the Center of Epidemiologic Studies Depression Scale. The presence of aphasia was operationalized as a score in the clinical range of either the Token Test (short version, score ≥ 9) or the Utrecht Communication Observation (Utrechts Communicatie Onderzoek, score < 4) (13). Each assessment the presence of aphasia was measured again.
The study was approved by the medical ethics committees of the University Medical Center Utrecht and the participating rehabilitation centres. Informed consent was obtained from all participants.
Procedure
At the start of inpatient rehabilitation, stroke patients were invited by their rehabilitation specialists to participate in the study. The first assessment was conducted as soon as possible after informed consent was given. Other assessments followed at 1 and 3 years after stroke. Patients were assessed at home or at the institution where they lived by trained research assistants.
Measures
Perceived social support was measured with the Social Support List-Interaction (SSL-12-I) (Appendix I). This questionnaire measures the patients’ subjective experience of social support. The SSL-12 consists of 12 items in 3 scales: “everyday social support” (social companionship and daily emotional support), “support in problem situations” (instrumental support, informative support, and emotional support in times of trouble), and “esteem support” (support resulting in self-esteem and approval) (9). The score ranges from 12 to 48, and higher scores indicate more social support. It has good psychometric properties (9).
Depressive symptoms were measured using the Center of Epidemiologic Studies Depression Scale (CESD). The total score of this 20-item scale ranges between 0 and 60, and a score ≥ 16 indicates a clinically relevant presence of depressive symptoms. It has a good reliability and validity (14, 15).
Cognition was assessed with the Mini Mental State Examination (MMSE), which is a screening test with good validity and reliability (16). Participants were scored as having cognitive disability if the MMSE score was ≤ 23 points or if they were not able to complete this test due to aphasia.
Independence in activities of daily living (ADL) was assessed using the Barthel Index (17), which is a valid and reliable instrument (18, 19). Participants were scored as dependent if the Barthel Index score was ≤ 18.
Demographic characteristics, such as age, gender and type of stroke, were obtained from medical charts. Other data on marital status, pre-stroke employment and educational level were documented at the start of the inpatient rehabilitation.
Statistical analysis
All participants who completed at least one of the 3 measurement occasions were included in the analyses. Descriptive statistics were used to describe the demographic characteristics of the stroke survivors. Pearson correlations were used to investigate the cross-sectional associations between social support, its 3 subtypes and depressive symptoms.
To examine the course of social support (and its subtypes) and depressive symptoms up to 3 years post-stroke, random coefficient analysis (multi-level analysis) was used. Two advantages of this method in longitudinal studies are: (i) the number of observations per stroke survivor and the temporal spacing of these observations can be varied; (ii) this method considers dependency of repeated measures within the same person (20).
First, the course of social support was studied with time as the only determinant. Time was entered in the model as a set of 2 dummy variables with T1 (at baseline) as reference. Total social support and the 3 subtypes were separately used as the dependent variable, resulting in 4 different models.
To analyse the relationships between social support and depressive symptoms over time, again 4 different basic multi-level linear regression models were used with depressive symptoms as the dependent variable (T1, T2 and T3), 1 model for each subtype of social support and total support as the independent variable (also T1, T2 and T3).
Effect modification, related to level of disability, of the relation between social support and depressive symptoms was also investigated. Effect modification occurs if the association between social support and depressive symptoms is different in participants with disability than in participants without disability. Since the MMSE and the Barthel Index scores were strongly inter-correlated and the MMSE score was highly skewed, both variables were combined in 1 new variable. This new variable was dichotomized to indicate the presence of problems in ADL or cognition (MMSE ≤ 23 or Barthel Index ≤ 18) or the absence of these problems, and to facilitate the clinical interpretation of the findings. Both, the new variable and the interaction term between the social support variable and this new variable were added to the basic models.
To test for confounding the demographic (age, gender, having a partner, having children, educational level, pre-stroke employment) and clinical characteristics (type of stroke, hemisphere affected, post-stroke time, dependence in ADL and cognitive impairment) were added one by one to each model. A characteristic was considered a confounder if the B values of the above independent variables or interactions changed more than 10% after adding them to the model.
SPSS statistical program for Windows (version 16.0) and the MLwiN program of the Centre for Multi-level Modelling of the Institute of Education in London (version 1.1) were used for the analyses.
A p-value < 0.05 was considered statistically significant.
