Ingrid G. L. van de Port, PhD1, Gert Kwakkel, PhD, PT2,3 and Harriet Wittink, PhD, PT4
From the 1Revant Rehabilitation Centre Breda, Breda, 2Department of Rehabilitation Medicine, MOVE Research Institute Amsterdam, Vrije Universiteit Medical Center, 3Department of Neurorehabilitation, Reade Center for Rehabilitation and Rheumatology, Amsterdam and 4Research Group Lifestyle and Health, Utrecht University of Applied Sciences, Utrecht, The Netherlands
OBJECTIVE: To systematically review the use of cardiopulmonary exercise testing in people who have survived a stroke. The following questions are addressed: (i) What are the testing procedures used? (ii) What are the patient, safety and outcomes characteristics in the cardiopulmonary exercise testing procedures? (iii) Which criteria are used to determine maximum oxygen uptake (VO2peak/max) in the cardiopulmonary exercise testing procedures?
METHODS: Systematic review of studies of cardiopulmonary exercise testing in stroke survivors. PubMed, EMBASE, and CINAHL were searched from inception until January 2014. MeSH headings and keywords used were: oxygen capacity, oxygen consumption, oxygen uptake, peak VO2, max VO2, aerobic fitness, physical fitness, aerobic capacity, physical endurance and stroke. Search and selection were performed independently by 2 reviewers. Sixty studies were scrutinized, including 2,104 stroke survivors.
RESULTS: Protocols included treadmill (n = 21), bicycle (n = 33), stepper (n = 3) and arm (n = 1) ergometry. Five studies reported 11 adverse events (1%). Secondary outcomes were reported in few studies, which hampered interpretation of the patient’s effort, and hence the value of the VO2peak.
CONCLUSION: Most studies did not adhere, or insufficiently adhered, to the existing cardiopulmonary exercise testing guidelines for exercise testing. Thus, the results of cardiopulmonary exercise testing protocols in stroke patients cannot be compared.
Key words: stroke; cardiopulmonary exercise testing; systematic review; cardiopulmonary exercise tests; oxygen uptake.
Correspondence address: Ingrid GL van de Port, Revant Rehabilitation Centre Breda, Breda, The Netherlands. E-mail: i.vandeport@revant.nl
J Rehabil Med 2015; 47: 881–900
Accepted Sep 28, 2015; Epub ahead of print Nov 9, 2015
INTRODUCTION
The role of maximal cardiopulmonary exercise tests (CPETs) after stroke to assess cardiorespiratory fitness is of increasing interest. Several national and international organizations have issued guidelines for the optimal conduct and interpretation of CPET (1–5). However, in a recent systematic review of the correlation between aerobic capacity and walking capacity after stroke, we found that results regarding maximal CPETs were difficult to interpret due to methodological differences and incomplete reporting (6). Equally, Stoller et al. (7) reported in a systematic review that “there is a lack of a precise description regarding termination criteria for exercise testing and evaluation of aerobic capacity in most of the included studies”. Smith et al. (8) also noted in a systematic review that studies used different criteria for termination of exercise testing, and often failed to report which instructions patients were given prior to CPET. Despite the increased use of CPET after stroke, few data are available about the feasibility and safety of CPET testing after stroke (2), and different protocols are used.
Aerobic capacity (VO2 ml/kg/min), as an accepted measure of cardiorespiratory fitness, is the most commonly reported outcome of maximal CPET with open circuit spirometry. The classical outcome of a CPET is a levelling off, or “plateau”, in VO2 despite a continued increase in exercise intensity, the so-called “true” VO2max (9). In the absence of a plateau response, a series of secondary criteria can be used to confirm the maximum attainable effort. These include percentage of age-predicted maximum heart rate (APMHR), respiratory exchange ratio (RER) (≥ 1.15), and lactate (> 8 mmol/l) or rating of perceived exertion (> 8 on the 10-point Borg scale) (5, 10, 11). For clinical populations, a peak oxygen uptake (VO2peak) value, rather than a VO2max, is often reported, which is the highest VO2 attained before symptom limitation (12) in patients who make maximum effort.
Many studies have used aerobic capacity, expressed as VO2 peak, as an outcome measure to determine the effectiveness of an intervention, or to design intervention protocols based on exercise intensity. In addition, CPET can be used as a diagnostic tool before the start of a physical exercise programme to detect cardiac, pulmonary and/or muscular limitations/abnormalities (13). These important applications of CPET for both clinical and scientific goals require that maximal exercise testing should be conducted and reported according to the published guidelines and criteria.
The aim of the present study was to systematically review the use of CPET in people who have survived a stroke, whether used for diagnostic purposes or to assess functional capacity. The following questions were addressed:
• What testing procedures are being used, with respect to equipment, testing protocol and criteria for test termination?
• What are the patient, safety and outcomes characteristics in CPET procedures described in the literature?
• Which criteria are being used to determine maximum oxygen uptake (VO2peak/max) in the CPET procedures described in the literature?
The specific problems of hemiparesis, muscle weakness, fatigue, lack of balance, contractures and spasticity experienced by stroke survivors can interfere with effective testing with standard protocols (14) and might influence the reported outcomes. Answering the above questions will enable us to judge critically the quality of the outcomes of CPET in people after stroke in relation to the known guidelines for conducting CPET. Based on the above findings we can offer recommendations for the use of CPET in stroke research and practice (15).
METHODS
Data sources and searches
Potentially relevant studies were identified through computerized and manual searches. The electronic databases PubMed (up to 19 December 2013), EMBASE (up to 4 January 2014), and CINAHL (up to 19 December 2013) were systematically searched from inception. The following MeSH headings and keywords were used: oxygen capacity, oxygen consumption, oxygen uptake, peak VO2, max VO2, aerobic fitness, physical fitness, aerobic capacity, physical endurance and stroke. These were defined for use in PubMed, and adapted for use in the other databases. The PubMed search strategy was as follows: (((Stroke[Mesh] OR stroke[Tiab]))) AND ((oxygen capacity[Tiab] OR oxygen consumption[Tiab] OR oxygen uptake[Tiab] OR peak VO2[Tiab] OR max VO2[Tiab] OR aerobic fitness[Tiab] OR physical fitness[Tiab] OR aerobic capacity[Tiab] OR physical endurance[Tiab])), where Tiab = title plus abstract search. Reference lists of the included articles were also screened for relevant publications. The search was conducted under the supervision of a medical librarian. This review is written in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. No specific review protocol was used.
Study selection
The following inclusion criteria were used for studies: (i) participants were stroke survivors according to the World Health Organization (WHO) definition and were older than 18 years; (ii) a maximum exercise test was conducted using gas exchange analysis and at least maximum oxygen uptake (VO2max) or peak oxygen uptake (VO2peak) was reported; (3) the study was published in English, German or Dutch.
Baseline measures were used if a study had a longitudinal design and/or was a part of a controlled trial. In the case of multiple publications on the same patient population, the most relevant study was included. Reviews and grey literature were excluded.
Screening was performed by 2 independent reviewers (IvdP and HW). For each article, any discrepancy between the 2 reviewers was resolved by discussion. In the first screening stage (titles plus abstracts), studies were included when both reviewers agreed they were eligible for inclusion, or if there was doubt about whether to exclude them. In the second screening stage (full text), studies were included when both reviewers felt they met all the inclusion criteria.
Data extraction
Relevant study characteristics were extracted and described: (i) the characteristics of the population, (ii) the test protocol used to conduct the CPET and the termination guidelines referred to; (iii) the criteria used to determine maximum exercise effort; (iv) adverse events during the test; (v) key measurement outcomes reported, namely VO2peak or VO2max values, and percentage of age-predicted maximal heart rate or measured peak heart rate and/or, RER value and/or systolic and diastolic blood pressure (BP). When data were missing, the corresponding author of the manuscript was contacted.
