Corrie Myburgh, PhD1, Eleanor Boyle, PhD1,2, Henrik H. Lauridsen, PhD1, Lise Hestbaek, PhD1,3 and Alice Kongsted, PhD1,3
From the 1Institute of Sports and Clinical Biomechanics, University of Southern Denmark, Odense, Denmark, 2Dalla Lana School of Public Health, University of Toronto, Toronto, Canada and 3Nordic Institute of Chiropractic and Clinical Biomechanics, Odense, Denmark
Study design: Phenomenological, qualitative investigation. The discord between commonly used outcome measures and patients’ self-perceived recovery is problematic in the investigation and rehabilitation of low-back pain-related disorders. To better understand the course and development of this costly and disabling condition, the complex process of patient recovery requires further elucidation.
OBJECTIVE: To explore issues and experiences impacting retrospective, self-appraised recovery.
METHODS: Semi-structured interviews were conducted with 32 purposively sampled individuals, after which computer-assisted substantive categorization and thematic analysis was performed.
RESULTS: Self-appraised status could be determined as “recovered” for 17 respondents, “unsure” for 6, and “not recovered” for 9. Recovery/non-recovery hinged on continued pain-related issues and the perception that injury/trauma made recovery impossible. Individuals who had difficulties relating the recovery construct to their context as well as those who were sceptical of pain-free periods were unable to appraise their status.
CONCLUSION: This investigation confirms that pain is central to the resolution of recurrent low-back pain associated disorders. However, recovery also involves “redefinition” and “readjustment”. In the investigation and rehabilitation of ambiguous, regional musculoskeletal disorders, our results provide further sensitizing concepts, derived through naturalistic observation, that are useful in the development of a more comprehensive explanatory framework of patient recovery.
Key words: exploratory methods; qualitative research; health outcomes; musculoskeletal disorders; recovery.
J Rehabil Med 2015; 47: 00–00
Correspondence address: Corrie Myburgh, Department of Sports Science and Clinical Biomechanics, University of Southern Denmark, Campusvej 55, DK-5230 Odense M, Denmark. E-mail: cmyburgh@health.sdu.dk
Accepted Apr 24, 2015; Epub ahead of print Jul 1, 2015
INTRODUCTION
Musculoskeletal disorders of the lower back often referred to simply as low-back pain (LBP), remain a ubiquitous group of health problems that place an enormous burden on society (1–4).
According to the World Health Organization’s (WHO) vision, successful rehabilitation of LBP disorders is the culmination of a process that enables individuals to:
“Reach and maintain their optimal physical, sensory, intellectual, psychological and social functional levels. Rehabilitation provides disabled people with the tools they need to attain independence and self-determination (5).”
Consensus exists that this ambitious, multi-dimensional perspective of rehabilitation requires a systematic distillation of relevant, reliable and valid patient-centred outcomes in order to minimize the risk of erroneous measurement and misguided interpretation of observed phenomena (6–8). However, despite the efforts of the WHO to facilitate standardization through frameworks such as the International Classification of Functioning, Disability and Health (ICF), some concepts reflective of patients’ notions of their back problems have proven difficult to operationalize across health-related disciplines (9, 10). In this regard, patient recovery is an interesting case in point.
A popular approach to the observation of patient recovery in the context of ambiguous musculoskeletal conditions, including LBP, has been to operationalize the recovery construct through proxy measures, such as symptom attenuation (especially pain), activity limitation or work participation indices (8, 11, 12). This trend extends to the ICF, where investigators tend to de-emphasize contextual and environmental outcomes by using Brief Core Sets (7, 8, 13, 14). And whilst well-suited to disease-oriented models aimed at condition resolution, there is a growing awareness that this type of approach has limitations when dealing with patient recovery. Specifically, it seems that when LBP exists for a protracted period; a discord between commonly observed outcomes and self-perceived patient recovery starts to occur, which in turn complicates interpretation (7, 11, 12, 15, 16).
