Ji Won Lee, MD1, Yoon Sik Jo, MD2, Jae Sung Park, MD3, Jong Moon Kim, MD1 and
Shin Kyoung Kim, MD1
From the Departments of 1Rehabilitation Medicine, 2Neurology and 3Neurosurgery, School of Medicine,
Konkuk University, Chungju, Republic of Korea
OBJECTIVE: Prolonged fever is rare in patients with spinal cord injury. Fever has been shown to be associated with heterotopic ossification, but prolonged fever is very rare. We report here a case of prolonged fever in a tetraplegic patient who was eventually diagnosed with heterotrophic ossification, and provide a review of the literature. Treatment with sodium etidronate resolved the fever.
CASE REPORT: A 51-year-old man with C3 tetraplegia developed prolonged fever (37.5–39.4°C). Fever workup did not reveal a definite origin of the fever. Non-infectious disease was suspected. The patient was diagnosed with heterotopic ossification after 3-phase bone scintigraphy. Oral sodium etidronate treatment was started immediately at a dose of 20 mg/kg/day after diagnosis. On the 14th day of administration, the patient’s body temperature decreased to the normal range and remained stable.
CONCLUSION: Heterotopic ossification should be taken into consideration when examining patients with spinal cord injury who have prolonged fever. This case shows that heterotopic ossification can be treated successfully with sodium etidronate.
Key words: heterotopic ossification; spinal cord injury; fever; tetraplegia; bone scan.
J Rehabil Med 2015; 47: 669–671
Correspondence address: Shin Kyoung Kim, Departments of Rehabilitation Medicine, School of Medicine, Konkuk University, 620-5 Gyohyeon 2-dong, Chungju, 380-704, Republic of Korea. E-mail: kimnerve@hanmail.net
Accepted Apr 14, 2015; Epub ahead of print Jun 12, 2015
Introduction
Fever is a common symptom in patients with spinal cord injury (SCI), with an incidence of 34–50% during acute rehabilitation (1). The most common causes of fever in patients with SCI are respiratory and urinary tract infections. Other infections frequently observed include pressure wounds, bloodstream infections and osteomyelitis (2). Non-infectious causes of fever in patients with SCI include deep venous thrombosis, pulmonary embolism, heterotopic ossification (HO) and thermoregulatory dysfunction (3). Differentiating the causes of fever is crucial in clinical practice. Fever can be progressive, fatal and unresponsive to antipyretic agents and cooling interventions (4).
HO refers to bone formation in soft tissue where bone is not normally present (2). It is a frequent complication after SCI. Common presentations include swelling, warmth, erythema, and tenderness of involved joints. However, prolonged fever is rare in patients with SCI.
Although fever has been shown to be associated with HO, prolonged fever is very rare.
We report here a case of a patient with tetraplegia and prolonged fever who was diagnosed with HO, and provide a literature review. The patient was treated successfully with sodium etidronate.
Case Report
A 51-year-old man presented at our emergency department with symptoms of sudden paralysis in all limbs after falling from a 2-m high ladder.
Brain computed tomography (CT) and X-ray were obtained to exclude the possibility of traumatic brain lesions, which showed no definite abnormal findings. X-ray, CT and magnetic resonance images of the cervical spine revealed a fracture of the C5 vertebral body, a high-signal intensity epidural haematoma extending from the C2 to C5 vertebrae. Initial physical examination showed SCI below the C3 level. Intravenous methylprednisolone was administered within 8 h of injury and hourly thereafter for 24 h. Three hours after admission, the patient underwent decompressive laminectomy of the C3–C5 spine.
On the 14th hospital day, fever above 38°C developed once or twice a day. The patient underwent fever workup, including white blood count, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), electrolyte, aspartate aminotransferase (AST), alanine aminotransferase (ALT), r-glutamyl transpeptidase (r-GTP), total bilirubin, blood urea nitrogen (BUN)/creatinine, rheumatoid arthritis (RA) factors, urinalysis, urine microscopy, cerebrospinal fluid analysis, and microbial cultures of blood, sputum (real-time tuberculosis polymerase chain reaction (TB PCR), acid-fast bacilli stain, etc.) and urine, which gave no definitive clue as to the origin of the fever. X-ray and chest CT were performed to rule out pneumonia and pulmonary embolism, and did not reveal any abnormalities. Despite consultation with the department of infectious diseases, the origin of the fever remained ambiguous and unresponsive to empirical antibiotic therapy (cefbuperazone + clindamycin, amoxicillin + clavulanate, ceftazidime, meropenem). Under the clinical impression of drug-related fever, all non-essential drugs (e.g. the antidepressant, tianeptine) were discontinued. However, the patient’s body temperature still fluctuated between 37.5°C and 39.4°C. On the 33rd hospital day, the patient was transferred to the department of rehabilitation medicine.
