Lucelle A. W. van de Ven-Stevens, MSc, OT, CHT-NL1, Maud J. L. Graff, PhD, OT2, Ruud W. Selles, PhD3, Ton A. R. Schreuders, PT, PhD, CHT-NL3, Harmen van der Linde, PhD, MD1, Paul H. Spauwen, MD, PhD4 and Alexander C. H. Geurts, PhD, MD2
From the 1Department of Rehabilitation, 2Donders Institute for Neuroscience, Department of Rehabilitation, Radboud University Medical Centre, Nijmegen, 3Department of Rehabilitation and Department of Plastic and Reconstructive Surgery, Erasmus University Medical Center, Rotterdam, 4Department of Plastic and Reconstructive Surgery, Radboud University Medical Centre, Nijmegen, The Netherlands and Wilhelminenspital, Vienna, Austria
OBJECTIVE: To reach multidisciplinary European consensus on the assessment tools for impairments and activity limitations in patients with hand conditions.
DESIGN: Electronic Delphi method.
SUBJECTS: Thirty experts from European societies for hand therapy, hand surgery, and physical and rehabilitation medicine.
METHODS: In 3 rounds, participants were asked which of 13 preselected categories of the Brief International Classification of Functioning, Disability and Health (ICF) Core Set for Hand Conditions should be assessed. In addition, they were asked to choose which of 55 preselected instruments they preferred for each category by confirming or rejecting instrument-specific statements.
RESULTS: All 13 preselected ICF categories were considered relevant. Consensus was based on ≥ 75% agreement. After 3 rounds, 9 instruments were selected: Shape Texture Identification Test, Semmes Weinstein Monofilament Test, Visual Analogue Scale for pain, goniometer, Jamar Dynamometer, Pinch Gauge Device, Cold Intolerance Symptom Severity questionnaire, Canadian Occupational Performance Measure, and Disabilities of the Arm, Shoulder and Hand Questionnaire. It remained undecided whether to use the Nine-Hole Pegboard Test or the Purdue Pegboard Test.
CONCLUSION: In this European Delphi study, multidisciplinary consensus was reached on 9 assessment tools for impairments and activity limitations in patients with hand conditions addressing 13 categories of the Brief ICF Core Set for Hand Conditions.
Key words: Delphi study; outcome assessment; hand conditions; hand injuries; hand therapy; ICF.
J Rehabil Med 2015; 00: 00–00
Correspondence address: Lucelle A. W. van de Ven-Stevens, Radboud University Medical Centre, Radboud Institute for Health Sciences, Department of Rehabilitation, 898, PO Box 9101, NL-6500 HB Nijmegen, The Netherlands. E-mail: L.vandeVen-Stevens@home.nl/Lucelle.vandeVen-Stevens@Radboudumc.nl
Accepted Jul 31, 2015; Epub ahead of print Oct 9, 2015
INTRODUCTION
Injuries of the hand are among the most common injuries worldwide (1), accounting for approximately 20% of all visits to hospital emergency departments (2). Both hand injuries and hand diseases (i.e. hand conditions) may affect a person’s ability to engage successfully in day-to-day self-care, work and leisure activities (1, 3) and therefore may have a serious impact on social participation and health-related quality of life (4, 5).
The use of valid, reliable and responsive instruments to assess the impact of hand conditions on functioning and quality of life is essential for clinical decision-making, monitoring patient progress and evaluating the effectiveness of treatment (6–8). Although hand impairments can cause activity limitations, this relationship is rather complex (9–11). It is, thus, important to assess not only body functions (impairments), but also a person’s (limitations to perform) activities in order to determine how different hand conditions impact the daily lives of individual patients (6, 8, 12–19).
In recent decades, professionals in the field of hand surgery and hand rehabilitation have emphasized the need for consensus in defining a core group of assessment instruments to facilitate a universal description and comparison of individual hand impairments and related disabilities (6, 7, 20, 21). This, however, requires consensus on which of the available validated instruments, that are also reliable and responsive, should be used to assess (and preferably predict) a patient’s functioning and/or to evaluate outcomes of different interventions. Many tools are available to assess impairments and activity limitations in patients with hand conditions, but there is currently no standardized accepted core set for use with this patient group (6, 12, 14, 18, 20). To support the development of such a core set, we first conducted 2 systematic reviews in order to identify 23 instruments that can be used to evaluate activity limitations in patients with hand conditions (18, 19). In a previous study, the content of published studies on hand conditions was analysed (22) for the development of the Brief and Comprehensive International Classification of Functioning, Disability and Health Core Set for Hand Conditions (BICF-CS) (23). The BICF-CS is a subset derived from the International Classification of Functioning, Disability and Health (ICF) (24), consisting of 23 ICF categories (22, 25). Based on knowledge about available instruments and their relationship with relevant ICF categories, we conducted an international Delphi study (the HandART-Delphi study). The aim was to reach multidisciplinary European consensus on a core set of assessment tools to be used in patients with hand conditions who may need surgical or non-surgical interventions. The focus was to include as few instruments as possible, but as many as necessary to assess impairments and activity limitations, addressing all categories of the BICF-CS (25).
