Abderrazak Hajjioui, MD1, Maryam Fourtassi, MD2 and Chakib Nejjari, MD, PhD3
From the 1Department of Physical Medicine and Rehabilitation, Faculty of Medicine and Pharmacy of Fez, Sidi Mohammed Ben Abdallah University, Fez, 2Department of Physical Medicine and Rehabilitation, Faculty of Medicine and Pharmacy of Oujda, Mohammed Premier University Oujda, Oujda and 3Department of Epidemiology and Clinical Research, Faculty of Medicine and Pharmacy of Fez, Sidi Mohammed Ben Abdallah University, Fez, Morocco
OBJECTIVES: To investigate the prevalence of disabilities amongst adult hospitalized patients and to estimate their specific needs for rehabilitation support.
METHODS: A cross-sectional study was conducted in a Moroccan university hospital. A total of 411 patients were included, and assessed for impairments, activity limitations and participation restrictions through medical examination and structured questionnaires. Patients’ clinical and assessment data were used to estimate the specific needs for rehabilitation professionals’ intervention, and the optimal mode of rehabilitation support.
RESULTS: Patients’ mean age was 47.75 years (standard deviation (SD) 17.34). Prevalences of types of impairments were led by pain (41.6%), followed by sensory-motor deficits (21.9%) and limitations in joint range of motion (21.4%). Activity limitations were dominated by gait and balance disorders (25.3%). Participation restrictions in social and family life were reported by 118 patients; and in professional life by 44 patients. The most needed rehabilitation interventions were: physiotherapy (36.2%), occupational therapy (20.4%), and prosthetics (15.8%), and 24.5% patients were eligible for inpatient rehabilitation support.
CONCLUSION: Disability is very common among hospitalized Moroccan patients, and there is a great need for inpatient rehabilitation support in Moroccan hospitals.
Key words: Morocco; disability evaluation; disabled persons; disability and health; health services needs and demand; public health; inpatients rehabilitation; prevalence.
J Rehabil Med 2015; 47: 593–598
Correspondence address: Abderrazak Hajjioui, BP 1893, Km 2200, Route de Sidi Hrazem, 30000 Fez, Morocco. E-mail: hajjiouiabdo@yahoo.fr
Accepted Mar 27, 2015; Epub ahead of print Jun 12, 2015
INTRODUCTION
The World Health Organization (WHO) estimates that more than one billion people around the world are living with some kind of disability (1). There is an extensive medical literature highlighting the cost-effectiveness of structured medical rehabilitation in improving the general health condition, the optimal autonomy level, and the quality of life of people with disabilities, and in returning them to productive lives (2, 3). Currently, 80% of people with disabilities live in low-income countries and most of them have limited or no access to healthcare support and rehabilitation facilities (1). Furthermore, Physical and Rehabilitation Medicine (PRM) is almost non-existent in these countries’ medical care systems (3), which contributes to deny people with disabilities the right to access a qualified and specialized medical care.
In Morocco, the National Disability Survey, conducted in 2004 by the Secretary of State for “Social Protection, Family and Children” (SSSPFC) revealed that 1.5 million people live with disabilities, representing 5% of the Moroccan population, and 55.7% are in the age range 15–59 years (4). This prevalence is likely to be an underestimate. A more recent survey by the Moroccan Ministry of Health showed that 18.2% of the Moroccan population had at least 1 chronic disease. This rate rises to 57.5% among subjects aged 60 years and more (5), suggesting a higher prevalence of disabilities, as chronic diseases often result in some kind of disability.
Access to medical care appears to be the first requirement for people with disabilities in Morocco. More than 1 person in 5 has never attended a healthcare institution (4). This is due to lack of financial resources (80%), geographical remoteness (25%), negative image of public health services (21%), and the limited resources of these institutions to meet the patients’ needs (18%) (4).
In contrast with other extensively developed medical disciplines in Morocco, PRM remains poorly represented. The activity indicator for public hospitals for the year 2011 revealed that only 5 hospital beds in the whole country had dedicated to PRM activity. In contrast, 28 beds were dedicated to plastic surgery (6), which could be considered as luxury medical care in a limited resources healthcare system. Regarding this situation, the Moroccan Economic Social and Ecological Council (ESEC) set out a number of recommendations in its 2012 report, such as creating and developing PRM departments in university and regional hospitals (7).