RESULTS
Study selection
A total of 3,385 articles were identified initially (Fig. 1). After duplications had been removed, titles were screened and the abstracts of 589 relevant articles were screened. In this second stage, 163 articles were selected for full-text screening. Eighty-seven articles did not fulfil the inclusion criteria. Two articles were unavailable full-text and 14 articles were excluded because they described a population that was also included in another study. One study was included after a hand search and one was excluded because it was a duplicate. In total, 60 peer-reviewed articles were included based on our inclusion criteria. The extracted study and population characteristics, protocols and outcomes are shown in Tables I and II.
|
Table I. Patient and study characteristics |
|||||
|
Study |
n (% male) |
Setting/Period after stroke |
Age (years) |
Beta-blockers (%) |
Time since stroke (mean) |
|
Treadmill with BWS |
|||||
|
Mackay-Lyons & Makrides, 2004 (36) |
25 (80) |
Stroke unit |
Mean: 64.1 |
52 |
26.0 days |
|
MacKay Lyons et al., 2013 (37) |
50 (58) |
Acute (< 1 month) |
Mean: I: 61.5 C: 59.0 |
I: 32 C: 44 |
I: 23.3 days C: 23.1 days |
|
Stoller et al., 2013 (20) |
3 (100) |
Acute (< 8 weeks) |
Mean: 53.7 |
0 |
Median: 26.3 days |
|
Treadmill |
|||||
|
Askim et al., 2013 (45) |
14 (64) |
3–9 months |
Mean: 70.0 |
21 |
5.8 months |
|
Dobrovolny et al., 2003 (48) |
53 (83) |
> 6 months |
Mean: 64 |
NR |
NR |
|
Gjellesvik et al., 2012 (64) |
8 (50) |
> 6 months |
Mean: 48.9 |
37.5 |
7.2 years |
|
Globas et al., 2012 (65) |
36 (81) |
> 6 months |
Mean: 68.7 |
NR |
65.1 months |
|
Hill et al., 2012 (18) |
10 (60) |
Community |
Mean: 46.3 |
0 |
7.4 years |
|
Ivey et al., 2010 (66) |
53 (54) |
Chronic |
Mean: 61 |
NR |
> 6 months |
|
Kim et al., 2013(46) |
55 (67) |
< 3 months |
Mean: 62.2 |
0 |
32.6 days |
|
Lee et al. 2013 (67) |
16 (50) |
< 6 months |
Mean: 63.3 |
NR |
I: 62.5 days C: 57.4 days |
|
Luft et al., 2008 (68) |
71 (46) |
> 6 months |
Mean: I: 63.2 C: 63.6 |
25 |
I: 62.5 months C: 44.6 months |
|
Macko et al., 2001 (69) |
23 (83) |
> 6 months |
Mean: 67 |
17 |
28 months |
|
Macko et al., 2005 (70) |
61 (70) |
> 6 months |
Mean: I: 63 C: 64 |
16.3 |
I: 35 months C: 39 months |
|
Michael et al., 2005 (71) |
50 (55) |
Community (> 6 months) |
Mean: 65 |
NR |
10.3 months |
|
Michael et al., 2009 (26) |
10 (70) |
Community |
Mean: 71 |
NR |
7.5 years |
|
Michael et al., 2006 (72) |
53 (59) |
> 6 months |
Mean: 66 |
NR |
10.3 months |
|
Ovando et al., 2011 (73) |
8 (75) |
> 6 months |
Mean: 53 |
50 |
18 months |
|
Patterson et al., 2007 (74) |
74 (58) |
> 6 months |
Mean: 64 |
NR |
48 months |
|
Stookey et al., 2012 (75) |
43 (70) |
Community |
Mean: 61.5 |
NR |
> 6 months > 12 months (haemorrhagic) |
|
Yang et al., 2007 (76) |
15 (60) |
< 1 year |
Mean: 64 |
NR |
|
|
Arm ergometrie |
|||||
|
Sutbeyaz et al., 2009 (34) |
45 (53) |
< 12 months |
Mean: I1: 60.8 I2: 62.8 C: 61.9 |
0 |
I1: 156.0 days I2: 155.1 days C: 163.2 days |
|
Bicycle recumbent semi |
|||||
|
Brooks et al., 2008 (63) |
45 (58) |
< 3 months |
Mean: 65.2 |
20 |
16.2 days |
|
Chang et al., 2012 (77) |
37 (62) |
< 1 month |
Mean: I: 55.5 C: 59.7 |
NR |
I: 16.1 days C: 18.2 days |
|
Jakovljevic et al., 2012 (21) |
28 (100) |
NR |
Mean: 70 |
0 |
19 months |
|
Kelly et al., 2003 (12) |
17 (76) |
< 6 weeks |
Median: 66 |
0 |
Median: 30 days |
|
Koopman et al., 2013 (78) |
11 (64) |
Rehabilitation |
Mean: 53.9 |
18 |
NR |
|
Olivier et al., 2013 (55) |
21 (57) |
Community (cognitive impairment) |
Mean: 64.3 |
29 |
44.9 months |
|
Salbach et al., 2013 (19) |
16 (88) |
Community, > 3 months |
Mean: 71.1 |
25 |
2.0 years |
|
Tang et al., 2006 (39) |
35 (54) |
< 3 months |
Mean: 65.7 |
14 |
17.6 days |
|
Tomczak et al., 2008 (27) |
10 (40) |
> 1 year |
Mean: 54 |
30 |
7.5 years |
|
Recumbent stepper total |
|||||
|
Billinger et al., 2012 (30) |
10 (60) |
< 6 months |
Mean: 61.2 |
20 |
68.6 days |
|
Billinger et al., 2010 (29) |
12 (42) |
Chronic |
Mean: 60.6 |
33 |
69.1 months |
|
Tseng et al., 2010 (31) |
21 (57) |
Chronic |
Mean: 59.5 |
NR |
4.1 years |
|
Bicycle upright |
|||||
|
Baert et al., 2012 (79) |
40 (65) |
Rehabilitation |
Mean: 57.2 |
NR |
3 months |
|
Carvalho et al., 2008 (41) |
34 (71) |
Community |
Mean: 60 |
44 |
62 months |
|
Chen et al., 2013 (80) |
64 (80) |
< 2 weeks |
Mean: 59.2 |
11 |
8.6 days |
|
Chen et al., 2010 (23) |
19 (100) |
< 2 weeks |
Mean: 62.7 |
NR |
9.9 days |
|
Courbon et al., 2006 (81) |
21 (86) |
> 3 months |
Mean: 53.4 |
33 |
24.5 months |
|
Eng et al., 2004 (14) |
12 (92) |
> 1 year |
Mean: 62.5 |
NR |
3.5 years |
|
Fujitani et al., 1999 (24) |
3 (100) |
2–49 months |
Mean: 53.6 |
NR |
10.1 months |
|
Janssen et al., 2008 (51) |
12 (50) |
> 5 months |
Mean: I: 54.2 C: 55.3 |
NR |
I: 12.3 months C: 18.3 months |
|
Table I. Contd. |
|||||
|
Study |
n (% male) |
Setting/Period after stroke |
Age (years) |
Beta-blockers (%) |
Time since stroke (mean) |

|
Jin et al., 2013(17) |
128 (71) |
> 6 months |
Mean: I: 57.6 C: 56.3 |
20.3 |
I:18.7 months C: 17.9 months |
|
Katho et al., 2002 (82) |
20 (80) |
Community |
Mean: 64 |
NR |
22 months |
|
Lee et al., 2008 (83) |
48 (58) |
Community dwelling |
Mean: 63.2 |
17 |
57.0 months |
|
Letombe et al., 2010 (40) |
18 (61) |
Acute |
Mean: I: 59.1 C: 60.9 |
26 |
I: 21 days C: 20 days |
|
Murakami et al., 2002 (84) |
29 (79) |
Inpatient rehabilitation |
Mean: 55 |
NR |
76 days |
|
Pang et al., 2005 (47) |
63 (57) |
> 1 year |
Mean: 65.3 |
11 |
5.5 years |
|
Potempa et al., 1995 (85) |
42 (55) |
> 6 months |
Range: 43–72 |
21 |
NR |
|
Rimmer et al., 2009 (42) |
55 (40) |
> 6 months |
Mean: 59.6 |
NR |
NR |
|
Rimmer et al., 2000 (43) |
35 (26) |
> 6 months |
Mean: 53.1 |
NR |
NR |
|
Severinsen et al., 2011 (86) |
48 (73) |
Community |
Median: 68 |
13 |
Median: 18 months |
|
Stibrant Sunnerhagen, 2007 (25) |
30 (100) |
> 6 months |
Mean: I: 53 C: 50 |
NR |
I: 16 months C: 15 months |
|
Tang et al., 2013 (87) |
35 (65) |
Community |
Mean: 66.9 |
31 |
Median: 3.7 years |
|
Teixeira da Cunha Filho et al., 2001 (22) |
12 (100) |
< 6 weeks |
Mean: I: 57.8 C: 59.7 |
NR |
I: 15.67 days C: 14.33 days |
|
Tseng & Kluding, 2009 (88) |
9 (22) |
<6 months |
Mean: 56.8 |
NR |
47.6 months |
|
Yates et al., 2004 (44) |
100 (= completers) (66) |
30–150 days |
Mean: 69.8 |
19 |
70 days |
|
Mixed |
|||||
|
Billinger et al, 2008 (28) |
11 (64) |
NR |
Mean: 60.9 |
82 |
40.1 months |
|
Marzolini et al, 2012 (33) |
98 (69) |
Community |
Mean: 63.3 |
43 |
89.7 weeks |
|
Tang et al., 2010 (32) |
43 (70) |
> 3 months |
Mean: 64.5 |
NR |
30 months |
|
n: number; I: intervention; C: control; NR: not reported; CWS: comfortable walking speed; ACSM: American College of Sports Medicine; AHA: American Heart Association; RC: reliability coefficient; CT: clinical trial. |
|||||
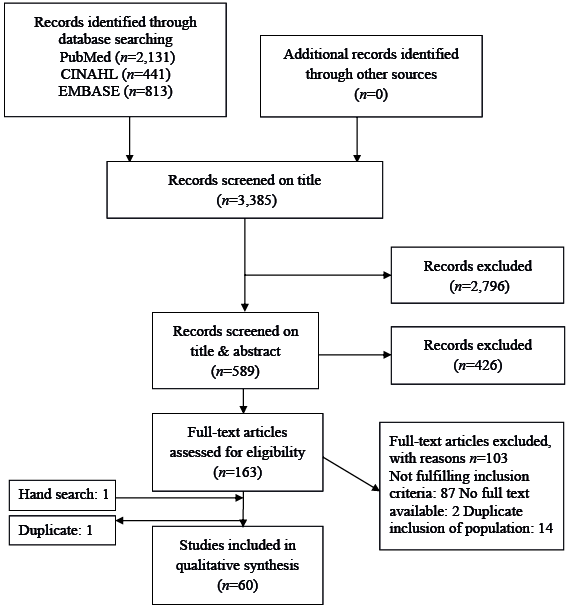
Fig. 1. Flow chart of included studies.
