Giedre Matuseviciene, MD1, Gunilla Eriksson, PhD 2,3 and Catharina Nygren DeBoussard, MD, PhD1
From the 1Department of Clinical Sciences, Karolinska Institutet and Department of Rehabilitation Medicine, Danderyd Hospital, 2Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Stockholm and 3Department of Neuroscience, Rehabilitation Medicine, Uppsala University, Uppsala, Sweden
OBJECTIVE: To evaluate measures of activity, participation and quality of life 3 months after mild traumatic brain injury and the effect of an early intervention for patients with an estimated high risk for problems after mild traumatic brain injury.
Patients: Consecutive patients attending the emergency room with mild traumatic brain injury.
DESIGN: Randomized controlled trial.
METHODS: Patients reporting < 3 symptoms after 10 days were considered to have a low risk for prolonged problems. Patients with ≥ 3 symptoms (high-risk patients) were randomized to a visit to a physician or treatment-as-usual. Data on self-reported limitations in activity, restrictions in participation, and quality of life were collected for all patients at 3 months.
RESULTS: At 3 months post-injury, low-risk patients reported good quality of life and significantly fewer problems in everyday life compared with high-risk patients. The intervention had no effect on activity, participation or quality of life.
CONCLUSION: Patients who report few symptoms early after mild traumatic brain injury are likely to have a good outcome regarding activity and participation. The intervention offered in this study, focusing on reassurance of a good outcome and treatment of comorbidities, had no effect.
Key words: mild traumatic brain injury; concussion; intervention; outcome; activity; participation; quality of life; sick leave.
J Rehabil Med 2015; 00: 00–00
Correspondence address: Giedre Matuseviciene, Department of Rehabilitation Medicine, Danderyd Hospital, SE-182 88 Stockholm, Sweden. E-mail: giedre.matuseviciene@ds.se
Accepted Aug 27, 2015; Epub ahead of print Nov 4, 2015
INTRODUCTION
Mild traumatic brain injury (MTBI) is common, with reported annual incidence rates of 100–300/100,000 population for hospital-treated MTBI and 600/100,000 population for all MTBI (1, 2). The prognosis is usually good (1, 3), but long-term disabilities are reported by a subgroup of patients. The reported frequency of long-term symptoms after MTBI ranges from 24% to 40% (4–6), most often comprises headache, fatigue and self-perceived cognitive deficits (6–8), and may impact on activity and participation and health-related quality of life (9, 10). There are few studies on the relationship between sick leave and MTBI, but a recent review found that best-available evidence is that most persons have returned to work 3-6 months after MTBI (11).
Previous studies provide some support for the effect of early educational interventions, but there is a clear need for more studies (12). The effect of interventions in some previous trials has probably been diluted by the inclusion of patients with good spontaneous recovery. Previous studies indicate that early symptom load may be used to predict outcome and thus to triage patients to no follow-up, or to preventive and therapeutic interventions (7, 13, 14). Stulemejer et al. further observed that few symptoms reported early (mean 9 days, range 0–37 days) after the injury, low levels of post-traumatic stress, and lack of premorbid physical problems, were associated with good outcome (13).
We have reported previously that an early intervention visit to a physician and further interventions, if needed, had no effect on self-reported symptoms in a randomized controlled trial (14). Previous studies demonstrate that symptoms correlate to some aspects of activity and participation after MTBI (7, 10), but more data in this respect may support the development of new interventions. We report here outcome with regard to activity and participation, as assessed by Rivermead Head injury Follow-Up Questionnaire (RHFUQ) (15) and the Occupational Gaps Questionnaire (OGQ) (16). The OGQ was developed to measure the individuals’ perception of participation in everyday activities (16) and is a valid measure across different diagnostic groups (17). We also explore whether low, early symptom load predicts a good outcome with respect to activity limitations and restrictions of participation. We hypothesized 1) that patients who report few symptoms early after MTBI will have a good outcome with regard to activity and participation at 3 months after the MTBI and 2) that the early intervention visit offered to patients who reported 3 or more symptoms early after MTBI might have beneficial effects on activity and participation. We also wanted to explore self-reported quality of life 3 months after MTBI in the 3 groups of patients, and sick leave 6 months before and 12 months after the injury.