RESULTS
Participants
A total of 308 stroke survivors were recruited in the FuPro-stroke study. At baseline (T1) 206 participants, at 1 year post-stroke (T2) 210, and at 3 years post-stroke (T3) 174 participants completed the measurement on social support at T1, T2 and T3, respectively. A total of 249 participants (response percentage 81%) completed at least one measurement on social support in 3 years and were included for the current analyses.
Fifty-nine of the 308 stroke survivors could not complete any measurement on social support. A non-response analysis revealed that these stroke survivors were more often male, more often had a lesion in the left hemisphere and a lower mean educational level than the 249 participants.
Table I displays the demographic and stroke characteristics of the participants at admission for inpatient rehabilitation. The majority were men (57%) and their mean age was 56.7 years. The majority had had an infarction. More than one-third (36.9%) showed clinically relevant depressive symptoms. At baseline 76.7% were dependent in ADL and 17.1% reported cognitive impairments.
|
Table I. Baseline characteristics (n = 249) |
|
|
Included stroke patientsa |
|
|
Demographic characteristics |
|
|
Age, mean (SD), median (IQR) |
56.7 (10.8), 56.0 (49.0–65.0) |
|
Female gender, % |
43.0 |
|
Living with a partner, % |
72.3 |
|
Having children, % |
81.5 |
|
Educational level (higher education)b, % |
19.3 |
|
Pre-stroke employment status (employed), % |
42.2 |
|
Place of residence 3 years post-stroke, % at home |
91.4 |
|
Stroke characteristics |
|
|
Type of stroke (infarction), % |
71.9 |
|
Hemisphere (right), % |
54.6 |
|
Post-stroke time in days, mean (SD) |
50.5 (24.0) |
|
Barthel Index, mean (SD), median (IQR), % dependentc |
13.9 (4.6), 14.0 (10–18), 76.7% |
|
Mini Mental State Examination (MMSE), mean (SD), median (IQR), % presentd |
26.0 (2.8), 27.0 (24.5–28.0), 17.1% |
|
Dependence in ADL and/or cognitive impairment, % |
78.0 |
|
Depressive symptoms, mean (SD), median (IQR), % presente |
13.7 (9.3), 12.0 (6.0–18.0), 36.9% |
|
aStroke patients are included when at least 1 out of 3 social support lists is completed. bSenior secondary education, university preparatory education, higher professional education, and university. cDependent in ADL if Barthel Index is ≤ 18. dCognitive impairments are present if MMSE ≤ 23. eDepressive symptoms are present if CESD ≥ 16. n: number of patients; SD: standard deviation; IQR: interquartile range; ADL: activities of daily living; CESD: Center of Epidemiologic Studies Depression Scale (CESD). |
|
Course of social support
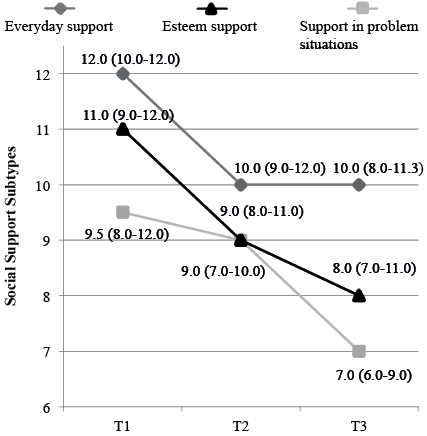
Table II shows the descriptives of social support and depressive symptoms at each time-point and Fig. 1 displays the course of the 3 subtypes of social support over time as estimated using random coefficient analysis. It shows a similar decrease in each subtype of social support over time. This decline in social support was significant in both time periods (T2–T1 and T3–T1, respectively) (Table III).