The present study is the first step in the project to create a PRM department in a large Moroccan university hospital. The aim of the study was to investigate the prevalence and characteristics of disabilities amongst hospitalized patients and to estimate the specific needs for rehabilitation resources and professionals, in order to offer optimal rehabilitation care to this specific population.
MATERIAL AND METHODS
Study design
This cross-sectional study was performed in Hassan II teaching hospital, Fez, Morocco, with a capacity of 683 beds. The study was conducted on a single day; 29 March 2012.
Characteristics of the study population
All of the hospital inpatients were considered for inclusion in the study. Exclusion criteria were: age under 18 years, patient’s inability to be interviewed because of a severe illness, cognitive and speech disorders, temporary absence from the ward at the time of interview (operating room, radiological examination, etc.), or refusal to participate in the study (Fig. 1).
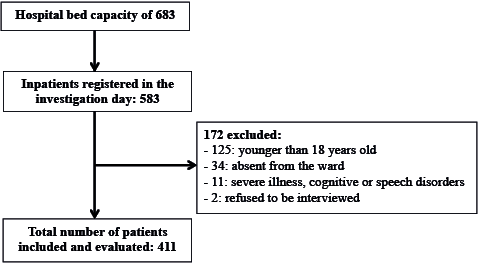
Fig. 1. Patients considered for participation in the study.
Data collection
The study included a total of 25 hospital wards with inpatient activity. Psychiatry and ophthalmology departments were not included in the study as they were located in independent buildings some distance from the main hospital. Data were collected by 25 medical collaborators (15 interns and 10 physical therapists), each in a single ward. Prior to the study all investigators received training about disability assessment.
Demographic characteristics were obtained directly from the patients during an interview, and clinical characteristics were obtained from the patients’ medical charts. For each patient, different aspects of disability were evaluated using a structured questionnaire. Specific impairments, generally targeted by rehabilitation care (joint range of motion (ROM) limitation, sensory motor deficits, symptomatic bladder dysfunction, pain, dysphagia and chest congestion, and pressure ulcers), were systematically checked in the patients’ medical charts, and verified by a short medical examination. Investigators assessed the presence of different activity limitations associated with the patients’ medical condition (gait and balance disorders, communication difficulties, feeding difficulties, grooming and dressing difficulties, and grasping difficulties). Participation restrictions were approached by both the use of the “Modified Rankin Scale” (8), assessing the patient’s autonomy level (from 0: asymptomatic, to 5: totally dependent), and by asking the patient to state (yes/no) whether his/her medical condition had a negative impact on his/her family and social life and/or professional life.
The principal investigator (PMR physician) used the above data to assess the theoretical need for rehabilitation support for each patient. The theoretical need for a specific rehabilitation professional intervention (physiotherapist, occupational therapist, speech and language therapist, or prosthetist) was determined according to the diagnosis and the observed impairments. The optimal rehabilitation support organization (inpatient rehabilitation, outpatient rehabilitation) was suggested according to the patient’s level of autonomy, the number of rehabilitation professionals needed, and the patient’s geographical remoteness from medical facilities.
Statistical analysis
All aspects of disability were considered in terms of presence or absence. Descriptive statistics, including size and frequencies for categorical variables, and means and standard deviations for continuous variables, were determined. Participation restrictions and Rankin score were assessed for potential correlations with patients’ demographic and clinical characteristics. The relationship between categorical variables was analysed using a χ2 test. The relationship between binary disability indicators and continuous predictors was assessed with logistic regression. Free Epi-info software (3.5.1) was used for all statistical analyses. A p-value of 0.05 or less was considered statistically significant.
Ethics
The study was carried out in agreement with Moroccan law and the principles of the Declaration of Helsinki on protecting human subjects, and was approved by the local ethics committee. All patients included in this study were informed of the study aims and characteristics and gave their informed consent to participate.