|
Table II. Cardiopulmonary exercise testing protocols and outcomes |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Treadmill studies with BWS |
|||||||||
|
Mackay-Lyons & Makrides, 2004 (36) |
Protocol: MacKay Lyons (2001, 2002) Warm-up: 1-min 60 –70% CWS Start: Self-selected speed, 0% incline, 2 min Increase: 2.5% incline/2 min until 10%. Thereafter 0.05m/s increase/ 2 min Termination: maximum effort, ACSM guidelines |
VO2peak ICC: 0.94 HRpeak ICC: 0.93 (MacKay Lyons, 2002) |
(1) V̇O2 plateau (< 150 ml in last min), (2) RER> 1.0, (3) SBP > 200 mmHg, (4) HRpeak < 15 bpm of APMHR |
One or more of the V̇O2max criteria were met in 62 (65%) tests |
No adverse events |
14.8 (5.3) |
RER: 1.00 (0.07) |
NR |
NR |
|
MacKay Lyons et al., 2013 (37) |
Protocol: MacKay Lyons 2001 Start: Self-selected speed, 0% incline, 2 min Increase: 2.5% incline/2 min until 10%. Thereafter 0.05 m/s increase/2 min Termination: ACSM guidelines |
VO2peak ICC: 0.94 HRpeak ICC: 0.93 (MacKay Lyons, 2002) |
NR |
NR |
No adverse events |
I: 14.2 (4.3) C: 14.5 (3.5) |
Total: 1.01 (0.08) |
Total: 128.3 (15.4) |
NR |
|
Stoller at al., 2013 (20) |
Walk passively 5 min, walk actively by pushing against exoskeleton until volitional exhaustion, walk passively 5 min Termination: abnormal BP, individual Pmech below 40% Pmechmax > 30 s, APMHR, pain/ discomfort in chest |
NR |
NR |
RER>1.0: 66% |
No adverse events |
19.7, 19.8, 28.8 |
1.11, 0.95, 1.14 |
115, 136, 161 |
NR |
|
Treadmill |
|||||||||
|
Askim et al., 2013 (45) |
Warm up: 10 min Start: Fastest preferred walking speed Increase: inclination 2–3%/min Termination: exhaustion, oxygen uptake level out or RER ≥ 1.1 |
NR |
NR |
NR |
1 fall |
28.7 (3.8) |
1.09 (0.07) |
149.4 (15.3) |
NR |
|
Dobrovolny et al., 2003 (48) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min Termination: Patient request, gait instability ACSM guidelines |
VO2peak RC: 0.92 RER RC: 0.72 HRpeak RC: 0.87 |
(1) RER > 1.1 (2) Reaching APMHR |
RER>1.1 and APMHR: 9% |
NR |
14.6 (4.1) |
0.96 (0.09) |
124 (18) |
176 (26) |
|
Table II. Contd. |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Gjellesvik et al., 2012 (64) |
Start: 3% inclination at 0.83 m/s Increase: 1% speed and 1% incline/min Termination: volitional fatigue |
NR |
(1) VO2 plateau (2) RER ≥ 1.05 (3) Lactate ≥ 7.0 mmol/l (4) Borg RPE ≥ 15 |
NR |
No adverse events |
30.1 (3.2) |
1.09 (0.04) |
1 72 (20) |
NR |
|
Globas et al., 2012 (65) |
Protocol: Modified Balke Start: Constant treadmill velocity adjusted to 60%–70% of CWS in 10 m test Increase: incline 2%/2 min Termination: patient request, gait instability, AHA guidelines |
VO2peak RC: 0.92 RER RC: 0.72 HRpeak RC: 0.87 (Dobrovolny, 2003) |
NR |
NR |
NR |
I: 18.9 (4.6) (n = 18) C: 21.7 (7.8) (n = 18) |
NR |
NR |
NR |
|
Hill et al., 2012 (18) |
Start: 3 km/h or 2.7 km/h at 3% incline, Increase: in speed and incline whenever VO2 stabilizes until exhaustion |
NR |
NR |
NR |
One TIA (unclear if during testing) no other adverse events Non-completion n = 1 |
31.4 (4.6) |
NR |
170 (29) |
NR |
|
Ivey et al., 2010 (66) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
NR |
NR |
NR |
No adverse events |
(1) 14.1 (4.0) (2) 13.5 (3.6) |
NR |
NR |
NR |
|
Kim et al., 2013(46) |
Protocol: Macko 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
NR |
NR |
NR |
NR |
19.7 |
0.98 (0.08) |
133.2 (23.3) |
SPB: 176.1 (32.8) DBP: 83.2 (17.2) |
|
Lee et al., 2013 (67) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
NR |
NR |
NR |
NR |
I: 16.00 (2.79) C: 20.08 (5.79) |
I: 0.67 (0.15) C: 0.98 (0.12) |
I: 128.50 (25.82) C: 143.38 (28.08) |
SBP: I: 177.75 (18.24) C: 173.13 (34.01) DBP: I: 79.63 (16.62) C: 80.75 (19.52) |
|
Luft et al., 2008 (68) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
NR |
NR |
NR |
NR |
I: 12.9, range 11.5–14.3 C: 12.9, range 11.5–14.4 |
NR |
NR |
NR |
|
Macko et al., 2001 (69) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min Termination: Patient request, gait instability, ACSM guidelines |
NR |
NR |
NR |
NR |
15.2 (3.0) |
NR |
NR |
NR |
|
Macko et al., 2005 (70) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
NR |
NR |
NR |
No adverse events |
I: 14.9 (0.9) (n = 32) C: 14.7 (1.0) (n = 29) |
NR |
NR |
NR |
|
Michael et al. 2005 (71) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min Termination: volitional fatigue |
NR |
NR |
NR |
Non-completion n = 2 |
11.7 (2.8) |
NR |
NR |
NR |
|
Michael et al., 2009 (26) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2min, 4% for 2 min, thereafter 2%/min Termination: volitional fatigue |
NR |
NR |
NR |
NR |
15.3 (4.1) |
NR |
NR |
NR |
|
Michael et al., 2006 (72) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min |
RC VO2peak: 0.92 RER: 0.72 HRpeak: 0.87 (Dobrovolny, 2003) |
NR |
NR |
NR |
11.46 (2.87) (n = 48) |
NR |
NR |
NR |
|
Ovando et al., 2011 (73) |
Protocol according to MacKay-Lyons, 2002 Start 70% of CWS Increase: until 40% above maximum walking speed, inclination 10%, Termination: patient’s request, unstable walking, ECG abnormalities |
NR |
NR |
> 95% APMR: n = 2 (25%) > 75% APMHR: n = 6 (75%) RER > 1.00: n = 3 (37.5%) |
NR |
20.60 (5.70) |
0.96 (0.07) |
%APMRH: 78.24 (13.30) |
SBP: 160 DBP: 70 |
|
Table II. Contd. |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Patterson et al., 2007 (74) |
Macko, 1997/ Michael, 2005 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min Termination: fatigue gait instability ACSM guidelines |
NR |
NR |
NR |
NR |
13.1 (4.0) |
NR |
NR |
NR |
|
Stookey et al., 2012 (75) |
Protocol: Macko, 1997 Start: Self-selected walking speed after tolerance test Increase: Incline 0% 2 min, 4% for 2 min, thereafter 2%/min Modified: incline 0% 2 min, 2% for 2 min, thereafter 2%/min Termination: volitional fatigue |
NR |
NR |
NR |
Non-completion n = 3 |
17.4 (5.4) |
NR |
NR |
NR |
|
Yang et al., 2007 (76) |
Start: 0.5 mph for 2 min Increase: 1 mph and 3.5% incline/2 min Termination: volitional fatigue ACSM guidelines |
NR |
NR |
NR |
NR |
11.24 (2.42) |
110.27 (14.56) |
NR |
