Naoichi Chino, MD, PhD1, Yoshihiro Muraoka, PhD1, Hiroki Ishihama, PhD, RPT1, Masaru Ide, RPT1, Riousuke Ushijima, BS1 and Jeffrey R. Basford, MD, PhD2
From the 1The Eisei-kai Rehabilitation Research and Development Center, Kunugida-machi, Hachioji City, Tokyo, Japan and 2Department of Physical Medicine and Rehabilitation, Mayo Clinic, Rochester, MN, USA
Objective: To assess the ability of a newly developed portable instrument (the Electric Spastic Ankle Measure (E-SAM)) to quantitatively measure ankle plantar flexor muscle tone and spasticity.
DESIGN: Comparison of quantitative measurements of the E-SAM with those obtained manually with the Modified Ashworth Scale (MAS).
PARTICIPANTS: Seven adult men with stroke of more than 8 months’ duration with a MAS score of 3, and 7 healthy age-matched control subjects.
Main outcome measures: Quantitative measurements of the reactive and viscoelastic components of muscle tonus and spasticity.
RESULTS: Analysis of the pooled data of all subjects revealed 2 components: an initial negative peak (indicating viscoelasticity), and subsequent positive peaks (denoting reactive contractions of the plantar flexor muscles). Positive, reactive contraction, peaks of the subjects with stroke were significantly higher than those of age-matched controls (p<0.01, t-test).
CONCLUSION: The E-SAM appears to provide meaningful information on muscle tone and spasticity that is more specific and quantitative than that obtained with the MAS. While further study is necessary, this instrument shows promise as an easy-to-use clinical and research tool for the measurement of spasticity and muscle viscosity.
Key words: Modified Ashworth Scale; muscle tone; measurement; spasticity.
J Rehabil Med 2015; 47: 753–755
Correspondence address: Naoichi Chino, The Eisei-kai Rehab Research and Development Center, Kunugida-machi 583-15, Hachioji City, Tokyo #193-0942, Japan. E-mail: naochino@mbg.nifty.com
Accepted May 12, 2015; Epub ahead of print Aug 14, 2015

*This material was presented at the 75th American Academy of Physical Medicine and Rehabilitation (AAPMR) Annual Assembly, Poster 297 (Best Neurological Rehabilitation Research), Vol. 5, Issue 9, Suppl. S139, September 2013, http://www.pmrjournal.org/article/S1934-1482(13)00426-7/fulltext.
INTRODUCTION
Spasticity is a frequent consequence of upper motor neurone injuries, such as those associated with stroke and spinal cord injury (SCI). While its characterization as “a velocity-dependent increase in tonic stretch reflexes with exaggerated tendon jerks” (1) is widely accepted, its quantitative measurement and the specification of its components have remained elusive. This is not a trivial concern, as spasticity can have both inhibitory (such as slowing rehabilitation of the upper limb rehabilitation following stroke) or beneficial (e.g. improving the ability to stand following SCI) consequences. Easily obtainable, quantitative measurements might lead to more proactive control, treatment, and understanding of the impact of spasticity.
Clinical measurements of spasticity are currently limited to the use of manual tools such as the Ashworth or Modified Ashworth Scales (MAS). These scales have the advantages of wide use and easy application, but are limited in their reliability and ability to quantify results (2, 3). This lack has been well recognized, and while a number of attempts have been made to quantitate its measurement, the resulting instruments have typically proven bulky and difficult to use in the clinical setting (4, 5).
We describe here the use, and assess the capabilities of, a newly developed and easily portable instrument, the Electric Spastic Ankle Measure (E-SAM), to quantitate and isolate the spastic and viscoelastic components of muscle tone.
METHODS
The E-SAM consists of an ankle-foot orthosis (AFO) with torque sensors mounted on an upright bar, a goniometer at the ankle joint, and a foot plate that pivots about an anteriorly located hinge (Fig. 1a, b). When the heel lock is released, the lower extremity, as a result of its weight, drops from an initial position of 10° of ankle plantarflexion (Fig. 1b) to 5° of dorsiflexion (Fig. 1c). The foot plate is automatically locked in this latter position. Torque and angle data are recorded during the manoeuvre at a sampling frequency of 1 kHz using LabVIEW (LabVIEW 2011 National Instruments Corporation, Austin, TX, USA) software. The resulting data are then used to evaluate muscle tone and spasticity.