METHODS
Participants
Experts from the European Federations of Societies for Hand Therapy (EFSHT), Hand Surgery (FESSH), and Physical and Rehabilitation Medicine (ESPRM) were invited to participate. To this end, a written invitation was sent to these European societies, and subsequently to their individual members, by the national societies. To participate in the HandART-Delphi study, experts had to have ample clinical experience of treatment of hand injuries and/or hand diseases during the last 5 years and have sufficient knowledge of the English language. Participants were selected based on fulfilment of at least 1 of the following criteria, in the field of hand surgery or hand therapy: (i) being involved in research on the use of assessment tools; (ii) being a (co-) author of one or more published articles about assessment tools; (iii) being a lecturer on clinimetrics; or (iv) being involved in developing an assessment protocol or standardized assessment. Participants had to indicate their expertise on a separate form that was sent together with the written invitation. In advance, it was decided to invite a maximum of 32 experts, including, physical therapists (PTs), occupational therapists (OTs), hand surgeons, and rehabilitation physicians. This number of participants was considered appropriate in order that all disciplines were well represented. The preferred ratio between disciplines was set beforehand at 16 hand therapists (PTs and OTs), 8 hand surgeons, and 8 rehabilitation physicians.
Instruments
Assessment tools considered in this study were instruments that: (i) are used to measure impairments and activity limitations in patients with hand conditions; (ii) are used in adults; (iii) can be used in the acute phase or post-acute phase of rehabilitation; and (iv) are used in addition to general physical examination (Table I). We excluded instruments concerning quality of life, instruments concerning personal and environmental factors, diagnostic tests (i.e. medical or laboratory tests, such as X-ray or electromyography), and instruments that were specifically developed for children.
|
Table I. Assessment tools that were linked to the components “Body functions” and “Activity and Participation” of the Brief International Classification of Functioning, Disability and Health Core Set for Hand Conditions (BICF-CS) |
|
Assessment tools |
|
Instruments mainly measuring body functions and structures |
|
Ab-adductometer |
|
AIKOH dynamometer gauge |
|
Blood-pressure cuff |
|
Goniometer |
|
Grated Orientation Task |
|
Grippit |
|
Hot & Cold Discriminator Test |
|
Intrinsic-o-meter (Mannerfelt) |
|
Jamar Dynamometer |
|
Locognosia Test |
|
Lode handgrip dynamometer |
|
Lode pinch-grip dynamometer |
|
Moberg Pick Up Test (MPT) |
|
Numeric rating scale |
|
Pinch Gauge Device |
|
Pollexograph |
|
Rotterdam Intrinsic Hand Myometer (RIHM) |
|
Semmes Weinstein Monofilament Test (SWMT) |
|
Shape Texture Identification Test (STI) |
|
Tuning fork |
|
Two-Point Discrimination Test – Static (STPD) |
|
Two-Point Discrimination Test – Moving (MTPD) |
|
Verbal rating scale |
|
Vibrometer |
|
Vigori-meter |
|
Visual analogue scale (pain) (VAS) |
|
Wire tracing method |
|
Pegboard tests |
|
Functional dexterity test (FDT) |
|
Grooved Pegboard Test |
|
Nine-Hole Peg Test (NHPT) |
|
Purdue Pegboard Test (PPT) |
|
Instruments measuring fine hand use by handling different objects |
|
Box and block test (BBT) |
|
Minnesota Manual Dexterity Test (MMDT) |
|
Moberg Pick Up Test (MPT) |
|
O’Neill Hand Function Assessment |
|
Rosenbusch Test of Finger Dexterity |
|
Instruments measuring single tasks (and fine hand use) by scoring tasks |
|
Arthritis Hand Function Test (AHFT) |
|
Jebsen-Taylor Hand Function Test (JTHFT) |
|
Radboud Skills Test (RST) |
|
Sequential Occupational Dexterity Assessment (SODA) |
|
Smith Hand Function Evaluation (SHFE) |
|
Sollerman Hand Function Test (SHFT) |
|
Southampton Hand Assessment Procedure (SHAP) |
|
Upper Extremity Performance Test Elderly ( TEMPA) |
|
Upper Extremity Function Test (UEFT) |
|
Questionnaires |
|
Australian/Canadian Osteoarthritis Hand Index (AUSCAN) |
|
Canadian Occupational Performance Measure (COPM) |
|
Cold Intolerance Symptom Severity Questionnaire (CISS) |
|
Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) |
|
Michigan Hand Outcomes Questionnaire (MHQ) |
|
McGill Pain Questionnaire–long form (MPQ) |
|
McGill Pain Questionnaire–short form (MPQ) |
|
Patient Evaluation Measure (PEM) |
|
Patient Rated Wrist and Hand Evaluation (PRWHE) |
|
Subjective Hand Function Scoring System (HFS) |
|
Upper Extremity Functional Scale (UEFS) |
Design
A web-based electronic Delphi method was used. To make effective decisions in situations in which there is contradictory or insufficient information, the Delphi Survey Technique for reaching consensus is recommended (20, 26–28). This procedure includes a series of sequential questionnaires (“rounds”) that must be completed by a group of multidisciplinary experts (20, 26–28). An electronic Delphi method was considered most appropriate because of its feasibility in the case of an international study (28).