In recent years, studies grounded in a more naturalistic research approach have begun to elucidate patient recovery (17). In particular, observations in several qualitative investigations strongly suggest that individuals do not use pain-related symptom attenuation as the sole cognitive anchor from which to judge their own recovery status (10–12, 14, 15). Rather, patient recovery is likely to be appraised through the individual’s unique and changing set of life experiences, which relate as much to their search for happiness and satisfaction as to a change in disease state (12, 16, 18).
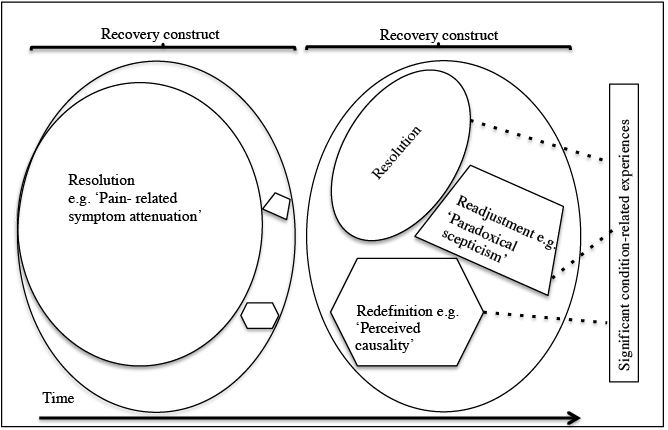
Conceptually, a strong argument has been made that, in the short-term, recovery is completely (or almost completely) operationalizable through outcomes relating to the resolution of a particular condition (Fig. 1) (16, 19). However, due to individual lived experiences, at least 2 other domains; readjustment and redefinition gain importance as the condition becomes chronic or recurrent, thus increasing the complexity of the recovery construct (12, 19). The resultant effect is a relative “shrinking” of the resolution domain, as disease resolution now shares the recovery construct space with 2 other domains.
Notwithstanding the above, fundamental questions regarding the nature of patient recovery require further exploration; in particular, the domains relevant to the recovery construct that lie beyond traditional measures of disease resolution, yet are integral to comprehensive patient rehabilitation.
Consequently, the purpose of our investigation was to retrospectively explore the recovery experiences of individuals on different pain trajectories after 12 months of observation aimed at quantifying the course of their LBP. The specific objectives were to generally describe retrospective, self-appraised patient recovery and more specifically to gain insight into the factors determining recovery and non-recovery.
MATERIALS AND METHODS
Design
A phenomenological, qualitative design was considered appropriate, considering our interest in capturing the lived experiences of individuals from an established conceptual perspective (8, 20).
Participants
Through our participants, we aimed to observe a diverse, yet balanced set of reflections from people with different pain-related experiences over a 12-month period. We solicited responses from individuals enrolled in a longitudinal cohort study, which investigated the course of LBP in the Danish primary care setting. The characteristics of this cohort is described in detail elsewhere, but in brief, all participants were recruited from either general practices or chiropractic practices, had LBP with or without nerve root involvement, were aged between 18 and 65 years and were functionally literate in Danish (21).
Our sampling protocol followed a maximum variation approach (22). This was achieved through a profile matrix generated by 1 of the research team (AK). The profiles, obtained from data collected during the cohort study, were based on the number of weekly LBP days measured by Short Message Service (SMS) tracking over a period of 1 year. SMS tracking has previously been demonstrated as both a valid and reliable method for survey-type data collection (23). The profiles were termed “mainly recovered” (mean 14 days LBP during one year), “improved and fluctuating” (mean 40 days), “unchanged intermediate” (mean 152 days), and “unchanged severe” (mean 353 days) (24).
Interviewers, blind to the particular pain profiles of individuals, were provided with a list of study participants who had completed their 1-year follow-ups and were thus eligible for inclusion (21, 25). Three attempts were made to contact a particular individual (on different weekdays). In the event that the individual could not be contacted, they were excluded and the next person on the list was contacted for potential inclusion.