RESULTS
Demographic and clinical characteristics of the patients
A total of 411 patients were included in the study. Their demographic and clinical characteristics are shown in Table I. The mean age of the patients was 47.75 years (SD 17.34 years) and the majority were female (female/male (F/M) ratio: 1.3). The majority of patients were married (72.26%), living in urban areas (66.42%), with an average of 2 children per family (range 0–12). Of the participants, 58.39% were illiterate, 70.56% had a work activity either as an employee, house-worker or student, and 71.29% belonged to a poor family with a monthly household income of less than 200 US dollars (USD). Most of the patients were diagnosed with non-communicable diseases (89.5%), with cancer being the leading diagnosis (20.9%), followed by cardiovascular (19%) and neurological (11.4%) diseases. Finally, 36.25% of the study population came from other Moroccan administrative regions than the Fes-Boulman region where the Hassan II university hospital is located.
Assessments of disability prevalence
Impairments. Pain was the most common impairment, reported by 171 (41.6%) patients, with an mean intensity of 4.70 (SD 2.01) on the 10-cm visual analogue scale. Pain was followed by sensory-motor deficits, found in 90 (21.9%) patients, and joint ROM limitations, found in 88 (21.4%) patients. Dysphagia and/or chest congestion were identified in 69 (16.8%) patients. Symptomatic bladder dysfunction and pressure ulcers were the least common impairments, found in, respectively, 19 (4.6%) and 14 (3.4%) of the study population. As shown in Fig. 2, distribution of these impairments varied according to the patients’ medical condition category. Pain, sensory-motor deficits, joint ROM limitations, and pressure ulcers were more common in patients with injury, whereas chest congestion was more common in patients with communicable diseases.
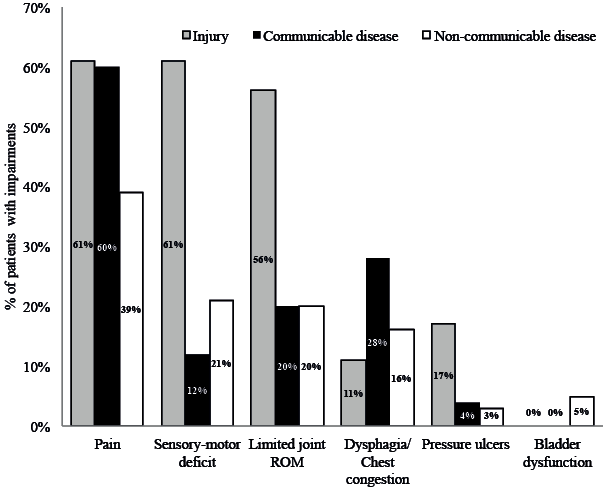
Fig. 2. Prevalence of impairments in different medical condition categories.
Activity limitations. Activity limitations were dominated by gait and balance disorders, present in 104 (25.3%) patients, followed by difficulties in activities of daily living, such as grooming and dressing, gripping and feeding, reported by 91 (22.1%), 49 (11.9%) and 33 (8%) patients, respectively. Communication difficulties were observed in 16 (3.9%) persons.
Participation restrictions. A total of 44 patients, out of 290 with a work activity, reported a negative impact of their medical condition on their work life, whereas 118 patients out of 411 reported a negative impact on their social life. Table II shows the correlations between the presence of a negative impact on patients’ lives, and their demographic characteristics. There was a significant relationship between the absence of health insurance and the presence of a negative impact on both professional and social lives. Work impact was correlated with the patients’ household income level (p < 0.01) and social impact was associated with the patients’ sex (p = 0.01), and was more common in patients leading an active work life (p < 0.01). Work impact was significantly more common in patients with injuries and non-communicable diseases than in those diagnosed with communicable diseases, whereas social impact did not show such relationships with any specific medical condition category.