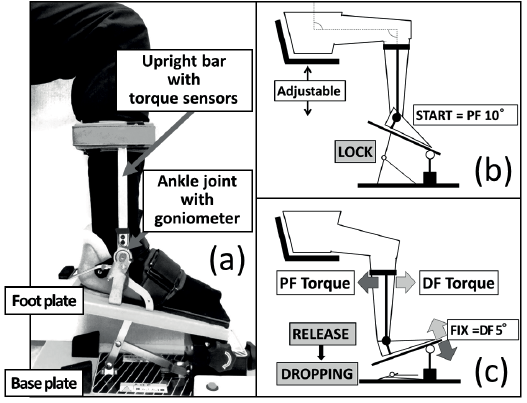
Fig. 1. Electric Spastic Ankle Measure (E-SAM) device and measurement protocol. Preparation phase: the subject sits with the ankle at 10° of plantarflexion (a). Measurement phase: the ankle is allowed to drop following the release of the lock bar (b) and then locked at 5° of dorsiflexion at completion of the drop (c). The torque sensor mounted on the upright bar measures the time series of the ankle torque. PF: plantar flexion, DF: dorsiflexion, FIX: fixation.
A pragmatic scale of spasticity, the E-SAM Score, was generated by applying a numerical formula to quantify the spasticity as follows:
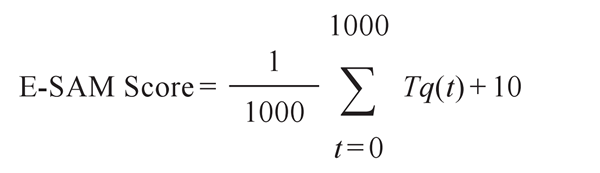
where the E-SAM score represents the value of the mean torque (Tq) during the period of 1000 ms following the start of the heel drop and the initiation of a dorsiflexion-generated stretch reflex. A value of 10 is added for convenience in communication so that the mean value in neurologically intact adults is positive but close to zero. Measurements are triggered by a switch in the E-SAM and automatically stored by a notebook computer that is connected to the device via a USB port.
The present study was approved by the ethics committee of the Eisei Hospital Health Care Group. All subjects signed informed consent and the study was conducted in accordance with the 1975 Declaration of Helsinki (revised 2008).
Subjects
Seven adult men (mean age 60.7 years (standard deviation (SD) 8.1); age range 47–69 years) with stroke of a mean duration of 89 months (range 8–292 months) and a MAS score of 3 were enrolled in the study. Seven (7) neurologically intact age-matched adult males (mean age 54.7 years (SD 7.8); age range 49–72 years) served as healthy controls. All subjects with stroke were recruited at the Eisei Clinic. Control subjects were recruited from the staff of the same institution. All measurements were performed at the Eisei Clinic between November 2011 and July 2012. Subjects’ MAS scores were assessed within 1 h of their E-SAM measurements.
Spasticity assessment
Subjects were seated on an adjustable-height chair with their hip and knee joints at 90° and their ankles fixed at 10° of plantarflexion by the E-SAM device (Fig. 1b, c). Measurements began when the lock bar was released without warning. Torque changes were recorded as indicated above.
All measurements were performed by the same physical therapist. The total duration of the measurement period was approximately 10 min, including setting up the device and positioning the subject. Measurements were repeated 10 times and averaged, with each waveform synchronized at the point where angle changes generated by the heel-lock release began.
RESULTS
Torque data obtained from the subjects with stroke had the appearance of a damped sine wave with 2 components: an initial negative peak, indicating viscoelastic resistance associated with eccentric stretching, and subsequent positive peaks denoting spastic (reflexive) components of the plantar flexor muscles (Fig. 2a). The absolute value of the viscoelastic negative peak was lower (mean ± standard error (SE) –11.5 ± 7.1 Nm, range –21.4 to 0.1 Nm) among the subjects with stroke than among their healthy control counterparts (mean ± SE –33.0 ± 5.1 Nm, range –41.3 to –25.2 Nm), while the subsequent positive values were higher among the members of the stoke group (mean ± SE 5.6 ± 2.1 Nm, range 2.8–8.4 vs mean ± SE –3.7 ± 1.1 Nm, range –4.8 to –1.5 Nm, respectively). Ankle jerk reflexes were elicited in all trials and measurements successfully obtained in all subjects. There were no adverse effects. Ankle joint trajectories of the stroke and the control subjects are displayed in Fig. 2b.