METHODS
Study design and participants
The current paper is a second report on a randomized, controlled multicentre study (14) which was designed in accordance with the Consolidated Standards of Reporting Trials (CONSORT) (18). Analysis is based on the same study population as in the first paper (14). Patients were recruited prospectively from March 2008 until September 2009 at 7 regional and county hospitals in 5 Swedish cities. Inclusion criteria were: patients aged 15–70 years, presenting at the emergency room (ER) within 24 h of a closed head trauma, with loss of consciousness < 30 min and/or post-traumatic amnesia < 1 h and Glasgow Coma Scale 14–15 at the ER. Exclusion criteria were: need for neurosurgery or intensive care, other significant physical injury requiring surgery, significant on-going somatic or psychiatric disease with a probable impact on activities of everyday life, a history of MTBI requiring medical attention within 5 years, previous moderate or severe TBI, and insufficient knowledge of the Swedish language.
A total of 76 eligible patients declined study participation, they were younger and more often men than those who consented (mean age 29.6 vs 39.4 years, p < 0.001; 66% vs 45%, p = 0.003).
Intervention
All patients at all study centres were provided with the same written information about MTBI, along with information about the study and the informed consent, either at discharge or as early as possible after the visit to the ER. The information included examples of common symptoms, description of the common course of recovery and the probable good outcome.
Patients reporting < 3 symptoms were not randomized (non-randomized group), ≥ 3 symptoms were randomized to treatment-as-usual (TAU group), or early intervention (EIV group). The patients randomized to the TAU group as well as the patients in the non-randomized group were not offered any routine follow-up. If necessary, the patients could see a physician on their own initiative: in Sweden this is usually a general practitioner.
Patients randomized to the EIV group were offered a visit to a specialist in rehabilitation medicine, 14–21 days post-injury.
The visit was carried out according to a structured protocol and included;
• a detailed interview about current psychosocial conditions and occupation, and other prior and on-going somatic and psychiatric disorders and treatments;
• standard examination of somatic status, including neurological examination;
• screening for depression and anxiety using the Hospital Anxiety and Depression Scale;
• information about MTBI, reassurance about a favourable outcome, recommendations about a gradual return to ordinary activities and what to do in case the symptoms persist.
Any identified problem or co-morbidity related to the MTBI was discussed and, if necessary, treatment, for example, for pain, anxiety or depression, or referrals to other specialists were offered.
Baseline assessments
The Rivermead Post Concussion Symptoms Questionnaire (RPQ) (19) and the OGQ were administered twice, at baseline and follow-up for all patients.
Outcome measures
Outcome measures 3 months after the injury were self-reported limitations in activity and participation according to the RHFUQ and the OGQ, self-reported health-related quality of life according to the Short-Form 36 (SF-36), and sick leave. The OGQ was completed twice, 10 days and 3 months after injury, so that changes in perceived gaps could be analysed. Data on sick leave and disability pension 6 months before MTBI and 12 months after the injury were collected from the Swedish Social Insurance Agency. At follow-up all patients were asked to report any contact with healthcare providers.
Follow-up questionnaires
Rivermead Head Injury Follow-up Questionnaire (RHFUQ). The RHFUQ measures perceived injury-related changes in everyday activities and in aspects of participation, such as domestic activities, work, leisure and social interaction. The RHFUQ consists of 10 questions on a Likert scale: 1 no change; 2 have had symptoms, now resolved; 3 mild change; 4 moderate change; and 5 very marked change. Ratings “Mild change” to “Very marked change” (3–5) were merged into a single score, “problems”.
For evaluation of associations with age, sex and group (non-randomized, TAU and EIV) and for logistic regression analysis, RHFUQ was dichotomized into “good” (a sum of < 8 injury-related changes in everyday activities) and “unfavourable” (a sum of ≥ 8 injury related changes in everyday activities) outcome (20).