SBP: 164.67 (16.76) DBP: 96.58 (8.98) |
|
Arm ergometrie |
|||||||||
|
Sutbeyaz et al., 2009 (34) |
Start: 3 min, 25W Increase: every 3 min 50 rpm Termination: volitional fatigue |
NR |
NR |
NR |
NR |
1: 12.42 (0.91) 2: VO2peak: 13.19 (1.31) C: 12.4 (0.86) |
1: 133.8 (4.84) 2: 134.4 (6.42) C: 133.8 (4.84) |
NR |
NR |
|
Bicycle recumbent semi |
|||||||||
|
Brooks et al., 2008 (63) |
Protocol based on Tang, 2006 Warm up: 2 min, 10 W Increase: 5 W/min 50 rpm Termination: ACSM guidelines, < 50 rpm |
ICC VO2peak: 0.50 RER: 0.58 HRpeak: 0.74 (Tang 2006) |
(1) plateau VO2 (2) RER > 1.0 (3) HR < 10 bpm of the APMHR |
RER > 1.0: 47 |
NR |
11.1 (3.1) |
1.0 (0.18) |
107 (23) |
NR |
|
Chang et al., 2012 (77) |
Protocol based on Tang, 2006 Start: 2 min, 10 W Increase 5 W/min 50 rpm Termination: ACSM guidelines, patient’s request |
NR |
(1) RER > 1.0 (2) APMHR of 85% (3) VO2 plateau |
NR |
NR |
I: 15.7 (5.6) (n = 20): C: 14.1 (4.8) (n = 17): |
I: 1.04 (0.05) C:1.02 (0.04) |
I: 123 (11) bpm C: 120 (15) |
I: SBP: 156 (10) DBP: 87 (11) C: SBP: 159 (10) DBP: 88 (11) |
|
Jakovljevic et al., 2012 (21) |
Start: 2 min, 20 W Increase: 10 W/min Termination: volitional exhaustion |
NR |
(1) VO2 plateau (2) RER > 1.05, (3) inability to continue |
NR |
No adverse events |
18.4 (4.6) |
1.10 (0.10) |
87% APMHR |
NR |
|
Kelly et al., 2003 (12) |
Start: 0 W Increase: 10 W/min 50 rpm Termination: ACSM guidelines, direction of the attending medical staff. |
NR |
NR |
Within 2 SDs of the mean cardiorespiratory fitness of their respective age-matched normative group: n = 4 Within 1 SD of age-matched group’s fitness: n = 1 |
NR |
Median: 1.09 (IQR: 0.85–1.48) |
Median: 0.90 (IQR: 0.80–0.99) |
Median 80% APMRH (IQR: 70–82) |
NR |
|
Koopman et al., 2013 (78) |
Start: 0 W, 2 min Increase: variable W/min per 8–12 min Termination: < 60–70 rpm, patient request |
NR |
NR |
NR |
NR |
19.0 (8.2) |
1.19 (0.05) |
135.6 (16.8) |
NR |
|
Olivier et al., 2013 (55) |
Start: 0 W, 1 min Increase: 10 W/min 60 rpm Termination: ACSM guidelines, < 60 rpm |
ICC VO2peak: 0.94 HRpeak: 0.81 |
NR |
NR |
No adverse events |
16.44 (6.94) |
NR |
128 (20.8) |
NR |
|
Salbach et al., 2013 (19) |
Start: 0 W, 3 min Increase: 5, 10 or 15 W/min Termination: unable to keep up required pedalling rate |
NR |
NR |
NR |
NR |
13.8 (3.3) |
1.1 (0.1) |
98.3 (17.1) |
NR |
|
Tang et al., 2006 (39) |
Start: 2 min, 10 W Increase 5 W/min 50 rpm Termination: ACSM guidelines, < 50 rpm |
ICC VO2peak: 0.50 RER: 0.58 HRpeak: 0.74 n = 20 |
(1) plateau VO2 based on ACSM formula (2) RER > 1.0 (3) HRpeak < 10 bpm of APMHR |
Plateau VO2: 34% RER > 1.0: 44% HRpeak within 10 bpm of APMHR: 9% |
Non-completion n = 6 |
10.7 (SE = 0.38) n = 34 |
1.00 (SE = 0.02) |
105.3 (SE = 3.9) |
NR |
|
Tomczak et al., 2008 (27) |
Protocol Manns Start: 15 W/min. Increase: 10 W/min 50–60 rpm Termination: volitional fatigue, < 50 rpm, signs of exertional intolerance |
NR |
NR |
NR |
NR |
16.0 (1.2) |
NR |
NR |
NR |
|
Table II. Contd. |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Recumbent stepper total |
|||||||||
|
Billinger et al., 2012 (30) |
Protocol Billinger, 2008 25 W, 40 W, 55 W, 70 W, 85 W, 100 W, 115 W, 130 W/2 min 80 steps/min 2 additional stages (145 W and 160 W) |
r (bicycle ergometer) VO2 peak: 0.94 HRpeak: 0.89 (Billinger, 2008) |
NR |
NR |
NR |
15.8 (3.9) n = 9 |
1.1 (0.1) |
142.9 (18.0) |
NR |
|
Billinger et al., 2010 (29) |
Protocol Billinger, 2008 25 W, 40 W, 55 W, 70 W, 85 W, 100 W, 115 W, 130 W/2 min 80 steps/min Termination: volitional fatigue, VO2 plateau or decrease, unable to maintain stepping rate, RER >1.10 |
r (bicycle ergometer) VO2 peak: 0.94 HRpeak: 0.89 (Billinger, 2008) |
NR |
90% of APMHR (220-age): 67% |
NR |
19.3 (6.9) |
1.1 (0.10) |
136.5 (21.9) |
NR |
|
Tseng et al., 2010 (31) |
Protocol: Billinger, 2008 25 W, 40 W, 55 W, 70 W, 85 W, 100 W, 115 W, 130 W/2 min 80 steps/min Termination: volitional fatigue, VO2 plateau, unable to keep cadence, adverse cardiovascular response |
r (bicycle ergometer) VO2 peak: 0.94 HRpeak: 0.89 (Billinger, 2008) |
NR |
NR |
No adverse events |
16.2 (6.5) |
NR |
NR |
NR |
|
Bicycle upright |
|||||||||
|
Baert et al., 2012 (79) |
Start: 10 W, Increase: 10 W/min 50–60 rpm Termination: ACSM guidelines |
NR |
NR |
RER ≥ 1.1: 25% |
Non-completion n = 8 |
18.1 (6.2) |
1.02 |
NR |
NR |
|
Carvalho et al., 2008 (41) |
One-legged Protocol Sunnerhagen, 2005 Start: 0 W, 3 min Increase: 10 W/min 60 rpm Termination: ACSM guidelines |
r (paretic leg) Peak isometric strength: 0.43 Peak isokinetic strength: 0.61 (Sunnerhagen, 2005) |
NR |
NR |
NR |
n = 30 paretic leg 10.7 (5.5) n = 34 Non-paretic leg 11.6 (6.5) |
NR |
119 (28) 121 (32) |
SBP: 164 (26) SBP: 166 (26) |
|
Chen et al., 2013 (80) |
Protocol Arena 2007: Start: Rest 4 min, 0 W, 4 min 60 rpm Increase: ramp 60 rpm Termination: ACSM guidelines, < 50 rpm, voluntary exhaustion |
NR |
NR |
NR |
Unable to start test: n = 5 |
12.7 |
NR |
NR |
NR |
|
Chen et al., 2010 (23) |
Protocol Zhang, 1991: Increase: 5 W/min 60 rpm Termination: ACSM guidelines, voluntary exhaustion < 50 rpm, abnormal BP responses |
NR |
(1)increase of VO2 of < 150 ml in final min of exercise (2) RER > 1.0 (3) HR peak < 15 bpm APMHR (220–age) |
RER>1.0: n = 15 HRpeak: n = 2 RER > 1.0 and HRpeak: n = 2: VO2max criteria: n = 0 |
No adverse events Non-completion n = 0 |
11.8 (0.8) |
1.1 (0.1) |
170.7 (5.3) % APMHR: 67.9 (3.4) |
SBP: 164 (26) DBP: 98 (10) |
|
Courbon et al., 2006 (81) |
Increase: 10 W/min 60 rpm Astrand guidelines |
NR |
Astrand guidelines |
NR |
NR |
17.98 |
NR |
135.43 (19.62) |
NR |
|
Eng et al., 2004 (14) |
Start: 0 W Increase: 20 W/min 50–70 rpm Termination: ACSM guidelines, ST-segment depression more than 2 mm, increasing nervous system symptoms (e.g. ataxia dizziness), sustained ventricular tachycardia, chest discomfort |
ICC VO2max: 0.93 SEM VO2max: 1.0 |
(1) RER ≥ 1.15 (2) failure to increase heart rate with increasing exercise intensity, (3) VO2 plateau (< 1.5 ml/kg/min) (4) volitional fatigue |