His neurological status was C3/C3 based on the American Spinal Cord Injury Association Impairment scale A. Slight limitation of passive range of motion was observed in the shoulder and hip joints with swelling and erythema. Chest CT and fever workup, including tumour markers and D-dimer, were repeated. The results gave no clue as to the origin of the fever. Proper room temperature was maintained to rule out poikilothermia. Serum alkaline phosphatase (ALP) and CRP (serum ALP 38 IU/l, normal: 32–91 IU/l; CRP 0.21 mg/dl, normal: 0–0.75 mg/dl) were within the normal range, but serum ESR was elevated (ESR 34 mm/h, normal: 0–9 mm/h). X-ray showed ossification in the left shoulder joint (Fig. 1), but otherwise normal findings. Three-phase bone scintigraphy was performed and revealed increased blood pooling and bone uptake in the proximal lateral aspect of the bilateral hip and shoulder joints (Fig. 2).
Fig. 1. X-rays of both shoulder joints showing ossification (arrows) in the left shoulder joint.
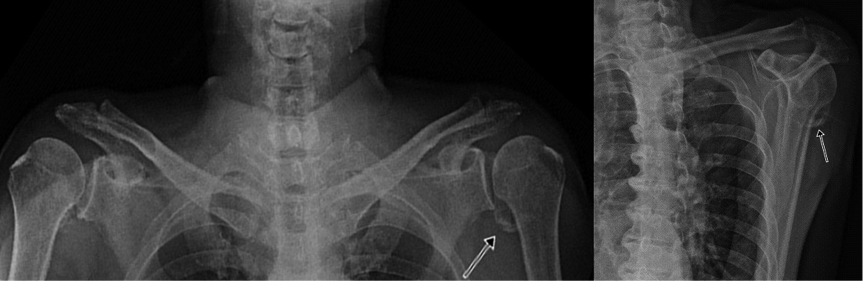
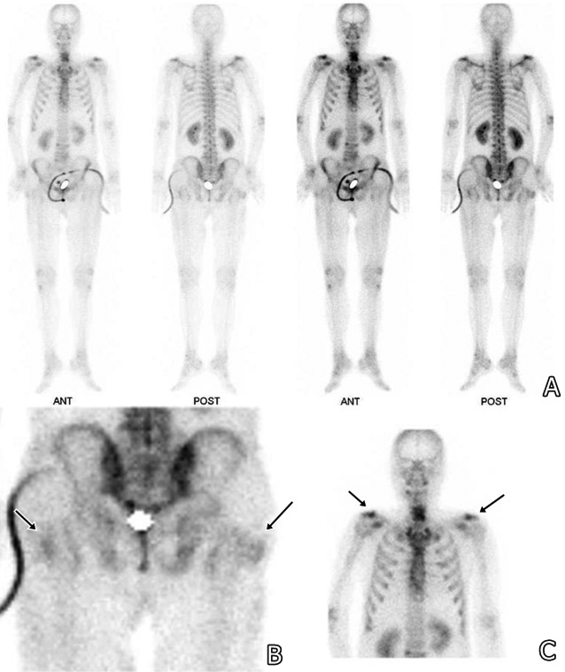
Fig. 2. Three-phase bone scintigraphy showing increased blood pooling and bone uptake (arrows) in the proximal lateral aspect of the bilateral hip and shoulder joints. (A) Whole body image; (B) bilateral hip joints; (C) bilateral shoulder joints.
Treatment with sodium etidronate was started at a dose of 20 mg/kg/day immediately after the diagnosis of HO (69th hospital day). On the 74th hospital day, the patient’s body temperature showed a tendency to decrease. On the 83rd hospital day, his body temperature decreased to the normal range and remained stable (Fig. 3).