Occupational Gaps Questionnaire (OGQ). The OGQ is a questionnaire intended to measure perceived occupational gaps, i.e. to what extent an individual does what he or she wants to do. It also measures what the individual does but does not want to do. The presence of occupational gaps is examined for 28 activities, including 8 instrumental activities of daily living (I-ADL), 6 social activities, 10 leisure activities and 4 work or work-related activities. Each activity includes 2 questions: “Do you perform the activity now?” and “Do you want to perform the activity now?” Answering “Yes” to one question and “No” to the other question constitutes an occupational gap.
Data from the randomized and non-randomized groups 10 days after injury and 3 months after the injury were compared. Only those patients who answered 26–28/28 questions were included in analyses of gaps.
Short-Form Health Questionnaire (SF-36). SF-36 is a questionnaire that evaluates self-reported health-related quality of life (21) and is validated for general Swedish population (22).
The SF-36 includes 36 questions on 8 health scales: limitations in physical activities due to health problems; limitations in social activities due to physical or emotional problems; limitations in usual role activities due to physical health problems; bodily pain; general mental health (psychological distress and well-being); limitations in usual role activities due to emotional problems; vitality (energy and fatigue); and general health perceptions. The scales are summarized in 2 composite measures: physical composite score (PCS) and mental composite score (MCS).
Sick leave. Data on sick leave and disability pension 6 months before the MTBI and 12 months after the injury were collected from the Swedish Social Insurance Agency Register for each person in the study. A list of all 173 patients was sent to the agency asking for information about any compensated sick leave and disability pension. Due to an administrative error one patient was omitted from the list.
In Sweden, almost all employees have the right to be financially compensated when unable to work. Retirement in Sweden is usually at 65 years of age. The Swedish Social Insurance Agency provides compensation after 14 days of sick leave. The employer pays for the first 14 days of sick leave compensation. In the case of permanent inability to work a disability pension is granted full- or part-time. Data from the Social Insurance Agency include the main sick leave diagnoses, coded according to International Classification of Diseases (ICD-10) (23) at a 3-digit level. The diagnostic code S06 ”Intracranial injury” was used to detect patients with sickness absence due to MTBI
Sample size
Power calculation was based on a previous study by Lundin et al. (7). With an expected 50% decrease in symptom intensity in the intervention group and no change in the control group, a significance level of 5%, a power of 85% and expected difference in change equal to an effect size of 0.90, 24 patients were required in each group. With an expected dropout rate of 25%, 32 patients should be included in each group.
The study was approved by the ethics committee in Uppsala University, Uppsala, Sweden.
Randomization
Randomization was centralized. Consenting patients were asked to respond to a Swedish version of the RPQ at 10 days after the injury. Patients reporting 3 or more current symptoms (mild, moderate or severe) according to the RPQ at 10 days post-injury were defined as high-risk patients and those with fewer than 3 symptoms were defined as low-risk patients (defined below as non-randomized group). Patients fulfilling high-risk criteria were randomized in blocks of 4 to either an EIV or TAU.
Blinding
The data collector (GM) and statistician were blinded to group affiliation.
Statistical methods
Data were analysed using SPSS v. 22. All variables were analysed with descriptive statistics, such as frequency, mean and 95% confidence interval (95% CI), or median and interquartile range (IQR), when appropriate. Results of SF-36 were presented as median and IQR, since it is an ordinal scale; however, mean and 95% confidence interval are often presented and are therefore also included. Non-parametric tests were used when data were skewed. Kruskal–Wallis test were used for comparison between 3 groups and Mann-Whitney U test for comparison between 2 groups. Univariate binary logistic regression analysis was performed to explore association with outcome.
RESULTS
A flowchart of the participants and those who withdrew is shown in Fig. 1. Eighty-three percent of the patients completed the study.