The formal consensus method consisted of 3 rounds, conducted via the internet supported by an IT company (www.horn.nl). Anonymity of responses was ensured in order to prevent opinion leaders influencing the individual opinions of other experts. Feedback of expressed expert input was provided after the first and second rounds, leading to a cyclical procedure to enable each participant to reconsider his/her earlier opinion or to provide arguments in favour of one’s opinion (28). The identity of the experts was known only to the principal investigator (LvdV).
Procedure
Three Delphi rounds were conducted. In each round all participants received an invitation e-mail providing background information. They were requested to login to a secure HandART-Delphi website to access the pages with questions and statements. If participants did not respond to the first invitation within 2 weeks, or if they left some of the questions unanswered, they were sent a reminder e-mail. They were asked to use both the best-available evidence and their clinical experience to make their decisions. Questions and statements were developed based on the results of previous studies (18, 19, 22, 25) using the ICF structure as a framework (24).
Each round consisted of formulating questionnaires and statements, sending these questionnaires to the participants, performing an analysis on the data received, and writing a feedback report. All tasks were carried out by the principal investigator (LvdV) with feedback from the research group (AG, MG, RS, TS, PS and HL). Although there is no universally accepted percentage of agreement for reaching consensus, the literature recommends 70–80% agreement to be set prior to data analysis (28). In the present study, a ≥ 75% agreement level was used to define consensus on a particular item (27, 28).
First round
First, 13 of the 23 ICF categories of the BICF-CS, referring to the levels of “body functions” and “activities and participation”, were selected (Table II). Two categories (i.e. “touch function” and “sensory functions related to temperature and other stimuli”) were combined because of the overlay of constructs and associated instruments, resulting in 12 categories. Each category was presented with a variable number of assessment tools that had been linked to this specific category based on previous work (29).
For each category 2 questions had to be answered by the experts:
• Is it important to assess this category? (yes/no/do not know).
• Are there any instruments missing that are commonly used and can be linked to this category? (yes, namely…./no/do not know).
For each instrument within each category 2 more questions had to be answered:
• Do you use this instrument to assess this category? (yes/no).
• Should this instrument be part of a core set to represent this category? (not at all/perhaps/certainly/do not know).
Participants were invited to provide argumentation and add literature in support of their answers.
If, for a specific assessment tool, 75% or more of the respondents had answered “certainly” on the last question, the instrument was selected and included in the HandART core set of instruments. The other results were used to define questions for the second round.
|
Table II. Selected categories of the Brief International Classification of Functioning, Disability and Health (ICF) Core Set for Hand Conditions (BICF-CS), concerning the components “Body functions” and “Activity and Participation” |
|
|
ICF code |
Description |
|
b265 & b270 |
Touch function & Sensory functions related to temperature and other stimuli Including: stereognosis, tactile gnosis, temperature recognition, detection threshold, and spatial discrimination |
|
b280 |
Sensation of pain |
|
b710 |
Mobility of joint functions |
|
b730 |
Muscle power functions |
|
d230 |
Carrying out daily routine |
|
d430 |
Lifting and carrying objects |
|
d440 |
Fine hand use |
|
d445 |
Hand and arm use |
|
d5 |
Self-care |
|
d6 |
Domestic life |
|
d7 |
Interpersonal interactions and relationships |
|
d840–d859 |
Work and employment |
Second round
The statements used in the second round were formulated according to decision rules explained in Table III. If in the first round the percentage of respondents who answered “certainly” and “perhaps” was 75% or higher, and the % “certainly” was higher than the % “perhaps”, a new statement suggested selecting this instrument for assessing the specific ICF category of the core set (agree/disagree), taking into account the group opinions and comments given by others in the first round. For the missing instruments mentioned in the first round, participants had to indicate whether this instrument should be part of the core set to assess a specific category (not at all/perhaps/certainly/do not know).