|
Table II. Descriptives of stroke patients’ total social support, everyday social support, support in problem situations, esteem support, depressive symptoms at T1–T3 (n = 249) |
||||||||
|
T1 |
T2 |
T3 |
||||||
|
Mean (SD) |
Median (IQR) |
Mean (SD) |
Median (IQR) |
Mean (SD) |
Median (IQR) |
|||
|
Total social support |
31.6 (6.1) |
31.0 (27.8–36.0) |
28.4 (6.0) |
28.0 (24.0–32.0) |
26.4 (6.1) |
26.0 (22.0 –31.0) |
||
|
Everyday social support |
11.1 (2.3) |
12.0 (10.0–12.0) |
10.4 (2.2) |
10.0 (9.0–12.0) |
9.9 (2.2) |
10.0 (8.0–11.3) |
||
|
Support in problem situations |
9.7 (2.5) |
9.5 (8.0–12.0) |
8.8 (2.6) |
9.0 (7.0–10.0) |
7.7 (2.5) |
7.0 (6.0–9.0) |
||
|
Esteem support |
10.7 (2.6) |
11.0 (9.0–12.0) |
9.3 (2.5) |
9.0 (8.0–11.0) |
8.8 (2.7) |
8.0 (7.0–11.0) |
||
|
Depressive symptoms |
13.7 (9.3) |
12.0 (6.0–18.0) |
11.7 (8.9) |
10.0 (4.0–17.0) |
10.0 (8.1) |
8.0 (4.0–14.0) |
||
|
T1: at admission; T2: 1 year post-stroke; T3: 3 years post-stroke; SD: standard deviation; IQR: interquartile range. |
||||||||
Fig. 1. Course of subtypes of social support over time. Figures represents median (IQR). T1: at admission; T2: 1 year post-stroke; T3: 3 years post-stroke.
|
Table III. Multilevel linear regression model for the course of social support between baseline and 3 years after stroke (n=249) |
|||||||||||||||
|
Variables |
Model for total social support |
Model for everyday support |
Model for support in problem situations |
Model for esteem support |
|||||||||||
|
Beta |
SE |
p |
|
Beta |
SE |
p |
Beta |
SE |
p |
Beta |
SE |
p |
|||
|
Constant |
31.354 |
0.407 |
11.051 |
0.150 |
9.699 |
0.171 |
10.623 |
0.170 |
|||||||
|
Time T2–T1 |
–3.054 |
0.384 |
< 0.001 |
–0.807 |
0.144 |
< 0.001 |
–0.913 |
0.180 |
< 0.001 |
–1.343 |
0.161 |
< 0.001 |
|||
|
Time T3–T1 |
–5.269 |
0.411 |
< 0.001 |
–1.304 |
0.154 |
< 0.001 |
–2.030 |
0.192 |
< 0.001 |
–1.931 |
0.202 |
< 0.001 |
|||
|
All 4 models had random intercepts. All time-dependent covariates had a fixed slope, except for time (T3–T1) in the model for esteem support, which had a random slope. T1: at baseline. T2: 1 year post-stroke. T3: 3 years post-stroke. Beta: non-standardized regression coefficient in multilevel analyses; SE: standard error; p: p-value. |
|||||||||||||||
Social support and depressive symptoms
Some bivariate correlations between social support, its 3 subtypes and depressive symptoms were significant, although weak and without an apparent relationship with measurement occasion (Table IV). The 3 subscales had opposite coefficients in their relationship with depressive symptoms. Everyday support and esteem support showed negative associations with depressive symptoms, whereas support in problem situations showed a positive association.
|
Table IV. Pearson correlations between social support and depressive symptoms at the 3 different measurements (n = 249) |
||||
|
Depressive symptoms |
Total social support |
Everyday social support |
Support in problem situations |
Esteem support |
|
T1 |
0.022 (0.756) |
–0.077 (0.274) |
0.146 (0.037)* |
–0.024 (0.730) |
|
T2 |
–0.109 (0.116) |
–0.181 (0.009)* |
0.019 (0.780) |
–0.124 (0.073) |
|
T3 |
–0.079 (0.301) |
–0.140 (0.067) |
0.103 (0.178) |
–0.156 (0.040)* |
|
Figures are Pearson correlations with p-values. *p-value < 0.05. T1: at admission; T2: 1 year post-stroke; T3: 3 years post-stroke. |
||||
In the random coefficient analyses, only social support in problem situations showed a significant positive direct relationship with depressive symptoms over time, indicating that social support in problem situations is a predictor of depressive symptoms (Table V). No significant confounders were found for this model.