Data collection
Semi-structured interviews were conducted with respondents. Telephonic, rather than face-to-face interviews were preferred, because of the wide geographical spread of respondents in the cohort study, which made conducting personal interviews unfeasible. Moreover, previous studies indicate that data obtained in face-to-face and telephonically interviews do not differ from each other when perceptions are being studied (26, 27). Thus, despite the negative bias associated with the latter, the 2 methods should be considered equally valid in this context.
Interview questions were partly adapted from previous investigations conducted in this area (12, 15). As a result our interview schedule consisted of 3 core questions and 2 sub-questions relating specifically to the respondent’s rationale for determining recovery status (Table I). Interviews were recorded, transcribed verbatim and then translated into English.
|
Table I. Interview schedule |
|
1. Are your back problems over? If yes, what does saying you are ”over it” mean to you? If no, what should change to make you experience your back problem as being over? |
|
2. To what extent have your back problems affected you? |
|
3. Has anything special occurred during the last 12 months in relation to your low back problems? |
Sampling was concluded after thematic data saturation was achieved across the sampling framework. In this regard, we coded the initial interviews inductively and then applied the code list deductively to subsequent interviews until, through constant comparison, no new codes were generated (28). Moreover, an a priori decision was taken to populate each of the 4 SMS profile groups with at least 5 individuals, so as to facilitate comparisons between emergent sub-groups.
Data analysis
The data was coded to facilitate general thematic emergence and enable substantive categorization of recovery status (29). In this regard, 2 research technicians and a research team member (CM) each generated a code list inductively from the first 5 interviews by allocating descriptive labels to key phrases or sentences. In the event that new codes emerged they were applied to previously coded interviews (28). After removing coding duplication and clarifying code definitions, a resultant composite code list was used by (CM) to code the remaining interviews deductively. To additionally ensure coding consistency and transparency, a second research team member (EB), independently coded the interviews and reviewed the key quotes generated using the same composite code list (22). The 2 research team members subsequently met to consider and resolve discrepancies and categorized the respondents in 1 of 3 emergent sub-groups, namely “recovered”, “not recovered” or “unsure”. To facilitate thematic emergence descriptive labels were linked, code families created and visual representations (networks) of the data built. All coding and thematic analysis was conducted through the use of computer-assisted qualitative data analysis software (CAQDAS) (Atlas Ti version 6.2) (http://www.atlasti.com) (30).
All data were collected confidentially and were anonymized for presentation. A quotation identification (QID) system was used to present verbatim English translated text data. For example, the QID (P2:7:10) refers to respondent 2, it is the seventh quote created in the interview and can be found in line 10 of the transcript.
Ethical approval was sought through the scientific ethics committee of the Region of Southern Denmark and was conducted in compliance with the stipulations of the Danish Data Protection Agency for the procurement and storage of anonymized interview data.
RESULTS
Interviews typically lasted around 20 min. A re-interview was conducted with 1 respondent because of poor voice clarity. Thematic data saturation occurred after 9 interviews; however, a further 3 buffer interviews were conducted. The final number of interviews conducted was 32 (23 from chiropractic practices and 9 from GPs) with an even distribution being achieved across individual course profiles (Table II).
|
Table II. Sample by Short Message Service (SMS) track low-back pain (LBP) course profile |
|
|
Mean number of days with LBP during 1 year |
Participants n |
|
SMS Profile 1 (14 days) |
10 |
|
SMS Profile 2 (40 days) |
7 |
|
SMS Profile 3 (152 days) |
7 |
|
SMS Profile 4 (353 days) |
6 |
|
SMS Profile unknown* |
2 |
|
*Two respondents had too many missing values to be profiled through SMS tracking. LBP: low back pain. |
|
From the general analysis, 2 themes emerged, these being “pain and vigilance” and “perceived causality”. In addition, the sub-group analysis led to a third concept, the notion of “paradoxical scepticism” being raised to the level of a theme.