|
Table III. Decision rules, based on the results of the first Delphi round, which were used to define second-round statements for each assessment tool |
||
|
Result first round |
Statement second round |
|
|
A. |
75% or more of respondents had answered “certainly” |
The instrument was included in the core set of instruments No new statement was formulated |
|
B. |
The sum of the % respondents who answered “certainly” and “perhaps” ≥ 75% and the % “certainly”>% “perhaps” |
A new statement suggested to use this instrument to assess a selected ICF category (agree/disagree) |
|
C. |
An instrument was already included based on ≥75% absolute agreement (A) and a second instrument linked to the same ICF category fulfilled the criterion mentioned under B |
It was asked whether the second instrument should be added to assess the same ICF category (yes/no) |
|
D. |
The sum of the % respondents who answered “certainly” and “perhaps”< 75% or the %”certainly”<%”perhaps” |
A new statement suggested not to include this instrument (agree/disagree) |
|
E. |
According to 1 or more participants, a missing instrument should “certainly” be included in the core set and could be linked to a selected ICF category |
It was asked whether this instrument should be used to assess this ICF category (not at all/perhaps/certainly/do not know) |
|
F. |
An instrument was mentioned by one or more respondents as missing, but could not be linked to a selected ICF category |
This instrument was not proposed to be included No new statement was formulated |
|
ICF: International Classification of Functioning, Disability and Health. |
||
If 75% or more of the respondents agreed with the suggestion upon the use (or no use) of an instrument to assess this preselected ICF category, the instrument was definitively selected (or rejected).
Third round
In the final round a new set of statements was formulated based on the results of the first and second rounds; however, only for those categories and instruments for which consensus had not yet been reached. Participants had to indicate whether they (dis)agreed with each statement, taking into account the group opinions and comments from the first and second rounds as well as the results of the clinimetric review (18).
Finally, participants were asked an open-ended question about their general opinion of the HandART-Delphi study.
RESULTS
Consensus
A total of 30 experts responded to the invitation and participated in the study (Table IV). The group consisted of 10 OTs/hand therapists, 9 PTs/hand therapists, 6 hand surgeons, and 3 rehabilitation physicians. Two hand therapists were also both PTs and OTs. Because the FESSH had sent the invitation to its members after the first Delphi round, the hand surgeons participated only in the second and third rounds. As a result, 7 European countries were represented in the first round, and 9 in the second and third rounds (see Fig. 1). The response rate varied from 90% to 93%.
|
Table IV. PARTICIPANTS: numbers and response rates |
|||||||||||||||
|
HandART Delphi |
Primary discipline |
Additional occupation |
Years of experience, mean |
Statement/questions, n |
Response rate, % |
||||||||||
|
Total, n |
OT/HT, n |
PT/HT, n |
Both OT/HT and PT/HT, n |
Hand surgeon, n |
Physiatrist, n |
Researcher, n |
(Co-)author, n |
Lecturer n |
Developer, n |
Other, n |
|||||
|
Round 1 |
22 |
9 |
9 |
2 |
– |
2 |
16 |
15 |
17 |
12 |
5 |
19.6 |
306 |
93 |
|
|
Round 2 |
30 |
10 |
9 |
2 |
6 |
3 |
21 |
21 |
22 |
13 |
5 |
17.0 |
141 |
90 |
|
|
Round 3 |
29 |
10 |
9 |
2 |
5 |
3 |
20 |
20 |
22 |
13 |
5 |
17.1 |
54 |
90 |
|
|
OT: occupational therapist; PT: physical therapist; HT: hand therapist. |
|||||||||||||||
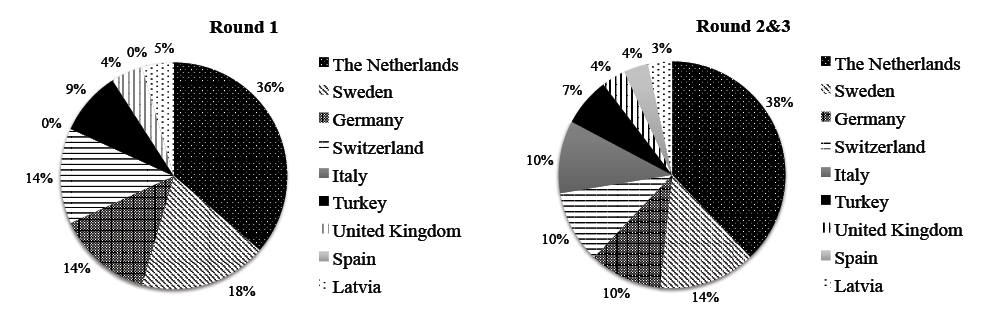
Fig. 1. Represented countries.