All subjects achieved maximum effort during the symptom-limited exercise test as defined by the ASCM criteria. Mean of 95% of APMHR: 100% HR within 10% of APMHR: 92% |
NR |
17.2 (3.0) |
NR |
94.7% (14.8) APMHR |
SBP: 174.9 (19.0) DBP: 83.1 (8.3) |
|
Fujitani et al., 1999 (24) |
Start: 10 W, Increase: 1 W/4 s Termination: subject complaining of discomfort, unable to maintain the pedalling rate, SBP > 200 mmHg, arrhythmia or ischaemic signs on ECG |
NR |
NR |
NR |
NR |
17.7 (4.2) |
NR |
124.6 (20.6) |
NR |
|
Janssen et al., 2008 (51) |
Preferred cadence, increase every 2 min Termination: unable to maintain cadence because of exhaustion |
NR |
NR |
NR |
NR |
(1) 1.0 (0.3) l/min (2) 1.0 (0.3) l/min |
NR |
NR |
NR |
|
Jin et al., 2013 (17) |
Protocol Jin, 2012: Start: 10–20 W Increase: 20 W/2 min 55–60 rpm Termination: fatigue, dyspnoea |
NR |
NR |
NR |
Non-completion n = 2 |
I: 13.2 (0.9) C: 13.2 (1.0) |
NR |
I: 127.0 (19.1) C: 128.4 (19.3) |
I: SBP: 162.1 (26.1) DBP: 75.8 (11.2) C: SBP: 165.6 (31.4) DBP: 82.0 (11.3) |
|
Table II. Contd. |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Katho et al., 2002 (82) |
Start: 20 W for 3 min, Increase: 10 W/min |
NR |
NR |
NR |
NR |
16.6 (4.8) |
NR |
NR |
NR |
|
Lee et al., 2008 (83) |
Protocol: Kelly, 2003 Termination: plateau oxygen uptake during effort |
NR |
NR |
NR |
No serious adverse events |
14.4 (3.1) |
NR |
133 (14) |
NR |
|
Letombe et al., 2010 (40) |
One-legged Start: 30 W Increase: 10 W/2 min Termination: cardiac risk factors on ECG |
NR |
NR |
NR |
NR |
I: 11.13 (4.60) |
NR |
NR |
NR |
|
Murakami et al., 2002 (84) |
Start: 20 W for 3 min Increase: 10 W/min Termination: patient’s maximum effort |
NR |
NR |
NR |
NR |
16.3 (4.4) |
NR |
NR |
NR |
|
Pang et al., 2005 (47) |
Start: 20 W Increase: 20 W/min 60 rpm Severe patients: Start: 10 W Increase 10 W/min 60 rpm Termination: ACSM guidelines |
NR |
(1) RER > 1.0 (2) a plateau in VO2 (< 150 ml/ min) (3) volitional fatigue (decline in cycling rate < 30 rpm) |
100% |
NR |
22.0 (4.8) |
1.12 (0.12) |
91.8% |
NR |
|
Potempa et al., 1995 (85) |
Start: 10 W Increase: 10 W/min Termination: ACSM guidelines |
ICC VO2max: 0.94 HRmax: 0.97 SBP: 0.83 DBP: 0.72 n = 25 (Potempa, 1995) |
(1) voluntary exhaustion (subjects could no longer continue pedalling) (2) RER > 1.15. |
NR |
NR |
(1) 16.6 (1.0) (2) 15.1 (1.0) |
(1) 1.22 (0.03) (2) 1.18 (0.02) |
(1) 142.2 (5.3) (2) 127.5 (5.5) |
NR |
|
Rimmer et al., 2009 (42) |
Start: 20 W Increase: 10 W/min 60 rpm Termination: abnormal BP or ECG RER ≥ 1.1, HRpeak within 10 bpm of APMHR, < 50 rpm |
NR |
NR |
NR |
Adverse events n = 4 |
13.0 (4.9) |
NR |
NR |
NR |
|
Rimmer et al., 2000 (43) |
Start: 20 W Increase 10 W/min 60 rpm Termination: abnormal BP or ECG RER ≥ 1.1, HRpeak within 10 bpm of APMHR, < 50 rpm |
NR |
NR |
NR |
Adverse events n = 2 |
(1) 13.34 (4.22) (2) 14.13 (2.96) |
(1) 1.06 (0.13) (2) 1.01 (0.12) |
NR |
NR |
|
Severinsen et al., 2011 (86) |
Protocol Tang 2006 Start: 2 min, 10 W Increase: 5 W/min 50 rpm Protocol Kelly, 2003: Start: 2 min, 10 W Increase: 10 W/min 50 rpm |
ICC VO2peak: 0.50 RER: 0.58 HRpeak: 0.74 (Tang, 2006) |
NR |
NR |
NR |
16.3 (4.9) |
NR |
NR |
NR |
|
Stibrant Sunnerhagen, 2007 (25) |
One-legged Start: 0 W for 3 min Increase: 10 W/min (stepless) 60 rpm |
NR |
NR |
NR |
NR |
Paretic leg: 12.4 (4.7) VO2/kg Nonparetic leg: 13.9 (4.3) VO2/kg |
0.95 (0.11) 0.98 (0.11) |
NR |
NR |
|
Tang et al., 2013 (87) |
Protocol Pang, 2005 Increase: 10–15 W/min Termination: ACSM guidelines |
NR |
NR |
NR |
NR |
17.8 (6.3) |
NR |
NR |
NR |
|
Teixeira da Cunha Filho et al., 2001 (22) |
Start: 0 W, Increase: 25 W/2 min Termination: Volitional fatigue, RER>1.0, HR within 10 bpm of the APMHR, clinical judgement |
ICC V̇O2max: 0.94 HRmax: 0.97 SBP: 0.83 DBP: 0.72 n = 25 (Potempa, 1995) |
NR |
NR |
No major ECG abnormalities |
I: 8.02 (2.05) (n = 6) C: 8.57 (2.09) (n = 6) |
NR |
I: 98.67 (12.08) C: 106.00 (20.40) |
I: SBP: 172.43 (24.99) DBP: 99.71 (16.95) C: SBP: 180.00 (24.49) DBP: 93.33 (7.55) |
|
Tseng & Kluding , 2009 (88) |
Protocol Yates, 2004 Start: 0 W, 3 min Increase: 10 W/min 50 rpm Termination: Signs of angina, dyspnoea, < 40 rpm, hyper/hypotension, ECG abnormalities |
NR |
(1) reaching 90% of APMHR (220–age) (2) RER > 1.1 |
HR or RER: 33% (n = 3) |
NR |
12.91 (3.70) |
NR |
NR |
NR |
|
Yates et al., 2004 (44) |
Protocol Potempa, 1995 Start: Sitting 2 min, thereafter 0 W Increase: 10 W/min 60 rpm Termination: 90% of APMHR, signs of angina, dyspnoea, voluntary exhaustion, < 40 rpm, hyper/hypotension, ECG abnormalities |
ICC VO2peak: 0.98 HRmax: 0.88 %HRmax: 0.85 n = 9 (Duncan 2003) |
(1) reaching 90% of APMHR (220–age) |
90% of APMHR: n = 24 |
Adverse events: n = 3 Non-completion n = 14 |
11.4 (3.7) |
NR |
116 (19) %APMHR: 77 (14) |
NR |
|
Table II. Contd. |
|||||||||
|
Study |
Protocol (including termination guidelines) |
Described reliability/validity statistics for protocol |
Criteria for reaching VO2peak |
Criteria met |
Adverse events Non-completion |
Mean VO2 peak values (SD)* (ml/kg/min) |
Mean RERpeak (SD)* |
Mean HRpeak (SD)* (bpm) |
Mean BPpeak (SD)* (mmHg) SBP (SD)* (mmHg) DBP (SD)* (mmHg) |
|
Mixed |
|||||||||
|
Billinger et al., 2008 (28) |
Protocol Yates, 2004 Bicycle ergometer Start: 0 W, 3 min Increase: 10 W/min 60 rpm Protocol Billinger, 2008 Modified total body recumbent stepper 25 W, 40 W, 55 W, 70 W, 85 W, 100 W, 115 W, 130 W; 2 min 80 steps/min Termination: volitional fatigue VO2 peak plateau or decrease <55 rpm, adverse cardiovascular event or response |
NR |
NR |
90% of APMHR 1) 63% 2) 27% |
Adverse event n = 1 |
(1) 15.4 (4.5) (2) 16.6 (4.9) |
(1) 1.1 (0.1) (2) 1.1 (0.1) |
1) 130.7 (19.2) 2) 132.9 (21.0) |
SBP (1) 139 (15.0) (2) 144 (19.8) DBP (1) 79.0 (13.0) (2) 78 (6.7) |
|
Marzolini et al., 2012 (33) |
Recumbent or upright bicycle ergometer Increase: 8.3 or 16.7 W/min 60 rpm Treadmill Protocol not reported Termination: peak volitional effort (i.e. if patient unable to maintain the required pedalling rate), appearance of adverse clinical signs or symptoms as described in ACSM guidelines, or patient achieving VO2max |
