Xinyu Guan, MSc1, Yali Liu, BSc1, Lianjun Gao, MSc2, Linhong Ji, PhD1, Rencheng Wang, PhD1, Mingliang Yang, MD2 and Run Ji, BSc3
From the 1Division of Intelligent and Bio-mimetic Machinery, The State Key Laboratory of Tribology, Tsinghua University, 2Department of Spinal and Neural Function Reconstruction, China Rehabilitation Research Center and Capital Medical University School of Rehabilitation Medicine and 3Human Biomechanics Laboratory, National Research Center for Rehabilitation Technical Aids, Beijing, China
OBJECTIVE: To investigate trunk muscle activity patterns in a person with thoracic spinal cord injury when walking with different un-powered exoskeletons, and to explore how different un-powered exoskeletons affect trunk muscle activity patterns.
CASE REPORT: Data were recorded from a subject with complete spinal cord injury at T10, using an electromyography system on 4 pairs of trunk muscles and a motion capture system simultaneously.
RESULTS: The participant generated large muscle force to laterally bend and rotate trunk, and swung his leg through the moments generated, not only by trunk flexion and extension, but by trunk rotation. In an energy-stored exoskeleton without springs condition, the energy generated by erector spinae contraction was stored in the energy-stored component in the stance phase and released in the swing phase to compensate for energy generated by the obliquus externus abdominis and avoid overuse of the obliquus externus abdominis.
CONCLUSION: These findings prompt further development of un-powered exoskeletons and investigation into trunk muscle functions in patients with spinal cord injury when walking with un-powered exoskeletons.
Key words: un-powered exoskeleton; electromyography pattern; spinal cord injury; gait; trunk muscles.
J Rehabil Med 2016; 48: 00–00
Correspondence address: Linhong Ji, 3503 Room, 9003 Building, Department of Mechanical Engineering, Tsinghua University, Beijing 100084, China. E-mail: jilh@tsinghua.edu.cn
Accepted Dec 18, 2015; Epub ahead of print Mar 2, 2016
INTRODUCTION
Walking is an effective way to reduce the complications of spinal cord injury (SCI) and improve the function of both undamaged and damaged neuronal structures (1). Many un-powered exoskeletons have been developed to assist ambulation in patients with SCI. Through intersegmental reaction forces the moment generated by an individual muscle can contribute to the power of a segment to which it is not applied (2). Patients with SCI therefore ambulate in a compensatory strategy, using residual muscles to substitute for the affected muscles, with crutches or walkers (3). Patients with complete injury at the thoracic level, who have lost the ability to control their hip flexors and extensors, have to use the trunk muscles to drive their lower limbs. In this context the activity of the trunk muscles is crucial to provide the necessary power for movement of the lower limbs.
Electromyography (EMG) can reflect muscle recruitment. A combination of EMG and kinematic data synchronizes trunk muscle recruitment and gait patterns. This combination is an objective method of analysing trunk muscle activity patterns, and may improve our understanding of trunk muscle function in patients with SCI when walking with un-powered exoskeletons. This study investigated the relationship between trunk muscle activity and corresponding gait kinematics, as well as the effects of different un-powered exoskeletons on trunk muscle activity patterns in a patient with thoracic SCI.
CASE REPORT
The study participant was a 29-year-old man (height 1.72 m, weight 62 kg), who was injured 2 years prior to the study and diagnosed with SCI at the T10 level. The injury was clinically classified as complete (“A” according to the American Spinal Injury Association (ASIA) Impairment Scale). He had strong upper limb muscles and good trunk control ability. In daily life he moved around outdoors using a manual wheelchair and indoors using bilateral knee-ankle-foot orthoses (KAFO). Before the experiment the participant had used a bilateral KAFO for 1 year, and had been trained to walk with an isocentric reciprocating gait orthosis (IRGO), energy-stored exoskeleton without springs (ES-EXO (w)), and energy-stored exoskeleton (ES-EXO), respectively, for 2 months. He performed two 20–30-min gait-training sessions daily by walking back and forth in a 30-m corridor, using a walker to maintain balance. Study approval was granted by the Institutional Review Board and the ethics committee.