Of the 32 subjects interviewed, 17 could be substantively categorized as recovered, 9 were not recovered, and the remaining 6 felt unsure of their status (Table III). After categorization of self-appraised recovery status, 2 additional themes were developed in relation to the 3 sub-groups; namely, “anchors for recovery” and “recovery uncertainty”.
|
Table III. Key quotes by recovery status for all participants |
|||
|
PN |
RS |
Key quotes |
Reference |
|
7 |
Î |
What should change? Well, that I do not feel pain or anything. |
(P7:4:8) |
|
8 |
Î |
… I shouldn’t feel pain every day. |
(P8:4:8) |
|
14 |
Î |
… , well the pain should change, right? |
(P14:4:8) |
|
15 |
Î |
… it should change in a way that I never felt pain then. |
(P15:4:9) |
|
21 |
Î |
Er, give me a new back. |
(P21:4:12) |
|
22 |
Î |
… I frankly don’t know. I broke my back. I have had an unstable rupture of the back |
(22:4:8) |
|
23 |
Î |
… then I should be rid of the pain, right. And I’m not. |
(P23:4:8) |
|
24 |
Î |
… it is just ordinary wear and tear, I think I’ll have to get used to me having those injuries…, that pain I feel. |
(P24:4:8) |
|
28 |
Î |
That my pain disappeared. |
(P28:4:12) |
|
1 |
? |
In the broad outline, I would say. It’s hard to tell, not a 100%. I can feel it once in a while…I must retrain. I wouldn’t say I feel pain, but I’m sore. That is, I can do most things; I take care when lift, I take care when I run and if it starts hurting, I stop. |
(P1:5:9) |
|
10 |
? |
Er, yes, not quite. The herniated disc, one does not recover completely from that I assume. One doesn’t, that’s just so… I haven’t had pain as fierce as I had before …[but] there have been days…where I have been hindered in doing some things, but it has only been short periods of time. |
(P10:5:13) |
|
13 |
? |
It isn’t that bad anymore at all. But, due to me being somewhat tall and a little weak, then I almost always feel a little pain in my back. |
(P13:4:4) |
|
18 |
? |
… I don’t know, I have recurrent problems I would say, it isn’t so that I have problems constantly, I have periods when it is not so good. |
(P18:4:12) |
|
29 |
? |
One cannot say that I’m decidedly recovered from them, but, er, I can feel them once in a while, right. I have to think carefully about what I run around doing and so. |
(P29:4:4) |
|
30 |
? |
… both yes and no because the kind of back problems I had was the kind that came and disappeared,… |
(P30:4:4) |
|
2 |
P |
Yes! ... I do not have pain, not anymore. |
(P2:5:9) |
|
3 |
P |
Yes, in broad outline. I do not feel pain anymore, only once in a while when I get hold [of something] in a wrong way; otherwise I do not feel pain. |
(P3:5:9) |
|
4 |
P |
I do not feel the pain I felt a year ago. That is, once in a while I get a sort of feeling that now something is, something is about to be wrong, but then it never comes to more than that,… |
(P4:5:9) |
|
5 |
P |
I’m all right now,… I haven’t felt anything from it today. |
(P5:8:20) |
|
6 |
P |
I feel fine … when I take care and know what I can do and what I can’t. |
(P:6:4:8) |
|
9 |
P |
It doesn’t hurt anymore. |
(P9:5:9) |
|
11 |
P |
I don’t run around with the problem permanently.. |
(P11:4:4) |
|
12 |
P |
… it has simply disappeared and since then there hasn’t been anything at all. |
(P12:4:8) |
|
16 |
P |
I feel better, and [I] feel better with myself too. |
(P16:4:8) |
|
17 |
P |
I don’t feel it anymore. I don’t feel the inconveniences I had then anymore. |
(P17:4:8) |
|
19 |
P |
I do not have any trouble, I can only just feel it a tiny bit once in a while, but it that’s nothing that bothers me in any way. |
(P19:4:8) |
|
20 |
P |
… for the last half year I haven’t felt anything at all. |
(P20:4:8) |
|
25 |
P |
Yes, well, I am actually back to basic. |
(P25:12:12) |
|
26 |
P |
Yes,…it just turns up once in a while. |
(P26:5:9) |
|
27 |
P |
Yes,… it isn’t like the back problems have disappeared, but I keep them on a sufficiently low level… |
(P27:4:4) |
|
31 |
P |
… yes, yes I am, …it returns a little once in a while…[but] there are times, where I do not feel it. |
(P31:4:8) |
|
32 |
P |
Well, it was [only] something acute that came by. |
(P32:4:8) |
|
PN: primary document number; RS: recovery status; Î: not recovered; ?: unsure; P: recovered: |
|||
Pain and vigilance
For our participants, pain served both as a warning and a reminder of intense discomfort/suffering. This is illustrated by P1, who stated:
…[After] one and a half months had passed I thought it went fine again and I was out helping my friend move. I shouldn’t have done that because I went down the day after, … that was the worst pain I have ever had. It was in fact perhaps then I realized most clearly how much I had to take care (P1:37:37).