The mean Rankin score in our study population was 1.80 (SD 1.3), with a score higher than 3 (moderately severe and severe disability) in 65 (15.9%) patients. Rankin score was significantly correlated with older age (p < 0.01) and injury (p = 0.01). However, there were no other significant relationships between Rankin score and the other patients’ demographic characteristics.
|
Table II. Correlations between participation restriction, and patients’ demographic characteristics |
||||||||
|
Characteristics of patients |
Work impact n = 44 (15.2%) |
Odds ratio [95% confidence interval] |
Social impact n = 118 (28.7%) |
Odds ratio [95% confidence interval] |
||||
|
Age, years, mean (SD) |
42.25 (14.24) |
50.08 (18.09) |
||||||
|
p = 0.06 |
0.97 [0.95–1.00] |
p = 0.08 |
0.85 [0.90–1.25] |
|||||
|
Sex, n (%) |
||||||||
|
Male |
25 (56.8) |
61 (51.7) |
||||||
|
Female |
19 (43.2) |
57 (48.3) |
||||||
|
p = 0.22 |
1.56 [0.77–3.15] |
p = 0.01* |
1.68 [1.09–2.58] |
|||||
|
Health insurance, n (%) |
||||||||
|
No |
28 (63.6) |
94 (79.7)) |
||||||
|
Yes |
16 (36.4) |
24 (20.3 |
||||||
|
p = 0.01* |
3.69 [1.80–7.54] |
p = 0.02* |
1.08 [1.06–3.33] |
|||||
|
Marital status, n (%) |
||||||||
|
Single |
14 (31.8) |
36 (30.5) |
||||||
|
Married |
30 (68.2) |
82 (69.5) |
||||||
|
p = 0.29 |
4.22 [0.95–2.36] |
p = 0.56 |
0.72 [0.23–4.27] |
|||||
|
Education level, n (%) |
||||||||
|
More than one year |
31 (70.5) |
51 (43.2) |
||||||
|
No education |
13 (29.5) |
67 (56.8) |
||||||
|
p < 0.01* |
4.13 [2.05–8.30] |
p = 0.91 |
0.97 [0.45–7.26] |
|||||
|
Origin, n (%) |
||||||||
|
Urban |
34 (77.3) |
82 (69.5) |
||||||
|
Rural |
10 (22.7) |
36(30.5) |
||||||
|
p = 0.07 |
1.22 [0.98–1.77] |
p = 0.40 |
1.82 [0.55–2.33] |
|||||
|
Work status, n (%) |
||||||||
|
Active |
290 (70.6) |
72 (61) |
||||||
|
Non-active |
121 (29.4) |
46 (39) |
||||||
|
– |
– |
p < 0.01 |
4.91 [2.72–8.90] |
|||||
|
Monthly household income level |
||||||||
|
Less than 499 USD |
35 (79.5) |
107 (90.7) |
||||||
|
≥ 500 USD |
9 (20.5) |
11 (9.3) |
||||||
|
p < 0.01* |
4.32 [1.86–10.00] |
p = 0.15 |
2.92 [0.15–5.46] |
|||||
|
Medical condition category, n (%) |
||||||||
|
Communicable disease |
||||||||
|
Yes |
2 (4.5) |
7 (5.9) |
||||||
|
No |
42 (95.5) |
111(94.1) |
||||||
|
p = 0.55 |
0.72 [0.35–6.38] |
p = 0.93 |
0.25 [0.15–9.36] |
|||||
|
Non-communicable disease |
||||||||
|
Yes |
35 (79.5) |
103 (87.3) |
||||||
|
No |
9 (20.5) |
15 (12.7) |
||||||
|
p = 0.02* |
2.63 [0.16–0.89] |
p = 0.34 |
3.28 [0.72–5.19] |
|||||
|
Injury |
||||||||
|
No |
37 (84.1) |
8 (6.8) |
||||||
|
Yes |
7 (15.9) |
110 (93.2) |
||||||
|
p < 0.01* |
9.11 [2.75–30.23] |
p = 0.13 |
0.53 [0.23–6.27] |
|||||
|
*p < 0.05. USD: US dollars; SD: standard deviation. |
||||||||
Estimation of rehabilitation care needs
The number of patients whose medical condition justified some form of rehabilitation support, according to their diagnoses and impairments, was estimated as 153 (37.2%).
Physiotherapists were the most needed rehabilitation professionals, with an estimate of 149 (36.2%) patients needing their intervention. Occupational therapy would be beneficial for 84 (20.4%) patients, orthotics and prosthetics for 65 (15.8%) patients, social intervention for 49 (12%) patients, and speech therapy for 35 (8.5%) patients.