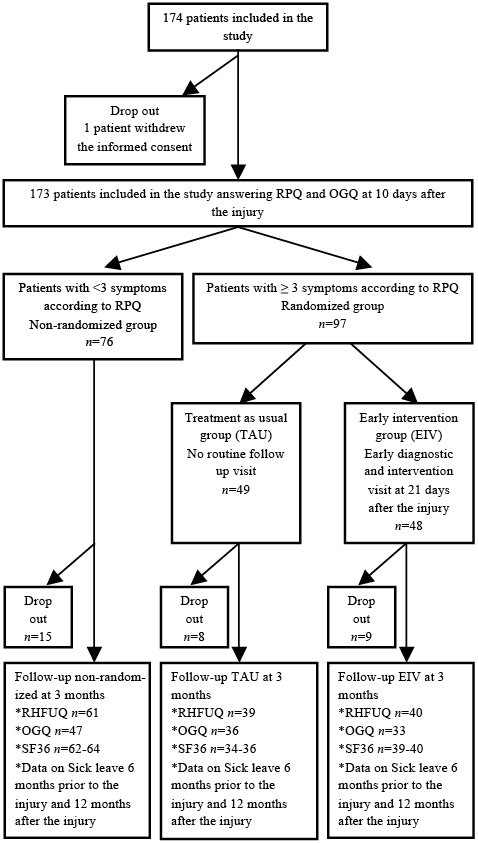
Fig. 1. Randomization, follow-up and withdrawals.
Demographic and clinical characteristics of the study sample are shown in Table I.
|
Table I. Sociodemographic and clinical characteristics of patients randomized to treatment-as-usual (n = 49) or to an early intervention (n = 48), and non-randomized patients (n = 76) |
||||
|
Characteristics |
Low risk |
High risk |
||
|
Non-randomized |
Treatment- as-usual |
Intervention |
||
|
Age, years, mean (range) |
39.6 (15–76) |
37.5 (15–68) |
41.0 (15–69) |
|
|
Men, n (%) Women, n (%) |
40 (53) 36 (47) |
23 (47) 26 (53) |
15 (31) 33 (69) |
|
|
Type of accident, n (%) Fall Car accident Bicycle accident Riding Sport Assault Other |
33 (43) 3 (4) 11 (15) 5 (7) 16 (21) 3 (4) 5 (7) |
14 (30) 1 (2) 7 (15) 9 (19) 9 (19) 3 (6) 4 (9) |
25 (53) 2 (4) 5 (11) 8 (17) 2 (4) 3 (6) 2 (4) |
|
|
Positive test of alcohol in blood, n (%) |
13 (24) |
3 (9) |
4 (12) |
|
|
GCS, mean (range) |
14.9 (12–15) |
15.0 (14–15) |
14.9 (14–15) |
|
|
CT scan examination, n (%) |
8 (13) |
4 (10) |
4 (9) |
|
|
GCS: Glasgow Coma Scale; CT: computed tomography. |
||||
There were no significant differences between the groups, except for a larger proportion of falls as an injury mechanism in the EIV group (p = 0.012).
Outcome regarding activity and participation
The proportion of patients in the EIV group, TAU group and non-randomized groups, who reported having no change in activity and participation items in the RHFUQ, as well as having had problems and having persistent problems in the different items is shown in Fig. 2.
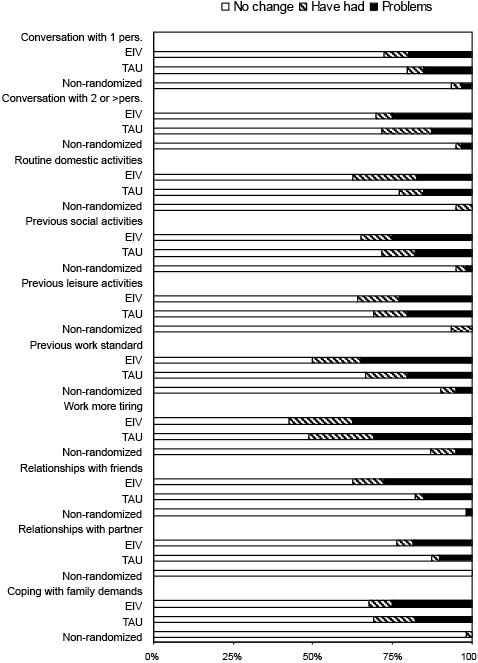
Fig. 2. Proportion of patients in early intervention (EIV), treatment-as-usual (TAU) and non-randomized groups who responded to questions in Rivermead Head injury Follow-Up Questionnaire (RHFUQ) as: (i) ”no change”, (ii) ”have had symptoms, now resolved”, and (iii) ”problems” (mild to very marked change).