In the first round, more than 75% of the participants indicated that it was important to assess each of the selected ICF categories. Eight instruments, assessing 7 categories, were preliminarily included in the HandART core set (Table V). A total of 42 different instruments were reported as missing (Table VI), and respondents indicated 19 times that the missing instrument should “certainly” be included in the core set.
In the second round, consensus was reached for 6 ICF categories on which instruments to select and which not to select. Of the 19 instruments that were reported as missing in the first round and that were suggested for inclusion in the core set, no instrument reached the necessary level of ≥ 75% agreement (certainly and perhaps) to formulate new statements for inclusion.
In the third and final rounds, consensus was reached on 9 instruments for the assessment of 9 ICF categories of the core set (Table V): the Shape Texture Identification test (STI), the Semmes Weinstein Monofilament Test (SWMT) and the Cold Intolerance Symptom Severity questionnaire (CISS) to assess “Touch function” and “Sensory functions related to temperature and other stimuli” (ICF b265 & b270); the Visual Analogue Scale for pain (VAS) to assess “Sensation of pain” (ICF b280); the Goniometer to assess “Mobility of joint functions” (ICF b710); the Jamar Dynamometer and the Pinch Gauge Device to assess “Muscle power functions” (ICF b730); the Canadian Occupational Performance Measure (COPM) and the Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) to assess other ICF categories (d230, d430, d445, d6, d840–d859).
For 39 other instruments (Table I), consensus was reached to exclude these from the core set.
|
Table V. Selected instruments related to the preselected International Classification of Functioning, Disability and Health (ICF) categories |
|||||||||||||
|
ICF codes |
b265& b270 |
b280 |
b710 |
b730 |
d230 |
d430 |
d440 |
d445 |
d5 |
d6 |
d7 |
d840– d859 |
|
|
Should this category be assessed? (yes/no (%)) |
Yes1 (91%) |
Yes1 (100%) |
Yes1 (100%) |
Yes1 (100%) |
Yes1 (81%) |
Yes1 (90%) |
Yes1 (100%) |
Yes1 (100%) |
Yes1 (95%) |
Yes1 (100%) |
Yes1 (80%) |
Yes1 (90%) |
|
|
Instruments measuring body functions |
|||||||||||||
|
Shape Texture Identification test (STI) |
Δ2 |
||||||||||||
|
Semmes Weinstein Monofilament Test (SWMT) |
Δ2 |
||||||||||||
|
Static Two-Point Discriminator (STPD) |
50% |
||||||||||||
|
Locognosia Test |
36% yes |
||||||||||||
|
Visual analogue scale (VAS) |
Δ2 |
||||||||||||
|
Goniometer |
Δ2 |
||||||||||||
|
Jamar Dynamometer |
Δ2 |
||||||||||||
|
Pinch Gauge Device |
Δ2 |
||||||||||||
|
Pegboard tests |
|||||||||||||
|
Nine-Hole Pegboard Test |
37% yes |
||||||||||||
|
Purdue Pegboard Test |
59% yes |
||||||||||||
|
Instruments measuring only fine hand use by picking up, manipulating and placing different objects |
|||||||||||||
|
None |
|||||||||||||
|
Instruments measuring single tasks (and fine hand use) by scoring executed tasks |
|||||||||||||
|
Jebsen-Taylor Hand Function Test (JTHFT) |
× |
× |
31% yes |
× |
|||||||||
|
Sollerman Hand Function Test (SHFT) |
× |
× |
69% yes |
× |
|||||||||
|
Questionnaires |
|||||||||||||
|
Cold Intolerance Symptom Severity Questionnaire (CISS) |
Δ |
× |
× |
× |
× |
× |
× |
||||||
|
Canadian Occupational Performance Measure (COPM) |
? 4% yes |
Δ2 |
? 23% yes |
Δ |
|||||||||
|
Disabilities of the Arm, Shoulder and Hand questionnaire (DASH) |
× |
× |
× |
× |
Δ |
Δ |
× |
Δ2 |
? 46% yes |
Δ |
? 46% yes |
Δ2 |
|
|
Both COPM and DASH |
50% |
31% |
|||||||||||
|
Patient Rated Wrist and Hand Evaluation (PRWHE) |
× |
× |
× |
? 73% no |
× |
× |
× |
||||||
|
1Confirmed to be important based on ≥ 75% agreement in the first round. 2Selected based on ≥ 75% agreement in the first round. ΔSelected based on ≥ 75% agreement after 3 rounds. ×: Not selected based on > 75% agreement, but linked to this ICF category. ?: No agreement. |