And whereas back pain per se might be self-limiting “…it came suddenly and it disappeared suddenly (P9:17:17)”, its global impact, at times, can be devastating:
[Back pain] affected me a lot, both physically and psychologically. It is a source of annoyance and there are many things one can’t do. …I have been fired, due to this thing with the back (P14:20:28).
Consequently, respondents displayed an awareness that “care” is required when performing activities of daily living, as according to P6: “I feel pain [so I] go around a little more quietly taking care (P 6:28:28)” and that vigilance against inappropriate physical activity contributes to coping. Accordingly, P5, P9 and P11 stated:
I have made such stupid movements, I think. Something like driving a garden tractor and then sitting too long time on it (P5:8:12).
It happens when I over-exert myself (P9:29:29).
It is mostly when I do too much physically (P11: 4:4).
Perceived causality
A “perceived cause”, for example evidence of tissue injury, emerged as an important issue for respondents as these appear to form an integral component of individual explanatory frameworks. While elaborating on the background to his/her injury, P27 stated:
I had a work injury, perhaps at the age of 30 years, … It wasn’t recognized as a work injury, but I think it was probably then I received my deathblow (P27:12:12).
This phenomenon appeared to be reinforced by a second-level diagnostic investigation, as according to P10 and P30:
The herniated disc, one does not recover completely from that, … that’s just how it is (P10:5:5).
and
…I don’t think I’ll ever recover fully from it, I don’t. I had X-ray pictures taken of my back once and they said, … but due to that condition one was liable to wear and tear, to have the back distorted by wear and tear that is. It’s in the back, that’s it (P30:41:41).
Significant traumatic events associated with LBP are apparently not limited to physical events only, as P28 clearly stated:
I have received treatment at a pain center and it didn’t help, … at the end they wanted to send me to a psychiatric emergency center because I was crying, … (P28:16:28).
Paradoxical scepticism
For respondents reporting an acute episode as part of their back pain history, fear of not recovering featured strongly:
…When you are lying there and can’t turn around in the bed at all, then you consider whether it will ever be all right again. [One worries] if it is something that will haunt one for the rest of [one’s] life. Will I be able to run again, will I be able to practice sports again? Will you be able to lift anything again at all?’ (P1:29:29).
And, while fear and anxiety tended to dissipate for respondents experiencing periodic LBP, it seems that they remain paradoxically sceptical of their backs during pain-free periods. As illustrated in the discourse of P6, individuals who are yet to perform what they perceive as high-risk activities or who have been unable to detect a predictable pattern to their pain appear to be particularly prone to this phenomenon:
Right now I’m really fine; I don’t feel anything. [But] perhaps suddenly this afternoon I could make a wrong movement and then it is back again…That is what is a little strange about it, I can work like a beast, right, without feeling anything, then … the day after it may come … (P6:40:40).
Anchors for recovery
When viewing the key quotes summarizing the recovery status of our study participants (Table IV), it became apparent that recovered individuals tended to anchor their perceived status mainly on pain “no longer being an issue”. Note that “not having issues” is not the same as being pain free. In this regard P19 stated:
I do not have any trouble, I can only just feel it a tiny bit once in a while, but it’s nothing that bothers me in any way (P19:6:8).