A significant difference in the number of activities in which the patients have problems was found between the EIV and non-randomized group (p < 0.001), and between the TAU and non-randomized group (p < 0.001), but no significant difference between the 2 randomized groups. The item “Work more tiring” was the highest rated item in all groups.
Regarding occupational gaps, a significant difference (p < 0.001) between the groups was found in change over time, both between the EIV and non-randomized and the TAU and non-randomized (Fig. 3). A significant difference between the EIV and non-randomized (p < 0.01) and between the TAU and non-randomized groups (p < 0.01) was shown at 10 days after the MTBI, but not when the EIV was compared with the TAU group (p < 0.88). In all groups, the EIV, TAU and non-randomized groups, activities in IADL, i.e. shopping, cooking, washing clothes, cleaning, performing light maintenance, and managing personal finances, were predominately reported as the type of gap “doing but not wanting to do” at 10 days after injury as well as at 3 months after injury.
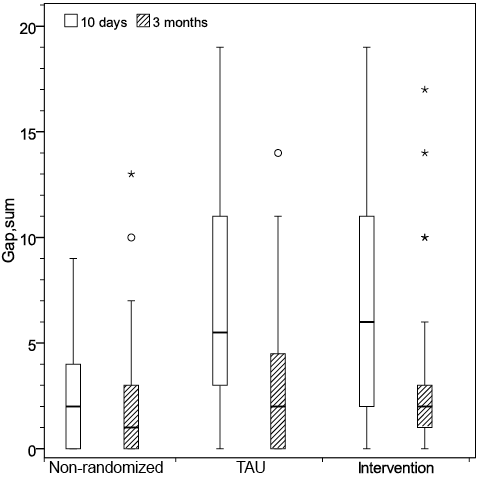
Fig. 3. Sum of perceived occupational gaps at 10 days and at 3 months after mild traumatic brain injury. TAU: treatment as usual.
In the EIV and TAU groups the dominant gap in leisure and social activities, (such as sports, seeing relatives and friends, engaging in societies, clubs and unions) was “not doing but wanting to do”. The non-randomized group had a low number of occupational gaps in all items at both time-points. However, there was no significant difference in the number of gaps between patients in the EIV group and patients in the TAU group at 10 days or 3 months after the injury. “Seeing partner and children” in the social activity domain had the highest number of reported occupational gaps in all 3 groups at 10 days after injury.
Quality of life
Analysis of SF-36 data revealed a significant difference between 3 patient groups in the following scales: Vitality, Mental Health and Bodily Pain (Table II). A significant difference (p < 0.05) was present between the EIV and non-randomized groups in Vitality, Mental Health, Bodily Pain and Role Physical. Between the TAU and non-randomized groups there was a significant difference in Vitality, General Health and Role Emotional.