The patients’ orientation towards inpatient or outpatient rehabilitation support was determined according to the decision tree shown in Fig. 3. According to their limited autonomy level (Rankin scale ≥ 4), the need for more than 2 therapists’ intervention, or their geographical remoteness from medical and rehabilitation facilities, 101 (24.5%) patients were eligible for inpatient rehabilitation support.
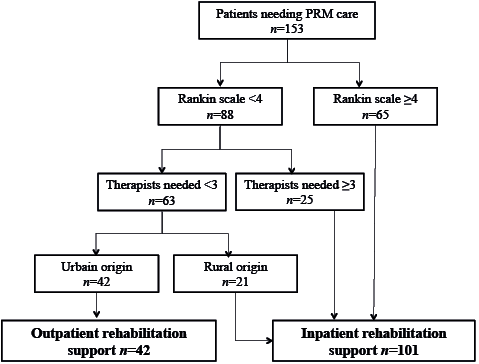
Fig. 3. Decision tree for in/outpatient rehabilitation support orientation.
DISCUSSION
This is the first study to characterize aspects of disability among Moroccan hospitalized patients and to address their specific rehabilitation needs. It was conducted in one of the largest and best equipped public hospitals in the country, which has a total capacity of 683 beds, serving the region of Fes-Boulmane with a population of more than 1.5 million. The study was exhaustive among all the hospital departments within the main geographical site. Our study population was characterized mainly by the young age of the patients (mean age 47.75 years), their lack of education (58.39% were illiterate) and their modest financial resources (71.29% living with a monthly household income of less than 200 USD). These characteristics should be considered carefully in the development of any rehabilitation projects intended for this specific population.
As a developing country, and due to its demographic transition driven by socio-economic development, Morocco has been facing an epidemiological transition, with a substantial increase in non-communicable diseases, which weigh heavily on the healthcare system. This fact is illustrated in our findings, with 89.5% of the hospitalized patients being treated for non-communicable diseases.
We tried to approach different aspects of disability in our study population, including impairments, activity limitations and participation restrictions. Impairments were largely dominated by pain, which is known for its negative effect on quality of life (9). Pain was reported by 41.6% of our patients. This is a lower rate than that found in previous studies, conducted in developed countries, reporting pain prevalence among inpatients ranging from 48.5% to 91% (10–13), and suggesting a possible socio-cultural impact on the perception of pain (14). Other substantial impairments were led by sensory-motor deficits and joint ROM limitations, which dramatically interfere with major human physical functions such as walking and grasping. Dysphagia and chest congestion might be life threatening, and should therefore be addressed quickly by applying efficient rehabilitation care. Bladder dysfunction and pressure ulcers were most likely underestimated, because on the day of the study there were no spinal injury patients, who have the highest risk for these impairments.
As expected, activity limitations were dominated by gait and balance disorders. Gait limitations would lead to participation restrictions in most medical conditions. When the patient can no longer walk independently and efficiently, he/she will quickly limit his/her movements inside the home, and offering a wheelchair would rarely solve the problem. Indeed, the inaccessibility of urban infrastructure to wheelchairs in most Moroccan cities, let alone rural regions, might discourage the person even more from going outside. Since people with disabilities are unfortunately still stigmatized in Moroccan culture, both disabilities and anything that might refer to them (e.g. wheelchairs) are often hidden from view.
Loss of autonomy in taking care of oneself (grooming, dressing and feeding) is very difficult to manage in daily life, as it leads to dependence on other people for the body’s basic needs. This is a delicate situation, causing suffering for both the patient, who may regard themselves as a burden on others, and the caregivers (spouse, parents, children, and sometimes siblings), who often undergo upheaval in their own lives in order to meet the new challenge of caring for a disabled adult family member (15).
In the whole study population 28.7% of patients reported a negative impact of their medical condition on their social life or, in other words, they experienced a significant restriction in their social participation.
Restriction in work participation was reported by 15.2% of patients with an active work life. This negative impact on work life was more common in patients with low household income and those lacking health insurance. People in these categories are most likely to have physically demanding jobs, and would probably experience a significant limitation in performance due to physical impairments. Participation restriction in work life is a good argument that rehabilitation care is beneficial not only for the individual but also for the whole society (3).