NR |
One of the following: (1) VO2 plateau (increase < 2.1 ml/kg/min, 60 s) and RER ≥ 1.15 (2) RER ≥ 1.15 and HR peak < 10 bpm APMHR (220–age or 164–0.7 age) |
18% achieved at least one criterion 36% achieved > 85% APMHR |
No serious cardiovascular events |
15.1 (4.6) VO2peak% age and sex pred: 63.1 (25.7) |
1.08 (0.14) |
%APMHR: 79.7 (15.8) |
NR |
|
Tang et al., 2010 (32) |
Protocol Tang, 2009 Upright (n = 6), recumbent (n = 3), semi-recumbent (n = 33) bicycle Increase: 5, 10 or 15 W/min Treadmill (n = 1) Bruce protocol |
NR |
NR |
NR |
NR |
13.6 (4.1) (n = 32) |
NR |
NR |
NR |
|
*Mean unless otherwise stated. n: number; W: Watt; RER: respiratory exchange ratio; HR: heart rate; APMHR: age predicted maximum heart rate; CWS: comfortable walking speed; ACSM: American College of Sports Medicine; AHA: American Heart Association; ICC: intraclass correlation coefficient; RC: reliability coefficient; r: correlation coefficient; CT: clinical trial; NR: not reported; SBP: systolic blood pressure; DBP: diastolic blood pressure; pred.: predicted. |
|||||||||
Patient characteristics
Based on 60 articles, a total of 2,104 patients were included in the analysis. The number of participants included in a study ranged from 3 (16) to 128 (17). Mean age ranged from 46 (18) to 71 (19) years. Most studies included more men than women, but 6 studies included only men (20–25). The mean time since stroke onset ranged from 9 days (23) to 7.5 years (26, 27). Approximately half of the studies described the use of beta-blockers, which varied between 0% (16) and 82% (28) of the patient sample.
Study characteristics
Test procedures; equipment and protocols. Of the 60 included studies, 21 used a treadmill with (n = 3) or without (n = 18) body-weight support to conduct the tests. In 33 studies, patients completed the test on an upright, semi-recumbent or recumbent bicycle ergometer. Three studies used a stepper (29–31). Two studies (32, 33) used a semi-recumbent bicycle, an upright bicycle and a treadmill, and one study used a bicycle ergometer and a stepper (28). One study used an arm-crank ergometer (34).
A number of different test protocols were used. Eight different test protocols were described for the 21 studies using a treadmill. Most of the included studies (n = 11) used the constant-velocity graded treadmill protocol described by Macko et al. (35). This protocol involves starting at a self-selected gait speed and increasing the treadmill incline by 2.5% every 2 min to 10%, after which gait speed is increased. The other studies described protocols in which activity was graded by increasing inclination and gait speed. Two studies using body-weight support (36, 37) used the protocol by MacKay Lyons & Makrides (38), which resembles that of Macko, increasing incline by 2.5% every 2 min up to 10%, followed by a 0.05m/s increase in gait speed every 2 min.
Of the 36 studies using a bicycle, the majority used a ramp protocol with a step duration up to 60 s, although different step increments were used. Most studies (n = 15) used steps of 10 W/min. Five studies used steps of 5 W/min, as recommended in the protocol by Tang et al. (39). The smallest steps were described in the study by Fujitani et al. (24) who used 4 W/s. The largest step was 16.7 W/min in the study by Marzolini et al. (33). Several studies used steps of longer duration, and different incremental steps, depending on the patient or on the total amount of exercise time, or they did not specify the steps. In most studies, patients were instructed to keep up a certain target cadence, varying between 50 and 70 revolutions/min. Three studies used a 1-legged protocol (25, 40, 41) and one of these studies explicitly described that the increase in resistance was stepless (25).
Adherence to recommendations. Pre-testing procedures were reported by almost half of the studies (n = 26). Pre-test screening was usually performed by a physician.
There are 2 reasons to terminate a CPET: to prevent adverse events when a patient becomes symptomatic, and when the patient has reached maximum effort. Fifteen studies did not explicitly report criteria for test termination. Symptom-limited test termination criteria were reported by 19 studies, which referred to the criteria described by the American College of Sports Medicine (ACSM) guidelines (1) and one that referred to the guidelines of the American Heart Association (5). Twenty-seven studies explicitly reported volitional exhaustion or patient request as termination criteria, indicating that maximal effort had been reached. In addition, gait instability (treadmill) or inability to continue a predefined level of revolutions/steps per min is mentioned in 18 studies as a test termination criterion.
Safety. Of the 23 studies (n = 876) that included information about clinical signs and symptoms during CPET, 18 reported no clinical abnormalities. Five studies (28, 42–45) reported 1 or more (maximum 4) clinically relevant abnormalities in 11 patients (1%). One study reported 4 patients with coronary changes. These patients were excluded and referred to their physician (42). One study reported 3 patients with cardiac problems (44) and one study reported terminating CPET in a patient with an ST segment elevation of more than 1 mm (28), in accordance with ACSM criteria. Another study reported 2 patients with cardiovascular problems during exercise testing, for which they received medical care and were discharged. However, both events took place during different exercise tests than the one included in our analysis (43). One study reported one fall, but no injury occurred (45). One study reported a patient with a transient ischaemic attack, but it is unclear if this event took place during CPET, and training was resumed within 4 days without further problems (18).
Peak oxygen uptake. VO2peak was calculated using different methods. Some studies included the highest value; others reported the mean value of the last 30-s stage.