|
Table II. Short-Form 36 (SF-36) results in study groups and in the general Swedish population |
|||||||
|
SF-36 |
Mean |
95% CI |
Median |
25th–75th percentile |
p-value between groups |
||
|
All |
EIV and non-randomized |
TAU and non-randomized |
|||||
|
Physical Functioning (PF) |
|||||||
|
EIV |
89.0 |
82.9–95.0 |
95 |
85–100 |
|||
|
TAU |
89.0 |
84.2–93.9 |
95 |
80–100 |
|||
|
Non-randomized |
92.3 |
88.7–96.0 |
100 |
95–100 |
0.156 |
0.172 |
0.730 |
|
Swedish norm* |
87.9 |
87.5–88.3 |
95 |
85–100 |
|||
|
Role-Physical (RF) |
|||||||
|
EIV |
67.9 |
54.5–81.3 |
100 |
25–100 |
|||
|
TAU |
75.7 |
63.5–87.9 |
100 |
50–100 |
|||
|
Non-randomized |
82.9 |
74.7–91.2 |
100 |
75–100 |
0.104 |
0.038 |
0.209 |
|
Swedish norm* |
83.2 |
82.5–83.8 |
100 |
75–100 |
|||
|
Bodily Pain (BP) |
|||||||
|
EIV |
70.3 |
61.4–79.3 |
74 |
46–100 |
|||
|
TAU |
75.5 |
66.7–84.4 |
84 |
52–100 |
|||
|
Non-randomized |
83.7 |
78.1–89.3 |
100 |
72–100 |
0.043 |
0.017 |
0.122 |
|
Swedish norm* |
74.8 |
74.3–75.4 |
84 |
52–100 |
|||
|
General Health (GH) |
|||||||
|
EIV |
74.5 |
66.4–82.7 |
82 |
54–96 |
|||
|
TAU |
73.7 |
65.6–81.9 |
80 |
57–95 |
|||
|
Non-randomized |
84.2 |
79.7–88.6 |
92 |
77–97 |
0.059 |
0.087 |
0.027 |
|
Swedish norm* |
75.8 |
75.4–76.3 |
82 |
62–92 |
|||
|
Vitality (VT) |
|||||||
|
EIV |
53.6 |
44.8–62.4 |
55 |
30–72 |
|||
|
TAU |
62.5 |
54.5–70.5 |
60 |
45–80 |
|||
|
Non-randomized |
73.1 |
67.7–78.6 |
80 |
60–90 |
0.001 |
< 0.001 |
0.023 |
|
Swedish norm* |
68.8 |
68.3–69.3 |
75 |
55–85 |
|||
|
Social Functioning (SF) |
|||||||
|
EIV |
80.1 |
71.6–88.7 |
100 |
75–100 |
|||
|
TAU |
84.9 |
77.4–92.4 |
100 |
75–100 |
|||
|
Non-randomized |
89.7 |
85.2–94.2 |
100 |
88–100 |
0.194 |
0.075 |
0.311 |
|
Swedish norm* |
88.6 |
88.2–89.0 |
100 |
88–100 |
|||
|
Role-Emotional (RE) |
|||||||
|
EIV |
76.7 |
64.5–88.8 |
100 |
66–100 |
|||
|
TAU |
74.1 |
60.6–87.6 |
100 |
66–100 |
|||
|
Non-randomized |
88.4 |
80.9–95.8 |
100 |
100–100 |
0.052 |
0.054 |
0.024 |
|
Swedish norm* |
85.7 |
85.0–86.3 |
100 |
100–100 |
|||
|
Mental Health (MH) |
|||||||
|
EIV |
72.6 |
66.4–78.9 |
76 |
64–88 |
|||
|
TAU |
79.2 |
73.8–84.6 |
84 |
72–92 |
|||
|
Non-randomized |
82.2 |
77.5–86.9 |
88 |
72–96 |
0.013 |
0.005 |
0.121 |
|
Swedish norm* |
80.9 |
80.5–81.3 |
88 |
72–96 |
|
|
|
|
*Norms for general Swedish population, n = 8,930. EIV n = 39–40, TAU n = 34–36, non-randomized n = 62–64. 95% CI: 95% confidence interval; EIV: early intervention; TAU: treatment as usual. |
|||||||
Moreover, a significant difference (p < 0.05) was observed in Mental Component Score between the 3 groups and between the EIV and non-randomized and TAU and non-randomized (Fig. 4).