|||||||||||||
|
Table VI. Non-selected instruments, mentioned as missing in the first round for each International Classification of Functioning, Disability and Health (ICF) category |
|
|
ICF category |
Instrument (number of times mentioned) 19 instrument that should “certainly” be included in the core set, according to 1 or more participants, are given in italic |
|
b265 & b270 |
Detection threshold: Mapping Localization Test Ninhydrin Test (2×) Sollerman Test The Ten Test (2×) The Ten Test Revisited Wrinkle Test (mentioned 3×) |
|
b280 |
body-pain-chart LANSS pain scale (Leeds Assessment of Neuropathic Symptoms and Signs) Pain Self-Efficacy Questionnaire (PSEQ) Schultz UE Pain Assessment (SUEPA) |
|
b710 |
(Slide) Caliper for ROM CMCI Inclinometer Pro- Supination Kapandji thumb range of motion (2×) Kapandji: functional hand grasps PRWHE Tip-To-Palm/centimeter (2×) |
|
b730 |
dyNex1 grip dynamometer Manual muscle testing, scored using the MRC scale (0–5) MIE Myometer Worksimulator (BTE, Baltimore Technical equipment) |
|
d230 |
Canadian Occupational Performance Measure (COPM) (2×) EQ-5D (EuroQol) The European Research Questionnaire Quality of Life), general questions Medical Outcomes Study, Short Form 12 (MO-SF12) and SF-36 MHQ Milliken Activities of Daily Living Scale PRWHE (2×) PSFS – Patient Specific Functional Scale Quick DASH |
|
d430 |
COPM (2×) Patient Specific Functional Scale (PSFS) Valpar work samples WEST Standard Evaluation Procedure (2×) Worksimulator (BTE) |
|
d440 |
Cambridge Hand Function test Crawford Small Parts Dexterity Test Functional Capacity Evaluation O’Conner Dexterity test |
|
d445 |
Abilhand Alderson-McGall Hand Function Questionnaire COPM Valpar work sample Worksimulator (BTE) |
|
d5 |
Milliken Activities of Daily Living Scale Patient Specific Functional Scale (PSFS) Patient Specifieke Klachten (PSK) (Dutch) Short Form-36 (SF-36) |
|
d6 |
SF-36 Impact on Participation and Autonomy (IPA) Jebsen-Taylor Hand Function Test (JTHFT) Milliken Activities of Daily Living Scale (MAS) Patient Specific Functional Scale (PSFS) |
|
d7 |
Impact on Participation and Autonomy questionnaire (IPA) (2x) MOHO Kielhofner& Henry 1988 Patient Specific Functional Scale (PSFS) SF-36 (2×) |
|
d840 –d859 |
Beck depression inventory, Beck anxiety inventory Evaluation der Funktionellen Leistungsfähigkeit (EFL) (German) Impact on Participation and Autonomy (IPA) Potential Work Exposure Scale (PWES) (McCabe, 1991) (2×) Patient Specific Functional Scale (PSFS) Valpar Work Samples |
No consensus
In the categories “Touch function” and “Sensory functions related to temperature and other stimuli” (ICF b265 & b270), no consensus was reached with regard to the Locognosia Test and the Static Two-Point Discriminator (STPD).
In the category “Fine hand use” (ICF d440), for both the Nine-Hole Peg Test (NHPT) and the Purdue Pegboard Test it was suggested in the second round to use these instruments (see Table III). Thirty percent of the respondents favoured the NHPT over the PPT, 22% favoured the PPT over the NHPT, whereas 48% indicated that both instruments should be selected. In the final round, when participants were forced to choose between these 2 instruments, 37% selected the NHPT and 59% the PPT.
In the category “Hand and arm use” (d445), the DASH was included. For both the Jebsen-Taylor Hand Function Test (JTHFT) and the Sollerman Hand Function Test (SHFT) it was suggested in the second round to use these instruments to assess “hand and arm use” (see Table III). Twenty-two percent of the participants chose the JTHFT, 37% the SHFT, 22% both tests, and 19% neither of these tests. In the final round, when participants had to choose between these 2 instruments, 31% selected the JTHT and 69% the SHFT (Table V).