Sixteen studies (40%) described criteria for reaching VO2max. Different criteria were used, including a plateau in VO2 despite an increase in workload (n = 15), RER above a certain level (> 1.00–1.15) (n = 15) and APMHR (n = 12). Two studies reported systolic BP above a certain level (> 190 mmHg) as a criterion for reaching VO2peak (36, 46). However, only a minority of the studies (n = 11) also reported the number of people who met the predefined criteria. The number of patients who met 1 or more of the predefined criteria ranged from 11% (23) to 100% (14, 47). The number of participants reaching a plateau in VO2 uptake was reported by 1 study (39), with 34% of the patients reaching the plateau. RER above the defined level (Table II) was reached by 9% (48) to 79% (23) of the patients. Defined criteria (Table II) related to APMHR were met by 9% (39) to 92% (14). Two other studies described the number of participants who met at least 1 out of 2 (33%) (31) or 2 out of 3 (100%) (47) criteria. All studies reported VO2peak values for all patients, regardless of whether patients satisfied the criteria for reaching VO2max.
In addition, various studies described one or more of the criteria for reaching VO2max as a criterion for test termination (n = 8), such as reaching APMHR, a percentage of APMHR or an RER value above 1.0. This means that the test was terminated as soon as a patient met 1 of the criteria, whether or not maximum effort had been reached at that moment.
A wide range of VO2peak outcomes were reported in the included studies. The lowest mean VO2peak score was 8.02 ml/kg/min, found in the control group of a study including 12 acute male stroke survivors using a cycling protocol (22). A total of 24 studies (40%) reported mean VO2peak values below 15 ml/kg/min, which is likely to negatively influence independence in older women (49). The majority of the studies reported values between 15 and 25 ml/kg/min. The highest reported VO2peak was 31.4 ml/kg/min, found in 10 young community-dwelling stroke survivors using a treadmill protocol (18). Using the reference values reported by Fairbarn et al. (50) for healthy persons, these results would indicate that the reported VO2peak values varied between approximately 20% and 70–80% of the reference values, depending on age and sex. Two studies reported VO2peak in l/min, with values of 1.0 (51) and 1.09 (12).
DISCUSSION
This review included 60 studies involving 2104 stroke survivors and describing 38 different CPET protocols to determine peak oxygen uptake. Protocols included treadmill, bicycle, step or arm ergometers, used in all phases post stroke. Although most authors refer to contemporary guidelines for exercise testing (i.e. ACSM, American Heart Association (AHA), American Thoracic Society (ATS)), the testing procedures applied in most studies did not, or insufficiently, adhere to the CPET guidelines. For example, information about safety was given in only a small number of studies. Although these reported no major adverse events, definite conclusions about safety cannot be drawn yet. A variety of criteria were used to determine maximal effort, and little information was provided about the number of patients who met the predefined criteria for maximum oxygen uptake.
Test procedures: equipment and protocols
Treadmill and bicycle ergometry were the most frequently used modalities. Studies using a treadmill applied stricter inclusion criteria concerning walking ability (e.g. Functional Ambulation Categories (FAC) > 8,963). However, the use of body-weight support (BWS), as described in 3 studies (20, 36, 37), also made it possible to conduct a safe CPET in patients with poorer walking ability. Testing on the treadmill usually involves more muscle mass and more work against gravity, which leads to higher oxygen uptake compared with seated modalities. The highest VO2peak values are assumed to be lower when using BWS (52), but the data in the present study do not confirm this. Reported VO2peak values were higher in the BWS protocols compared with some other treadmill protocols. Although patient populations might not be comparable, the BWS protocols show RER values above 1, suggesting that the participants were able to put in maximum effort even in the acute phase after stroke. Since beta-blockers limit the maximum heart rate, which leads to diminished cardiac output and, consequently, reduced VO2max (53), the use of medications should be recorded. Unfortunately, only approximately half of the studies reported the use of beta-blockers (Table II).
The bicycle ergometer was the most commonly used modality (Table II). Using bicycle ergometry may reduce the influence of balance problems. Although maximum oxygen uptake is often higher in treadmill protocols, especially in healthy populations (1, 4, 54), seated modalities are more useful for patients with balance problems or gait instability, which are often present after stroke. Testing can be further facilitated by using a recumbent or semi-recumbent bicycle or stepper. Also, cycling involves less noise and artefacts while testing, for example in electrocardiography (ECG) and BP measurements. For patients who are not used to cycling, it might be helpful to include some practice sessions on the bicycle before the CPET, to increase the chances of achieving maximum effort. Tang et al. (32) reported a practice effect in a sample of acute stroke patients, with a difference of 10% between the test and re-test measurements, which was significantly greater than the expected 3% day-to-day variability. Dobrovolny et al. (48) conducted an acclimatization treadmill trial without open-circuit spirometry, which may have eliminated any effect of practice. Olivier et al. (55), on the other hand, reported that a practice test did not systematically affect maximum CPET results. The final choice of equipment depends on the goal of the test and the patient’s ability. When designing an exercise intervention using CPET, it is best to choose the same modality for testing and training. Arm ergometry, although potentially useful for patients with walking difficulties and balance problems, uses small muscle groups, resulting in a lower VO2peak than bicycle or treadmill protocols, and causes larger increases in BP. This is an important safety issue, especially as it is not possible to monitor BP by the standard cuff method during an exercise that primarily involves the arms.
All studies applied protocols using fixed or individualized incremental steps. When larger stage-to-stage increments in energy requirements are used in a protocol, the relationship between VO2 and work rate is usually weaker. Hence, we recommend ramp protocols with modest increases in work rate per stage, preferably completing the test in between 8 and 12 min (3, 56). The duration of the steps in ramp protocols on a bicycle usually varies between 10 and 60 s (57). Most of the included studies used protocols with steps of a maximum duration of 1 min (Table II).
For patients with balance problems, we suggest using a bicycle ergometer or treadmill with body-weight support. For patients with moderate to severe stroke, a recumbent bicycle protocol seems appropriate.
Adherence to guidelines
In a previous review, Jones et al. (15) summarized the quality of methods used in different types of exercise tests for patients with cancer. They concluded that exercise testing in clinical oncology does not always comply with national and international quality guidelines. This is in line with the results reported in reviews including healthy subjects and elderly persons (58, 59) and is also in line with the findings of the present review.
The most commonly cited guideline for exercise testing is the ACSM guideline, which describes clinical exercise testing separately. This guideline recommends pre-exercise evaluations that help to identify the risk that individuals run when undergoing an exercise test. It also describes contraindications for maximum testing. Pre-exercise testing was poorly reported in the studies included in our review. As one may expect all patients to have undergone thorough medical screening, separate pre-test screening might be less important. Without pre-screening, however, it is important that physician approval is part of the inclusion criteria. This was scarcely reported in the studies included in our review. Patients should be given clear instructions before the test, taking potential cognitive difficulties into account, since this increases the test validity and data accuracy. Patients should be instructed to abstain from activities that influence their heart rate and BP, such as eating, drinking alcohol, caffeine or tobacco, and engaging in high-intensity exercise, 2–3 h prior to the test. Most of the studies did not describe these instructions in their exercise protocols or inclusion criteria. For safety reasons, precautions should be taken when testing stroke survivors: inclusion and exclusion criteria should be clear, pre-testing should be conducted and the patient should be monitored closely during the test. More than half of the included studies, however, failed to adequately take these precautions, or failed to describe them.
Variables that should be monitored to ensure safety during the test are BP, ECG, subjective rating (rate of perceived exertion; RPE) and clinical signs and symptoms (1, 56). The small number of adverse events suggests that CPET can be conducted safely in stroke patients. However, definite conclusions cannot be drawn, since adverse events were described in only a minority of the studies. Future studies need to include more information about adverse events during and as a result of CPET.
Some studies did report on adverse or abnormal cardiovascular changes that led to early test termination according to the ACSM recommendations. Several studies used the criteria for maximum effort, e.g. RER > 1.0 or a VO2 plateau, as termination criteria. However, these cannot be used as an indication to terminate the test (3). Some studies used a percentage of the age-predicted maximum heart rate as a termination criterion, which is not in agreement with the ACSM guidelines, despite the suggestion by some authors that it is a valid termination criterion.