The “not recovered” respondents similarly anchored their perceived status in pain, continued pain that is. In addition, these individuals appeared particularly affected by perceived injury undermining their potential for full recovery. P21 and 22 illustrate this issue by stating:
…give me a new back… the herniations [must] disappear and the old injuries disappear, then it would be fantastic (P21:4:12).
and
...I frankly don’t know. I broke my back. I have had an unstable rupture of the back (22:4:8).
|
Table IV. Factors influencing self-appraised recovery status |
||||||
|
Recovery, status (n) |
Pain issues |
Perceived causality (injury and/or trauma) |
No pain issues |
Positive coping |
Paradoxical scepticism |
Recovery meaning uncertain |
|
Recovered (17) |
Î |
Î |
||||
|
Not recovered (9) |
Î |
Î |
||||
|
Unsure (6) |
Î |
Î |
||||
|
Indicate the main self-appraised recovery issues highlighted. |
||||||
However, as a counter example, P16 despite receiving a magnetic resonance image (MRI) scan, a diagnosis of “a herniated disc” and reported having “been through a lot”, P16 nevertheless states: “I have become fine and I hardly feel pain in the back anymore (P16:1:12)”.
It therefore appears that individuals who no longer experience issues with pain and/or have somehow coped effectively, might place less importance on the “perceived cause” of their back problems.
Recovery uncertainty
Respondents who exhibited difficulties in classifying themselves as, “recovered” or “not recovered” exhibited uncertainty in 3 distinct areas. First, the notion of recovery as a finite state was difficult to marry with their particular set of experiences. For example, P15 did not feel recovered, but immediately qualified this position by stating: “I wouldn’t say [I have recovered], but I feel better now than I did before… (P15:14:4).” Similarly, according to P18:
I have recurrent problems I would say, it isn’t so that I have problems constantly. I have periods when it is not so good (P18:4:12).
Secondly, it appears that individuals who were unsure of their own recovery status were particularly prone to the phenomenon described as “paradoxical scepticism”, above. And thirdly, some individuals rejected the notion that their back pain was abnormal and, as such, felt that they had nothing to recover from. This is illustrated by P13, who argues:
…when I received this questionnaire [completed at the start of the cohort investigation], then it was because I went to see a chiropractor for help. And it isn’t that bad anymore at all. But, due to me being somewhat tall and a little weak, then I almost always feel a little pain in my back (P13:4:4).
DISCUSSION
In exploring the determinants of recovery expectation from non-specific LBP of less than 8 weeks’ duration, Iles et al. (19) reported that progressive pain reduction was strongly indicative of increased recovery expectation. However, in their respective investigations focused on perceptions of recovery from recurrent LBP and chronic mechanical neck pain, Hush et al. (15) and Walton et al. (16) observed that recovery was not contingent on the absence of pain, but rather acceptable levels of symptom attenuation. Given the anchors used for self-appraised recovery, our results confirm these findings. Specifically, complete pain-related symptom attenuation initially anchors recovery; however, individuals appear to enter into self-negotiation regarding acceptable levels of pain-related symptom attenuation as their condition progresses.
We observed evidence of tissue injury and psychological trauma to be an important factor associated with non-recovery. This finding also appears to be consistent with recent observations in relation to recovery from neck and low back-related disorders and individual experiences with LBP in the broader sense (18, 19, 31). Iles et al. (19) observed that as a part of the individual’s lived experience, past injury/illness played an important role in determining recovery expectations. More specifically, previous injury was used as a means of comparison to appraise recovery expectation. Young et al. (31), using a phenomenological approach to further understand LBP recurrence in a working population, observed that integral to the individual’s “total experience” of their LBP is its history, which often featured a traumatic event(s) (31). Novel to our study is the weighting individuals assigned to tissue injury in the recovered vs non-recovered individual. In particular, the weighting of a perceived cause of pain appears to diminish when the individual experiences a combination of acceptable pain-related symptom attenuation and positive coping.