Collected comments and arguments regarding the undecided instruments obtained in the 3 rounds together are presented in Table VII.
|
Table VII. Comments collected during 3 rounds regarding instruments for which no consensus was reached |
||
|
Instrument |
Yes, should be selected Comments and arguments |
No, should not be selected Comments and arguments |
|
Static Two-Point Discriminator (STPD) |
Quick assessment (2×) Quantitative Measure of density receptors Reliable (2×) For evaluation in research |
Limited reliability (5×) and validity; Pressure not manageable: the amount of pressure applied can vary with each application (2×) Not clear if patient can discriminate between 2 points or if he feels a line Validity for spatial threshold questionable Long administration time STI already selected Only useful for quick clinical detection Not suitable for research Not suitable for follow-up Often unresponsive especially in complete nerve injuries (2×) Different protocols and instruments exist |
|
Locognosia Test |
Gives complex data Only when using published standardized protocol by Jerosch (37) Good for diagnostics (2×) Responsive (2×) In peripheral nerve injury as prognostic sign Correlation with tactile gnosis tests Reliable in median and ulnar nerve injury |
Very time-consuming (5×) Complicated to apply (3×) Little extra information (2×) Unknown (2×) Preference to use monofilaments Useful in nerve injury, only when sensory re-education is indicated, |
|
Nine-Hole Peg Test (NHPT) |
Faster than PPT |
The complexity of fine hand use inadequately captured by simple grasp and release tasks More focused on hand/arm and eye coordination than on manual dexterity |
|
Purdue Pegboard Test (PPT) |
Many options to look at fine hand use or dexterity Involves bilateral and unilateral hand use (4×) Broader age range of normative data (2×) Reliable (2×) |
The complexity of fine hand use inadequately captured by simple grasp and release tasks Time-consuming |
|
Jebsen-Taylor Hand Function Test (JTHFT) |
High degree of standardization Commercial availability |
Writing task is out-dated (writing with the non-dominant hand is odd) |
|
Sollerman Hand Function Test (SHFT) |
Many items linked to hand and arm use (2×) Also assesses quality of movement |
Not commercially available (3×) |
General opinion
Ten participants (35%) gave an opinion about the HandART-Delphi study. According to these respondents, the study had been well organized and information and feedback on each round was well provided. Sixteen other participants (55%) responded that they had no comments. Three participants (10%) did not respond to this question.
DISCUSSION
The aim of the HandART-Delphi study was to reach multidisciplinary European consensus on a core set of assessment tools for impairments and activity limitations in patients with hand conditions, addressing the 13 categories of “body functions” and “activities and participation” of the BICF-CS (25). After 3 Delphi rounds, a group of 30 international experts from 9 European countries, consisting of hand therapists, hand surgeons and rehabilitation physicians, reached consensus (based on at least 75% agreement) on the majority of the preselected instruments. In the second and third round, consensus was reached on 9 instruments for the assessment of 9 ICF categories of the core set (see Table V). For 39 other instruments, consensus was reached that these should not be selected.
Regarding the assessment of “body functions”, consensus was reached for the domains Pain, Mobility of joint functions (Active range of motion), and Muscle power functions (Grip strength and Pinch strength). The VAS, goniometer, Jamar Dynamometer and Pinch Gauge Device were selected to assess these ICF categories, which is consistent with common clinical practice as well as with the literature in which these instruments are frequently used and recommended (7, 13, 22, 30–35). In addition, the STI, SWMT, and CISS were included in the core set to assess Touch function & Sensory functions. Although there is evidence for the validity of the Swedish version of the CISS (36), information about the validity of the English language version is not available. No consensus was reached with regard to the Locognosia Test or the Static Two-Point Discriminator (STPD) to assess spatial discrimination. Several participants commented that the Locognosia Test is time-consuming and provides little extra information. Others were in favour of the Locognosia Test, emphasizing its reliability and responsiveness. Hence, in a diagnosis-specific core set, the Locognosia test might still be selected, but only if the test is administered according to a standardized protocol (37).
Regarding the assessment of “activities and participation”, consensus was reached on most of the preselected instruments assessing the ICF categories “fine hand use” and “hand and arm use” that these should not be included in the core set. The choice between 2 remaining assessment tools, the NHPT and the PPT, that had both been linked to the ICF category “fine hand use”, remained undecided due to personal preferences, although the value of each instrument was agreed upon. Considering that, preferably, only one pegboard test should be part of the core set, an argument in favour of the NHPT would be the relatively short administration time. On the other hand, the PPT might be favoured over the NHPT, because it involves bilateral and unilateral hand use, has a broader age range of normative data, and has good test-retest reliability (38).
In the category “hand and arm use”, the selection of the DASH was readily agreed upon. However, the DASH is a questionnaire that evaluates the experienced disabilities of the patient and is not an observational instrument to assess the execution of specific tasks. For this reason, the JTHFT and the SHFT were also considered, but neither of these instruments reached 75% agreement. Still, the participants indicated that at least 1 of these instruments should be included in the core set. The SHFT might be preferred for various reasons. It is not only based on the time needed to finish tasks, but also on the quality of the movement (17, 18). Furthermore, it received a better rating than the JTHF in recent studies (39, 40), and 8 of its items (compared with 4 items of the JTHF) can be linked to the d445 category (29). A disadvantage of the SHFT is, however, that it is not (yet) commercially available, as mentioned by several experts (Table VII).