Brief descriptions of tested un-powered exoskeletons
The KAFO consists of a polypropylene thigh and shank shell with a lock at the knee joint. The IRGO consists of a bilateral KAFO connected by a fixed hip band and a rocking pelvic band that functions as a lever to achieve reciprocal gait. The ES-EXO (Fig. 1a) was developed by Tsinghua University, consisting of bilateral KAFO and 2 energy-stored components connected by soft straps. Each energy-stored component (Fig. 1b) has an inverted triangular pelvis bracket and 2 tensile springs. Each end of the springs can correspondingly slide along the upper edge, the hypotenuse, the thigh bar and the hip joint bar to adjust the initial forces (upright posture) and the force arms between the spring and the hip joint. The parameters of springs 1 and 2 in this case study are shown in Table I. Both spring 1 and spring 2 were tensile in the upright posture. The hip joint produces significant negative power in a gait cycle from mid stance to terminal stance, as the muscles control the body’s forward movement against gravity (4). Springs were used to store energy during the negative power period and release it during the positive power period for hip joint flexion.
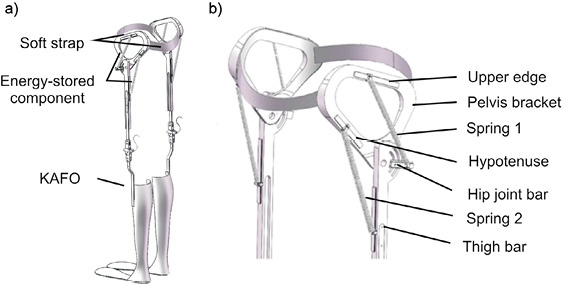
Fig. 1. Energy-stored exoskeleton (ES-EXO): (a) overall view, (b) energy-stored components, L1 and L2: initial lengths of Springs 1 and 2, respectively; A1 and A2: initial force arms of Springs 1and 2, respectively.
|
Table I. Parameters of springs 1 and 2 |
|||||
|
|
Stiffness, N/mm |
Original length, mm |
Initial length, mm |
Initial force, N |
Initial force arm, mm |
|
Spring 1 |
0.75 |
60 |
140 |
60 |
60 |
|
Spring 2 |
0.56 |
75 |
150 |
42 |
15 |
|
Initial length, initial force and initial force arm were tested when the participant stood in an upright posture. |
|||||
Experimental design
Trunk global muscles, including the bilateral rectus abdominis (RA), obliquus externus abdominis (OE), latissimus dorsi (LD) and erector spinae (ES), were measured. These muscle EMG patterns were recorded by 8-channel Telemyo DTS (Noraxon, Scottsdale, Arizona, USA), with a cut-off frequency of 1,500 Hz. The signals were sampled at 1,500 Hz and amplified 1,000 times. Pairs of silver/silver chloride (Ag/AgCl) surface electrodes (Tianrun Sunshine Medical Supplies Co., Ltd, Beijing, China) were attached to the muscle bellies after cleaning the subject’s skin with alcohol wipes. Maximal voluntary contractions (MVC) of 4–5 s were carried out against external resistance in the supine or prone position. The MVC techniques included: trunk flexion for bilateral RA, trunk flexion leftward for right OE and rightward rotation for left OE, shoulder elevation for bilateral LD, and trunk extension for bilateral ES (5). Each MVC test was repeated 3 times and the maximum value was recorded.
The participant was tested in 4 conditions in the same experimental session: KAFO, IRGO, ES-EXO (w) and ES-EXO. In each condition, the participant was asked to walk along a 6-m walk-way with the exoskeleton at a comfortable speed, maintaining balance using a walker. Whole-body motion was recorded using a VICON motion capture and analysis system (Oxford Metrics Ltd, Oxford, UK) with 8 digital cameras. VICON and Telemyo DTS were synchronized. Markers were placed on the un-powered exoskeletons for the lower limbs and on the participant for the trunk and upper limbs, according to Plug-in-Gait Marker Placement (6). Motion data were sampled at 100 Hz for 6–8 strides, on average, for each trial and 5 trials were collected for each condition. The participant rested for 2 min between 2 trials. All data were collected in the Gait and Motion Analysis Laboratory at the National Research Center Rehabilitation Technical Aids (Beijing, China).
Outcome measures
EMG analysis. Standard filtering and rectifying methods were used to process raw EMG data. A band-pass filter of 10–500 Hz was applied, and then the electrocardiogram artefacts were reduced. Next, a 60 Hz high-pass filter was used, the EMG signals rectified, and a 4 Hz low-pass filter adopted (bilateral zero-lag 4th order Butterworth). All EMG data were processed using software (MR-XP 1.07 Master Edition). The mean EMG amplitude for each muscle was calculated based on 5 trials after time normalization. Amplitude normalization (%MVC) was calculated by dividing the mean EMG amplitude by its corresponding MVC value. Integrated EMG (IEMG) in the stance and swing phases were calculated to estimate muscle effort.