Hush et al. (15) and Young et al. (31) observed that LBP sufferers have a tendency towards managing “…the potential for pain…”, and also retain “…the anxiety of it [LBP]” even when their condition state is classified as “normal”. We similarly observed the paradox that absence of pain did not necessarily determine the classification of “recovered” and termed the phenomenon as “paradoxical scepticism” (15, 31). When viewing the responses from individuals who were unsure of their recovery status, our investigation suggests that residual fear/anxiety regarding the recurrence of pain represents a cognitive barrier to self-appraised recovery.
We contend that our observations are suggestive of behaviours commensurable with what is described under the framework of cognitive dissonance (32). It would appear that dissonance might be aroused in individuals who have had recurrent LBP and then start to experience extended pain-free periods. This challenges their beliefs that their condition is intractable, especially in cases where a perceived biological cause exists. If dissonance is not reduced by changes in belief, the individual might attempt to restore consonance through maladaptation, such as misperception, rejection or refutation of information (33). As a consequence the individual can acknowledge improvement, but never complete recovery.
With respect to the role of the recovery construct in LBP rehabilitation, our study makes 3 contributions to the current conceptual understanding (see also Fig. 1). Firstly, the importance of resolution, operationalized as pain-related symptom attenuation, is likely to change with time. The exact shape and magnitude of this change is unclear, but further exploration using currently available outcomes such as minimally important change (MIC) (34) and Patient Acceptable Symptom State (PASS) (35) might be useful in this regard. Secondly, “perceived causality” influences redefinition of the recovery construct, and by extension health, in the mind of the individual. In this regard, the patient-practitioner relationship is likely to play an important role. In particular, the rationale, interpretation and communication of second-level investigations require further investigation in this context. Thirdly, paradoxical scepticism suggests that the individual has experienced (experiences) significant fear and/or anxiety regarding the potential for future episodes of intense pain and therefore might develop behavioural mal-adaptations and/or imposed restrictions on their own recovery potential. Paradoxical scepticism is likely to impact on readjustment, as significant condition-related experiences serve to reinforce or diminish distrust/anxiety over time (32). It stands to reason that this phenomenon be countered during the clinical rehabilitation process.
Strengths and limitations
Our data stemmed from a large cohort of primary care sector patients, who we were sampled based on their individual LBP course profiles. This was a study strength as we were able observe a “severe” group (Table II), which made up a small portion of the original cohort.
This study’s credibility was enhanced by input of multiple researchers, both during coding and analysis. More specifically, the interviewers and researchers were naïve to responder status from the outset, and the coding and analysis procedure reduced the risk of strong, individual views, not reflected by data, penetrating the results. Qualitative studies are, by their very nature, subjective; however, the researcher(s) carries the responsibility of reporting data in a “neutral” manner, even though he or she may not personally agree with the participant’s perspective(s) (28). Given the methodological approach we followed, it is unlikely that views of an individual researcher could have systematically influenced the results generated.
The reader ultimately determines transferability; however, we contend that given the method of data collection and what has been previously derived from qualitative enquiry, our results and conclusion are transferrable from LBP into the general context of non-specific musculoskeletal disorder recovery discourse (22).
Our respondents had been exposed to systematic observation for a year by means of weekly SMS tracking and therefore might have developed “learnt” behaviours with respect to viewing their LBP. In particular, they could have developed a tendency to be more vigilant with respect to their back problem.
In closing, our investigation confirms that pain is central to the resolution of recurrent LBP-associated disorders. However, “recovery” also involves redefinition and readjustment. These domains are not addressed adequately in standard outcomes focused on pain, disability and participation and, as such, inferences regarding patient recovery must be viewed with caution.
ACKNOWLEDGEMENTS
We would like to acknowledge Maria A. Hondras for her input as scientific adviser and contribution to the intellectual quality of this article.
Financial support. This study was supported by the IMK General Fund (Denmark). The funding source (IMK General Fund) played no role in the design, execution, or interpretation of the findings of this investigation.
Conflicts of interest. The authors declare that no conflicts of interest exist in relation to this investigation.
REFERENCES