Reporting CPET measures
There are currently no formal guidelines for reporting exercise-test data for any clinical population (15). The following key variables for reporting have been suggested (5): peak VO2, VO2 at ventilatory threshold (VT), peak RER, ventilatory equivalent for carbon dioxide production relationship (VE/ VCO2 slope), exertional oscillatory ventilation (EOV), pressure of end-tidal carbon dioxide (PetCO2), ventilatory equivalent for oxygen (VE/VO2) at peak exercise, change in cardiac output/oxygen uptake relationship (DQ/DVO2 slope), minute ventilation relative to ventilatory capacity (VE/MVV), forced expiratory volume in 1 s (FEV1), O2 pulse trajectory, change in oxygen consumption related to change in power output (DVO2/DW) trajectory, HR, heart rate reserve (HRR) at 1 min, BP, peripheral capillary oxygen saturation (SpO2), ECG and subjective symptoms. Since reporting VO2max or VO2peak was an inclusion criterion in the present review, all included studies reported 1 of these outcomes. Limited information was provided about the used measurement system to determine these outcomes, including types and quality control of gas analysers and flow transducers.
Reported VO2 values varied widely between the studies. The values are difficult to interpret, since only a minority of the studies reported the number of patients who satisfied defined criteria for maximum oxygen uptake. The criteria for achieving maximum effort during CPET are, however, being debated, and no gold standard can be provided (10, 11, 59, 60). Levelling off of VO2 despite increase in workload, percentage of APMHR, and RER exceeding a certain level have been suggested as criteria for determining VO2max. Recently, Edvardsen et al. confirmed, in a large sample of healthy participants, that more than one plateau can be achieved during continuous graded exercise, and therefore questioned the use of levelling off as a criterion (61).
Since most patients terminate CPET before criteria for VO2max are met, it is helpful to report secondary criteria and reasons for termination in order to judge patient effort and interpret the test results. If a secondary criterion is reported at all, the most common one in the included studies is an RER cut-off value, ranging from > 1.0 to 1.15. A peak RER > 1.10 is generally considered to be an indication of the subjects’ maximum effort (3). Again, caution is needed when using this variable in the stroke population. Data from healthy persons suggest that RER values are age-dependent. A peak RER higher than 1.0 already indicates maximum effort in persons aged over 65 years (61). As patients with stroke are often older people, an RER above 1.0 seems a reasonable criterion.
Two studies (36, 46) described systolic BP above 200 mmHg as an indication that maximum effort had been achieved. This is surprising, as BP is monitored for safety and not to judge maximum effort. It is clear that termination criteria for reasons of safety and criteria for maximum effort have been used interchangeably in the included studies.
Several studies mentioned maximum heart rate as a criterion for maximum effort, using different or unreported formulas and various percentages of APMHR. The use of maximum heart rate to determine maximum effort has been questioned by Cumming & Borysyk (62). They concluded more than 20 years ago that the maximum heart rate range was too wide to use a mean maximum value alone as a criterion for VO2max. The standard deviation associated with the estimate is approximately ± 11 beats/min, making it a difficult “standard” to justify (11). In addition, maximum heart rate is not a valid outcome for the stroke population, since it might be greatly influenced by the use of medication, especially beta-blockers. Therefore, maximum heart rate is not recommended for use as a valid criterion in the stroke population.
Since most patients are symptom-limited and the CPET might be terminated early, most of the defined criteria will not be met (63), and it is questionable whether the criteria defined in different guidelines are applicable to stroke survivors. We recommend reporting at least means and ranges of RER and exercise duration. In addition, the criteria and reasons for termination need to be reported, since these are necessary to interpret the test results. Also, results need to be compared with norm scores, data need to be reported for specific age groups, and values for men and women should be reported separately. Marzolini et al. (33) reported that women with a stroke were significantly less likely than men to reach more than 1 of the critical levels used to prescribe exercise. In addition, women report different non-cardiovascular reasons for discontinuing CPET and reach a significantly lower baseline VO2peak than men after stroke.
Limitations and recommendations
When interpreting the results of the present review, some limitations need to be taken into account. Despite our comprehensive and broad search strategy it is possible that some studies using CPET in stroke survivors have been missed, especially if CPET was a secondary aim. However, the conclusions are based on a large number of studies, which should be representative. A drawback of our broad inclusion strategy is that the included studies show a wide diversity of methods and populations, which makes it more difficult to draw general conclusions. In addition, some of the studies included patients who were participating in exercise intervention programmes, and therefore might not be representative of the stroke population as a whole. In the present review we could provide a limited amount of patient and stroke characteristics because of pragmatic reasons and available information. More details about, for example, comorbidities, motor impairment and functional capacity might help to interpret the conductance and performance of CPET. However, maximal exercise testing in stroke will most often be used to select or evaluate exercise interventions, making our findings useful for the intended population, since patients in all phases after stroke were included.
The findings of the present review do not enable us to state which protocol is preferable. However, since the results of CPET are not only used to assess the effects of stroke interventions, but also to develop exercise interventions, the methods of conducting and reporting CPET after stroke clearly need to be improved. Therefore we provide several suggestions to guide the conducting and reporting of maximal cardiopulmonary testing in stroke survivors (Table III). More research is needed to validate different testing modalities in the stroke population. In the present review only one study compared 2 protocols within the same population to examine the feasibility and validity of the protocol. We also recommend composing a consensus statement on how to report CPET in people after stroke comparable to, for example, CONSORT guidelines for reporting randomized trials.
|
Table III. Recommendations for conducting and reporting cardiopulmonary exercise testing (CPET) after stroke |
|
|
Reporting |
|
|
Participants Instruct the patient to refrain from ingesting food, alcohol or caffeine or using tobacco products from 3 h before testing, to avoid significant exercise on the day of the assessment, to wear loose-fitting clothes and suitable shoes, to use or stop using the medication (depending on the purpose of the test), to bring a list of medications, to drink ample fluids during 24 h preceding the test. |
Age Gender Time since stroke Severity of the stroke Use of medication Co-morbidities Patient-related risk factors to conduct CPET |
|
Safety Include pre-test screening by physical examination, according to the ACSM criteria (p. 44). Have the patient complete the Physical Activity Readiness Questionnaire or get approval from a physician. Check contraindications as described by ACSM guidelines (p. 54) During the test, monitor the following variables continuously or at the end of each stage: ECG, HR, BP, RPE and gas exchange. Clinical signs and symptoms also need to be closely monitored by the test supervisor. Have the test supervised by an experienced and trained person under supervision of a physician. Skills needed to supervise an exercise test are described by the ACSM guidelines based on the ACC and AHA guidelines (p. 122). |
Definition of serious adverse events Number of serious adverse events occurring during the CPET Nature of serious adverse events occurring during the CPET |
|
Equipment Use a proper test modality depending on the aim of the assessment and the patient’s characteristics, e.g. treadmill (with or without bodyweight support), cycle ergometer (recumbent or non-recumbent) or stepper (recumbent or non-recumbent). Bicycle ergometry is recommended since this modality is less influenced by sensorimotor deficits. When a patient is unable to pedal, the treadmill is a valid alternative. Include a test session to familiarize the patient with the equipment. Calibrate all equipment as recommended before use. |
Type of equipment used Brand (version) of the equipment used Safety and quality label |
|
Protocol Use a reliable and valid incremental test protocol. Incremental steps can be individualized or standard steps. Steps need to be small. Aim for test duration of 8–12 min. Make termination criteria clear to test supervisor and patient. Instruct the patient to exercise until exhaustion. |
Reliability and/or validity values Information about warming up/cooling down period Incremental scheme, i.e. size and duration of the incremental steps Termination criteria for safety (e.g. ACSM) Reasons for test termination Test duration (mean, range) |
|
Outcomes Record VO2, RER, BP and HR continuously during testing. Average VO2peak over the last 20–30 s, preferably during the plateau phase. Define criteria and cut-off points to determine maximum effort, such as VO2 plateau, RER ≥ 1.0, according to the population being studied. |
Absolute mean (range) VO2peak and RER values for total population and preferably divided by sex and age Criteria and cut-off points to judge maximum effort Number (percentage) of patients who met the criteria |
|
ACSM: American College of Sports Medicine; RPE: rate of perceived exertion; RER: respiratory exchange ratio; HR: heart rate; BP: blood pressure. |
|
Conclusion
The protocols described in the studies included in our review were very heterogeneous. Insufficient reporting of relevant outcome measures other than VO2peak, such as RER and VT, raises the question as to whether the results do indeed reflect maximum effort. Although authors referred to established guidelines, these were not adhered to, or were incorrectly adhered to. This means that the results of cardiopulmonary exercise testing protocols in stroke survivors cannot be compared, and raises the question as to whether stroke-specific testing and reporting guidelines are needed.
ACKNOWLEDGEMENTS
The authors would like to thank Jurgen Mollema, information expert at the University of Applied Science, Utrecht, the Netherlands, for his assistance with the literature search.
REFERENCES