|
Table V. Multilevel linear regression models for the direct relationship between different types of social support and depressive symptoms (n = 249) |
|||||||||||||||
|
Depressive symptoms |
Model for total social support |
Model for everyday support |
Model for support in problem situations |
Model for esteem support |
|||||||||||
|
Beta |
SE |
p |
|
Beta |
SE |
p |
Beta |
SE |
p |
Beta |
SE |
p |
|||
|
Constant |
10.385 |
2.148 |
14.112 |
1.752 |
7.792 |
1.251 |
11.934 |
1.805 |
|||||||
|
Social support variable |
0.094 |
0.059 |
0.112 |
–0.203 |
0.162 |
0.211 |
0.479 |
0.131 |
< 0.001 |
0.127 |
0.138 |
0.358 |
|||
|
Confounders |
|||||||||||||||
|
Cognitive impairment |
–1.738 |
1.401 |
0.215 |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
–1.701 |
1.413 |
0.230 |
|||
|
Educational level (higher education) |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
–0.239 |
1.316 |
0.857 |
|||
|
Hemisphere (right) |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
n.e. |
1.620 |
1.019 |
0.112 |
|||
|
All 4 models had random intercepts. All time-dependent covariates had a fixed slope for the direct relationship. Beta: a non-standardized regression coefficient in multilevel analyses; SE: standard error; p: p-value; n.e.: not entered. |
|||||||||||||||
Effect modification
None of the interaction terms tested was significant. This means that the associations between social support and depressive symptoms in participants with relatively severe disabilities were not significantly different from these associations in stroke survivors with relatively minor disabilities.
DISCUSSION
The present study describes the course of social support, as a total scale and as divided in 3 subtypes, and depressive symptoms in stroke survivors up to 3 years post-stroke. As hypothesized, social support and depressive symptoms declined over time. Our hypotheses about the cross-sectional and longitudinal relationship between social support and depressive symptoms were partly confirmed. Social support was associated with post-stroke depressive symptoms, although we had expected more consistent and stronger relationships. The advantage of examining subtypes of social support instead of a total scale was established: Depressive symptoms over time are predicted by social support in problem situations and not by everyday support or esteem support. No significant interactions were found; consequently our hypothesis on effect modification could not be established. Above all, this study reveals that social support cannot be seen as a one-dimensional factor and should be assessed within subtypes.
Course of social support
Levels of social support decreased over time in this study for all subtypes. A decrease in contacts with other persons over time has also been suggested by earlier cross-sectional studies (21–23). In the chronic phase, contacts with children seem more or less the same after stroke (21–23), but a majority of stroke survivors had less contact with friends (22), suggesting that it is difficult for persons with stroke to maintain friendships. Our study adds a longitudinal description of different subtypes of social support in a general stroke population over time to the stroke literature.
The levels of total social support and the 3 subtypes reported at baseline and at 1 year post-stroke were higher than those reported in the general elderly Dutch population (26.4, 9.7, 8.0 and 8.7, respectively) (9). At 3 years post-stroke the support levels of the stroke survivors were approximately the same as in the elderly population. However, “average” does not necessarily equal “sufficient”, since stroke survivors might need more social support than healthy elderly people, and a lack of social support is common in the elderly population (24).
Social support and depression
Our study shows that social support, including its 3 subtypes, is related to post-stroke depressive symptoms. There were significant correlations, although not at each measurement, in line with what was reported by other studies (5, 7), and adding an analysis of support subtypes and a follow-up period of 3 years to the literature.
Furthermore, our study shows, on the one hand, that more support in problem situations is associated with more depressive symptoms and, on the other hand, that more everyday support and esteem support are associated with less depressive symptoms. This partly corresponds to the literature, in which a systematic review presented that low social support was consistently associated with depression (5), and instrumental and emotional support were associated with depressive symptoms at 1 month post-stroke (instrumental and emotional support) and 3 months post-stroke (emotional support) (25).
Social support can increase the autonomy of stroke survivors (positive effect), but can also confirm the dependency of the stroke survivor to others (negative effect) (10). Perhaps, everyday support and esteem support have both effects in it (and more positive than negative effects), resulting in a non-significant positive association. On the other hand, support in problem situations confirms the dependency of the stroke survivor to others more, resulting in a significant negative association with post-stroke depressive symptoms.
These opposed directions might also explain the lack of significant association between total social support and depressive symptoms. Therefore, social support should not be measured as a total scale, but in subscales.
Social support, including its 3 subtypes, was associated with post-stroke depressive symptoms, although we had expected more consistent and stronger relationships. This finding may be explained by the disability profile of the participants. Our participants had relative high Barthel (mean 13.9 at baseline) and MMSE scores (mean 26.0 at baseline) suggesting a relatively moderately disabled group. Lewin and colleagues also focused in their study on former inpatient rehabilitation patients and showed that high levels of social support were a protective factor for depressive symptoms (7). In comparison with this study, our study population was younger, was less dependent in ADL and had a slightly lower score on the MMSE (7).