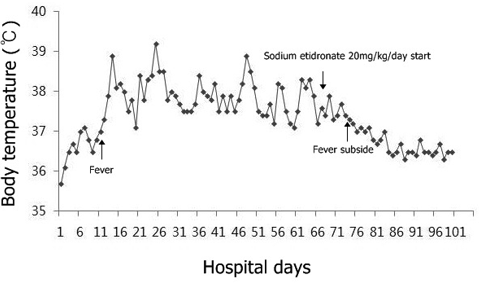
Fig. 3. Body temperature graph showing a decreasing tendency after administration of sodium etidronate.
DISCUSSION
Patients with SCI have a high risk of developing HO, with an incidence of 1–50% (5). HO in patients with SCI commonly occurs within the first 2 months of injury (6). Because of the non-specificity of clinical signs and symptoms, a diagnosis of HO is difficult in the initial stage. HO refers to bone formation within the soft tissue, and has a pathogenesis distinct from metastatic and dystrophic soft-tissue calcification. Some investigators have reported that the sera of patients with HO has a significantly higher level of osteoblast-stimulating factor (2). Other factors for developing HO include hypercalcaemia, tissue hypoxia, changes in sympathetic nerve activity, prolonged immobilization, remobilization, and disequilibrium of parathyroid hormone and calcitonin (2).
Early in the course of the disease, HO may cause pain (if sensation is intact), fever, swelling, erythema, and decreased joint mobility. In the early inflammatory phase, this condition may mimic cellulitis, thrombophlebitis, osteomyelitis or tumours (7). A systemic febrile reaction is known to coexist with HO, and low-grade fever may occasionally persist for a couple of weeks. However, prolonged and persistent fever for 2 months is very rare. The mechanism of fever underlying HO is unclear; it is possible that mediators involved in the process of HO could include endogenous pyrogens that trigger a febrile reaction (8).
The diagnosis, using simple X-ray, ultrasonography, 3-phase bone scintigraphy, elevated ALP, and elevated 24-h prostaglandin E2, can be used as predictors of the onset of HO. ALP has been suggested as a useful screening tool for HO (6). Unfortunately, ALP levels cannot be used to obtain clinical information about maturity or recurrence of HO because the values may be normal in the presence of active HO (2) or may remain elevated for years. The use of sonography has also been assessed in order to diagnose HO prior to radiographic evidence (9, 10). Previous studies suggest that ultrasonography can be used readily as the first-line imaging modality for the detection of HO, with several advantages, such as having high spatial resolution and no ionizing radiation, and is repeatable, widely available, and cheaper than computed tomography and magnetic resonance imaging (11, 12). Three-phase bone scintigraphy is positive with increased uptake of osteotropic radionucleotides, and therefore utilizing it in the early stage phase of HO can be very helpful. Three-phase bone scintigraphy has proven more sensitive than plain radiography in detecting early HO, becoming evident in the first and second phase of the 3-phase bone scintigraphy 2–6 weeks before diagnosis on plain radiographs (9).
Complications of HO include peripheral nerve entrapment, pressure ulcers, and functional impairment if joint ankylosis develops. Therefore, early treatment of HO is extremely important. Diphosphonates and non-steroidal anti-inflammatory drugs, such as indomethacin and ibuprofen, have been used for treatment of HO (13). Sodium etidronate is also used to treat SCI-related HO. It inhibits osteoid mineralization, binds to calcium phosphate, and prevents hydroxyapatite crystallization. Non-steroidal anti-inflammatory drugs (including indomethacin) demonstrate greatest efficacy in prevention of HO when administered early after a SCI, while bisphosphonates are the intervention with the strongest supportive evidence once HO has developed. It appears to be most effective if treatment is initiated earlier when the 3-phase bone scintigraphy is positive and radiographs are normal (14). Thus, we started oral treatment with sodium etidronate immediately after 3-phase bone scintigraphy indicated suspected HO. The prolonged fever was treated successfully and other complications were prevented.
The present case helps us to understand the association of HO with prolonged fever in patients with SCI without other symptoms or abnormal laboratory findings (e.g. ALP). HO should be considered as a possible cause of prolonged fever in patients with SCI. This case shows that HO can be treated successfully with sodium etidronate. However, more research into the association between sodium etidronate and HO is needed to confirm these results.
REFERENCES