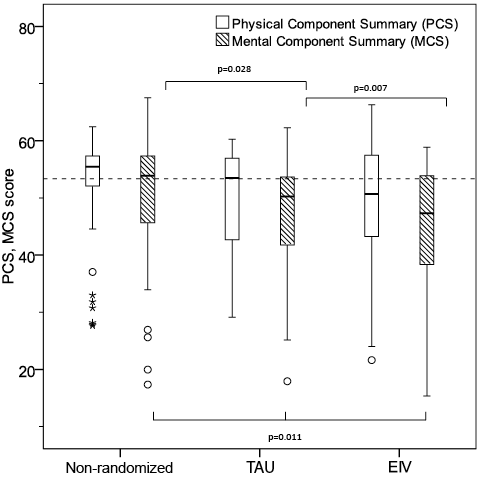
Fig. 4. Short-Form 36 (SF-36) summary measures: physical component score and mental component score. TAU: treatment as usual; EIV: early intervention.
Univariate logistic regression analysis
Univariate logistic regression analysis demonstrated that group affiliation (non-randomized, TAU or EIV), but not age or gender, were associated with outcome at 3 months after the injury.
Contacts with healthcare providers
In the EIV group 15 patients, all women, reported contact with healthcare due to MTBI, the corresponding number in the TAU group was 3 men and 8 women with no significant difference between the randomized groups. In the non-randomized group 8 patients had contact with some healthcare providers due to the MTBI (2 men, 6 women).
Sick leave
Nine patients (5%) were on sick leave at some time in the period 6 months before the MTBI. Eleven patients (6.4%) had a full- or part-time disability pension at the time of the injury and afterwards.
Fifteen patients (8 in EIV, 6 in TAU and 1 in non-randomized group) were on sick leave after MTBI with the ICD-10 diagnosis ”Intracranial injury” S06. Thirteen patients were on sick leave with other diagnoses than S06.
DISCUSSION
In this study patients who reported few symptoms early after MTBI had few limitations in activities and participation and were not on sick leave 3 months after the injury. Furthermore, these patients reported a good quality of life 3 months after the MTBI. Thus, our hypothesis that patients who report few symptoms early after an MTBI will have a good outcome is supported. This is in line with the findings reported by Stulemeijer et al., where patients with no comorbidity and low levels of early symptoms had a 90% chance of a good outcome without post-concussional symptoms (13).
Similar symptoms as those reported after MTBI are also reported in the acute stages of other injuries and are also associated with pain, depression (24), anxiety, post-traumatic stress (25) and other injury-related factors (26–28). This has hampered the design of intervention trials to prevent and treat disabilities after MTBI. In this study the intervention was intended to identify treatable co-morbidities and offer reassurance regarding a favourable outcome. However, the hypothesis that the treatment offered in this study would also have a beneficial effect on outcome regarding activity and participation for patients who still have symptoms at 3 months after the MTBI, was not supported. No significant differences were found between the EIV and TAU groups in any of the self-reported activity and participation measures.
The Occupational Gap Questionnaire was used twice; early after the MTBI and at follow-up, allowing analysis of changes in perceived gaps, thus lowering the risk of recall bias. No difference was found in reported occupational gaps in the EIV and TAU group. One possible reason for this might be that the OGQ is not sensitive enough to capture minor restrictions in participation in everyday activities in a sample with reasonably well-functioning persons with good ability in performance of daily activities. Nevertheless, a significantly lower frequency of reported occupational gaps were found in the non-randomized group compared with the EIV and TAU groups, which further supports that patients reporting few symptoms early after MTBI have a good prognosis with no need of follow-up.
Another finding, although not statistically significant, was that in all RHFUQ items and in the OGQ a slightly higher frequency of self-reported problems was found in the EIV group compared with the TAU group. In our study all patients received written information about MTBI at the earliest opportunity after discharge. Patients in the EIV group received further information at the visit to the doctor. Although the intention was to reassure that the outcome is likely to be favourable, the visit to the doctor might instead have increased the patient’s attention to possible problems after MTBI. If a patient in the EIV group had some problems at follow-up, the patient might therefore more easily attribute the problem to the MTBI. The psychological factor “diagnostic threat” has been discussed as a factor contributing to poorer cognitive performance after MTBI (29). In that study cognitive performance in tests was compared in 2 groups. The participants who were informed that the tests were done because they had had MTBI performed worse than the other group with no information about the link to a former MTBI. In line with this, the awareness of possible problems that might occur after MTBI and treatable comorbidities screened for at the doctors visit might affect experience and reporting of any problem at follow-up.