Effect modification
No effect modification of disability (in terms of having physical or cognitive disability) in the relationship between social support, its 3 subtypes and depressive symptoms, that is no significant interaction term, was found. No other studies focusing on effect modification in the relationship between social support and depressive symptoms after stroke were found. Our results imply that no stronger association between social support and depressive symptoms in stroke survivors who experience problems in ADL or cognition was found. This finding suggests that social support is always important, whether or not there are problems in ADL or cognition. An alternative explanation is that our study group consisted of persons with a relatively high Barthel score and high score on the MMSE, making it difficult to analyse this factor.
Strengths of the study
It is important to investigate social support in the subacute and chronic phases of stroke in a relatively young and moderately disabled population, because this support could be needed for many years or even lifelong. Therefore, one of the strengths of this study is its longitudinal design with a follow-up of 3 years. Furthermore, we specified social support by type. Patients may need different types of support at different times post-stroke. If the course of different types of support is clarified further, interventions could be better targeted.
Study limitations
Firstly, the participants in this study had a relatively high Barthel score and high MMSE score, suggesting a relatively moderately disabled study group. This may jeopardize generalization of the results to all stroke patients and their partners.
Secondly, we assumed a causal relationship between social support and depressive symptoms, but we cannot prove causality in this observational research. In the literature, the association between these variables has already been proven (4, 5) and a “protective effect” for developing post-stroke depressive symptoms has been suggested (5, 7).
Thirdly, a non-response analysis revealed that the non-responders differ in gender, hemisphere affected and educational level. However, in our statistical analyses we have also put these variables in each model to correct for the possible effect on the relationship between social support and depressive symptoms.
Fourthly, we performed linear regression analysis on the Social Support List-Interaction, which is a rating scale that has not yet undergone Rasch validation and transformation.
Finally, the study results should be interpreted with care beyond the Dutch culture and (in)formal care system.
Conclusion
Stroke survivors experienced a decline in social support, as a total scale and as divided into 3 subtypes, over time. Although we had expected stronger relationships, social support was related to post-stroke depressive symptoms. Social support in problem situations was a predictor of depressive symptoms over time, but not specifically in stroke survivors with disability. Above all, this study reveals that social support should not be seen as a one-dimensional factor due to the opposite coefficients of the support subscales in their relationship with depressive symptoms.
Practice implications
Attention should be paid to improving and maintaining adequate social support for stroke survivors from the beginning of the inpatient rehabilitation process up to the chronic phase. Healthcare professionals should focus on the various subtypes of social support, especially support in problem situations when dealing with depressive symptoms, both in practical healthcare and in designing interventions to enhance social support.
Further research
Further research could be focused on developing interventions to strengthen social support networks and decreasing depressive symptoms post-stroke. Therefore, it is important to reveal which stroke survivors could maintain their social network and which are at risk for social isolation and unmet needs. In elderly people, it has already been suggested that interventions to reduce social isolation should have a theoretical basis and offer social activity and/or support within a group format (24). Furthermore, interventions in which people are active participants also appeared to be effective (24). It would be worth investigating these interventions in the stroke population.
As mentioned before, social support is a broad concept and various aspects should be taken into account when targeting interventions. The type of support needed may vary over time and the people who give support may also vary over time or by type of support (10, 11). Therefore, next to dividing social support by subtype, as in this study, dividing it by source (i.e. partner, relatives or friends) and timing may also be of benefit in targeting interventions for strengthening social networks and decreasing post-stroke depression.
APPENDIX
Appendix I. SSL-12-I; Questions arranged by subtype |
Dimensions of social support |
Everyday social support |
Does it ever happen to you that people… - invite you to a party or to dinner? - drop in for a (pleasant) visit? - show you that they are fond of you? - just call you up or just chat to you? |
Social support in problem situations |
Does it ever happen to you that people… - comfort you? - provide you with help in special circumstances such as illness or moving home? - reassure you? - give you good advice? |
Esteem support |
Does it ever happen to you that people… - pay you a compliment? - confide in you? - ask you for help or advice? - emphasize your strong points? |
REFERENCES