According to the nature of their impairments, 153 (37.2%) patients would need rehabilitation support with the intervention of at least 1 rehabilitation professional. Physiotherapy was the most needed intervention in our population, as in most physical rehabilitation scenarios. However, it remains an extremely underdeveloped discipline, with only 305 physiotherapists working for the Moroccan public health system in 2010, serving a population of 30 million (7). Occupational therapy was the second most needed expertise, and would be important in improving rehabilitation services, especially regarding upper extremity rehabilitation and environmental adaptations, both at home and at work. Unfortunately, occupational therapy does not exist in Morocco at present. We therefore recommend that Moroccan universities include this highly needed discipline in their courses. Other rehabilitation professions need similar attention, because they are also insufficiently developed to answer the huge population demand in Morocco. Indeed, in 2010 there were only 47 prosthetists and 45 speech therapists in the public health system (7).
We estimated that 57% of the patients needing rehabilitation should be hospitalized for different reasons, either because they were highly dependent and would be extremely difficult to transport every day or every other day to the rehabilitation facility, or because they needed the intervention of 3 or more professionals, or because they lived far from the hospital and could not easily commute. In the Moroccan health system, even though there is a high level of need for inpatient rehabilitation, it is not currently considered seriously. As stated above, only 5 out of 21,734 hospital beds in the public health system (0.02% of all beds) are dedicated to rehabilitation. There were no PRM specialists to run inpatient rehabilitation departments in the Moroccan public health system before the early 2000s and up to 2009 there were only 5 (16). Most Moroccan PRM specialists (as many as 50 up to 2009) run private practices, which are not always affordable for the average Moroccan citizen who would seek public health medical assistance. However, the situation is changing rapidly and there are currently more than 20 public health PRM specialists in Morocco, including 6 university professors, who could manage inpatient rehabilitation activity. On the other hand, inpatient rehabilitation might not be the best rehabilitation approach for health systems with limited resources, like the Moroccan one, because the duration of stay is long and costly. Alternatives should therefore be provided for highly disabled patients discharged from neurology and neurosurgery wards (550 public health beds) to their homes, who are returned to their uneducated and unprepared families to care for, which often results in poor medical and functional outcomes. According to the United Nations Convention on the Rights of Persons with Disabilities, ratified by Morocco in 2009, persons with disabilities should be given the right to get the same standard of medical care offered to other patients (17), and inpatient rehabilitation is almost necessary to achieve this goal. In a system that accepts keeping a patient hospitalized for weeks until he undergoes a non-urgent computed tomography (CT) scan, because he lives so far from the hospital and would not be able to afford to return for the scan, how can we discharge a highly dependent, stroke patient with a prescription for 3 times/week physiotherapy to be performed in an ambulatory rehabilitation centre?
Creating inpatient rehabilitation departments does not necessarily mean constructing new buildings or providing unaffordable funds immediately. A little more organization would help to start inpatient rehabilitation care, especially as the occupancy rates in Moroccan hospitals are not very high, at an average of 61% in 2011 (5).
Study limitations
This study has some limitations that should be taken into account when interpreting the results. The study was cross-sectional in nature and was conducted on a single day. The prevalence of disability in hospitalized patients in the present study may be underestimated because of the exclusion of patients who were absent from the ward (operating room, radiological examination, etc.) at the time of the interview. On the other hand, the prevalence of some impairments was probably underestimated (e.g. ROM limitations), because they were not clinically checked unless they were already mentioned in the patient’s chart. However, despite its probable underestimation, the prevalence of disability among adult hospitalized patients was high enough to justify the introduction of organized inpatient rehabilitation.
Conclusion
This study revealed that disability is very common among hospitalized Moroccan patients, and that more than half of those sustaining disability should not be discharged home, but need more follow-up care and rehabilitation support, which cannot be optimally achieved without inpatient activity. As an inpatient rehabilitation discipline PRM is not as expensive as other medical or surgical disciplines, and yet it is a good medical and social investment that deserves more consideration from Moroccan medical authorities.
REFERENCES