It is well known that MTBI is more common in males than females (30). Women, however, have been found to be at higher risk of unfavourable outcome (31, 32). In our study, despite randomization, there were more women in the intervention group than in the TAU group. Since recent studies have shown that female sex is associated with increased risk of long-term problems after MTBI, participants in this study were probably more at risk of long-term problems (32, 33). At follow-up 3 months after MTBI there were few patients reporting contact with healthcare providers in all 3 groups. However, there were more contacts in the early intervention group compared with the TAU group, but the difference was not significant difference, and it was predominantly women who had had healthcare contacts. This is in line with the findings of a systematic review (33), in which women were found to use more healthcare services.
Personal traits and coping strategies have been proposed to have an impact on how patients report problems and quality of life after MTBI (34, 35). In the current study, patients in the non-randomized group reported higher quality of life than the Swedish norm population. Patients in the EIV and TAU groups reported a lower mental summary score, mostly due to lower vitality, than the non-randomized patients. Thus, the intervention offered in this study did not have any impact on self-reported quality of life, since no difference was found in the randomized groups. One might speculate that patients who report few symptoms early after MTBI might have coping strategies and personal traits that affect self-reported quality of life.
Although some patients in the EIV and TAU groups did report having limitations in activity and restrictions in participation, according to the RHFUQ and OGQ at 3 months after injury, sick leave more than 14 days after MTBI was uncommon. This is in line with a recent study, in which it was found that more than 50% of patients returned to work within 2 weeks after MTBI (36). Our data do not provide evidence that health insurance benefits, such as sick leave or disability pension before the MTBI, increases the risk of prolonged symptoms or disabilities after the injury.
Study limitations
Due to the policy of sick leave compensation in Sweden it was not possible to explore the frequency and length of sick leave in the first 14 days after MTBI in our study. The patients with only a few or no days off work after MTBI are likely to be those with positive expectations and good coping strategies, which have been shown to be related to shorter recovery times after MTBI (34).
Despite the multicentre design and a study nurse at each site protecting against selection bias, some eligible patients may have been missed and the study sample may not be representative of those who present to the emergency department following MTBI.
The generalizability of the results from this study might be affected by the fact that the study participants were older than those who declined to participate, and there were more females in the intervention group. Thus, the results may primarily be applied to patients who are older and female.
Conclusion
In conclusion, patients who report few symptoms early after an MTBI are likely to have a good outcome regarding activity and participation. Symptom screening early after MTBI may be used to detect patients with an expected favourable outcome and no need for follow-up. This might be due to personal trait and coping strategies, as indicated by the finding that patients who reported few symptoms early after the MTBI also reported better quality of life than the general Swedish population. There is still a lack of effective treatment for problems occurring after MTBI. The intervention offered in this study, focusing on the reassurance of a good outcome and treatment of comorbidities, did not have any effect in a group of patients who reported 3 or more symptoms early after MTBI. The results from this study lend support to the need for the early identification of patients at risk of long-term problems. Furthermore, early provision of structured educational information to all patients at the ED is also recommended. Interventions for patients with problems after MTBI should be individualized and based on the assessment of symptoms, comorbidities, activity and participation.
ACKNOWLEDGEMENTS
The authors would like to thank the patients, SIC study collaborators in Uppsala, Gothenburg, Umeå and Jönköping, and colleagues in the emergency room for enabling recruitment of their patients. This study was supported by a grant from AFA Insurance. The funders had no access to the data and provided no input to the study design or data analysis. GM and CNB received support from ALF-grants from Danderyd Hospital. The authors thank Seija Lund and Sandra Hallström, nurses and coordinators, and Lisbet Broman for all help with tables, figures and advice on statistical aspects. We also thank Professor Jörgen Borg for valuable support.
The authors declare no conflicts of interest.
REFERENCES