Strengths and limitations of the study
This Delphi study showed a very high response rate in all 3 rounds. According to the participants, the electronic method was feasible and adequate to reach consensus on the various topics addressed. If necessary, participants received a reminder if they had not yet responded. None of the participants (post-hoc) expressed the necessity of real-life meetings to reach consensus on the issues raised.
The present study had several limitations. In advance, it was decided to invite a maximum of 32 experts to participate, preferably 16 hand therapists (PTs and OTs), 8 hand surgeons, and 8 rehabilitation physicians. In fact, only 30 professionals were available, in a different ratio. Considering that, in clinical practice, mostly hand therapists will use the selected assessment tools, we believe that the multi-disciplinarity of the included experts was fair, albeit that rehabilitation physicians were underrepresented. The external validity of the participants may be questioned because of an overrepresentation of Dutch experts. Under-representation of other countries occurred due to limitations of Internet accessibility, problems with the English language, and the lack of well-represented networks of professionals in some European countries. Another limitation is the absence of patients and insurers as participants.
A core set of instruments developed by a consensus procedure, such as a Delphi study, is developed through consideration of the opinions of experts and is influenced by current practice. Therefore, if new clinimetric data become available, a revision of this core set of instruments may be necessary. The HandART-Delphi study was restricted to the selection of assessment tools. Standardization or protocols for administration of tests were not the subject of this study. The update of the Clinical Assessment Recommendations of the American Society of Hand Therapists (13) can be used for such purposes. Furthermore, this study was focused on instruments to be used in a generic core set for patients with hand conditions. In addition to such a generic core set, several diagnosis-specific assessment tools are available. Thus, instruments such as the Patient Rated Wrist and Hand Evaluation (PRWHE) or the Carpal Tunnel Syndrome questionnaire (41), which were not selected in this Delphi study, might still be valuable for a diagnosis-specific evaluation.
Recommendations
Future research should aim to reach consensus on which assessment tools should be used to address the remaining categories of the BICF-CS, such as “emotional functions” and “environmental factors”. Moreover, future research should evaluate the clinical feasibility of this core set as well as the acceptance by professionals, patients and insurers. Furthermore, diagnosis-specific core sets may need to be developed in addition to this generic core set.
Conclusion
In this HandART-Delphi study, multidisciplinary European consensus was reached on assessment tools for impairments and activity limitations in patients with hand conditions, addressing 13 categories of the BICF-CS. After 3 rounds, 9 instruments were selected, while 39 other instruments were excluded. The HandART core set is an important step forward in clinical practice and research in this population, enabling clinicians and researchers to select the best available tests for their purposes and facilitate comparisons between clinical studies.
ACKNOWLEDGEMENTS
We are grateful for the contributions made by the following experts participating in the HandART-Delphi study (in alphabetical order):
OTs/hand therapists: Susanne Breier (Germany), Mira Burnstan (Switzerland), Ingela Carlsson (Sweden), Ragnhild Cederlund (Sweden), Melanie Eissens (The Netherlands), Christina Engstrand (Sweden), Irene Ghezzi (Italy), Angela Harth (Germany), Christina Jerosch-Herold (UK) and Beate Jung (Germany).
PTs/hand therapists: Monique Ardon (The Netherlands), Vera Beckmann-Fries (Switzerland), Ylva Gollbo (Sweden), Annemiek Hol (The Netherlands), Ali Kitis (Turkey), Cigdem Oksuz (Turkey), Karin Schoneveld (The Netherlands), Erna Veerman (The Netherlands) and Annemieke Videler (The Netherlands).
Both OTs and PTs/hand therapists: Liesbeth Hemelaers (Switzerland), and Eleonore Sleegers (The Netherlands).
Hand surgeons: Erwin Heine (The Netherlands), Ghita de Jongh (The Netherlands), Mati Merila (Estonia), Roberto Rosales (Spain), Igor Rossello (Italy) and Chiara Novelli (Italy).
Rehabilitation physicians: Agnes Hoeksma (The Netherlands), Anita Vetra (Latvia) and Corry van der Sluis (The Netherlands).
The study was financially supported by grants from the V!GO-Centre for Rehabilitation and Orthopedic Technology and from the Revalidatiefonds (Rehabilitation Fund)”, both of which are situated in the Netherlands.
REFERENCES