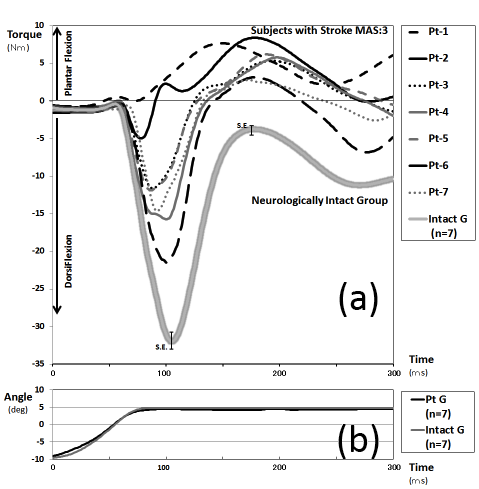
Fig. 2. Ankle torque and trajectories recorded using the Electric Spastic Ankle Measure (E-SAM) device. The individual torque curves for 7 subjects with (Pt) (Pt-1 to Pt-7) and the composite curve for their 7 control counterparts. Mean ankle joint torque (a) and angle (b) trajectories of the subjects with stroke and the control subjects measured by the E-SAM device.
The mean ± SE of E-SAM score in the normal subjects was low (0.21 ± 0.54), whereas those of the subjects with spasticity was significantly higher (10.10 ± 0.98) (p < 0.01, t-test, SPSS 17.0).
DISCUSSION
This paper represents the first report and assessment of the capabilities of E-SAM, a newly developed and clinically feasible tool for the measurement of muscle tone and spasticity. The initial results are encouraging. The device was able to delineate statistically significant differences between the time-averaged composite scores (10.1 vs 21, p < 0.01) of the subjects with stroke and their control counterparts. Furthermore, and, unlike the situation with the MAS, the E-SAM was able to quantitate and isolate the viscoelastic and spastic/reflexive components of a subject’s response. While neither E-SAM nor the MAS are likely to result in adverse effects, the MAS requires far more skill and training to grade accurately (6) than the simple triggering of the heel drop required by the E-SAM.
Clinical measurements using the MAS are subjective, but, given the lack of a convenient quantitative alternative, serve as the global standard for evaluating spasticity (7). A number of quantitative measures of spasticity have been proposed previously, with approaches involving both handheld and fixed instruments and ranging in complexity from measuring the pendulum component of the knee-jerk motion (8) to increasingly sophisticated computer-based analyses of ankle (4, 5) and elbow motion (9). However, most of these tools are expensive; their measurements time-consuming, and their use experimental. The findings of this study suggest that, while more research is needed, the E-SAM may be a practical tool for use in both the research and clinical assessment of spasticity.
Limitations
The findings of this study are reassuring in that they indicate that the E-SAM can both detect and quantitate differences in muscle tone and spasticity in people with or without upper motor neurone injury. However, our report deals with an initial evaluation and, as such, has a number of limitations that future work will need to address. First, we assessed only adult male subjects with stroke and a MAS of 3. Generalization would require the assessment of a broader range of conditions and severities of spasticity. Secondly, the ability of this device to isolate and measure the viscoelastic and reflexive component of muscles to a heel-drop stimulus is encouraging, but this work also needs further expansion to assess the reliability and reproducibility of the measurements. Thirdly, we did not examine subjects with noticeable contractures, and it is likely that our approach, as is the case with the MAS, would be less useful in this group. Further studies are required to evaluate the potential roles of sex, age, size, and, spasticity, as well as (despite the device’s nearly complete operator independence) its intra- and inter-rater reliability.
Conclusion
While further research is needed, these results suggest that the E-SAM device can detect and quantitate differences in muscle tone and spasticity in people with or without upper motor neurone injury in a manner that is potentially practical in the clinical setting.
Acknowledgements
Chino N, Muraoka Y and Ishihama H hold a patent on E-SAM. It has been assigned to Tomei Brace Co. (Nagoya City, Japan). The other authors have no conflicts of interest.
REFERENCES