Motion analysis. Motion data were filtered using a fourth-order bidirectional Butterworth low-pass filter with a cut-off frequency of 6 Hz and calculated, on average, after time normalization. The mean range of motion (ROM) of the trunk, pelvis and hip were also calculated based on 5 trials after time normalization. Fig. 2 sets out the definitions of the hip, trunk and pelvic angles.
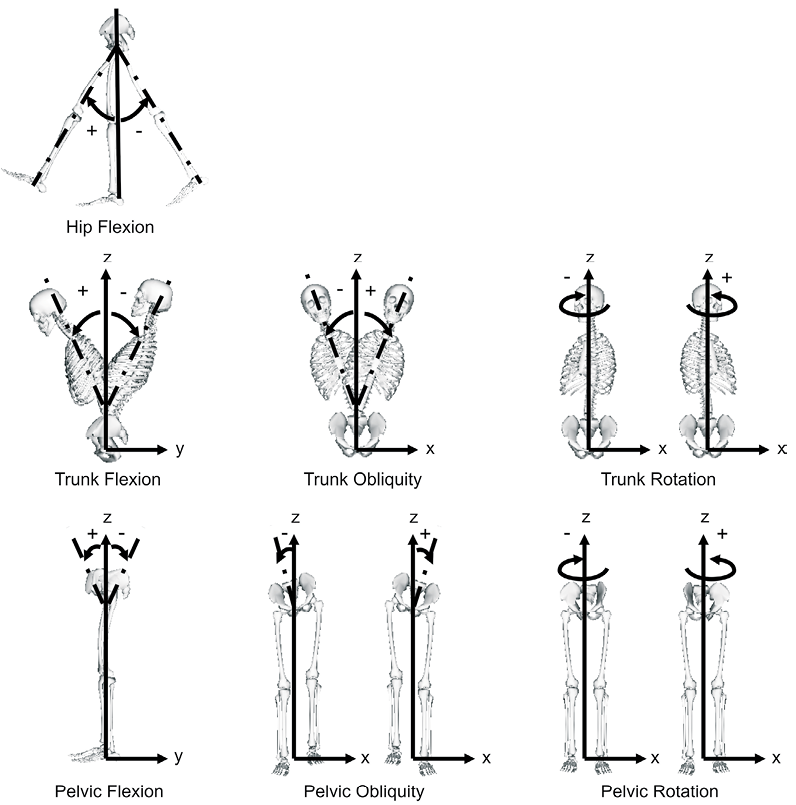
Fig. 2. Hip, trunk and pelvic angle definitions. Hip angle is the angle between the pelvis and thigh. Trunk angle is the angle between the thorax and the laboratory coordinate system. Pelvic angle is the angle between the pelvis and the laboratory coordinate system.
RESULTS
EMG measurements
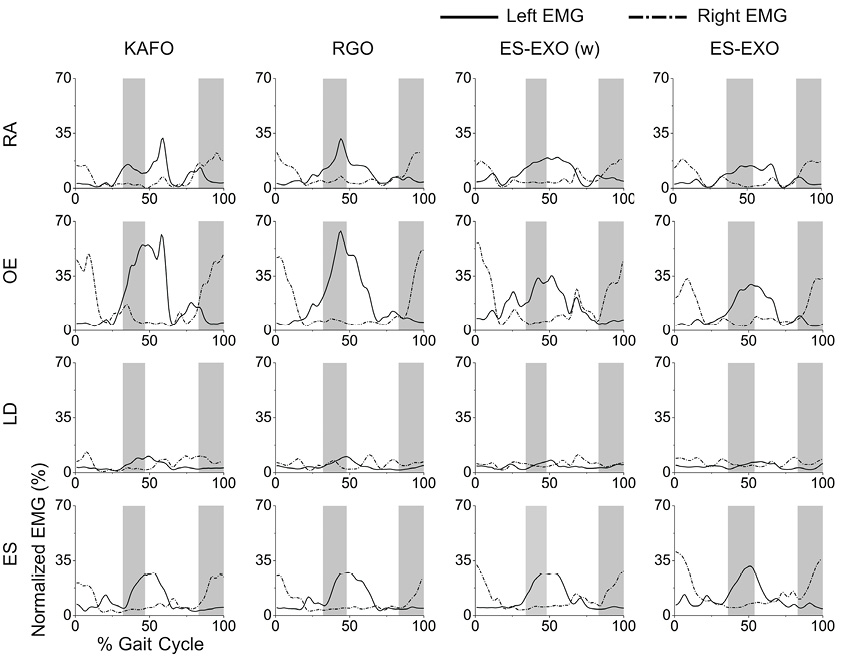
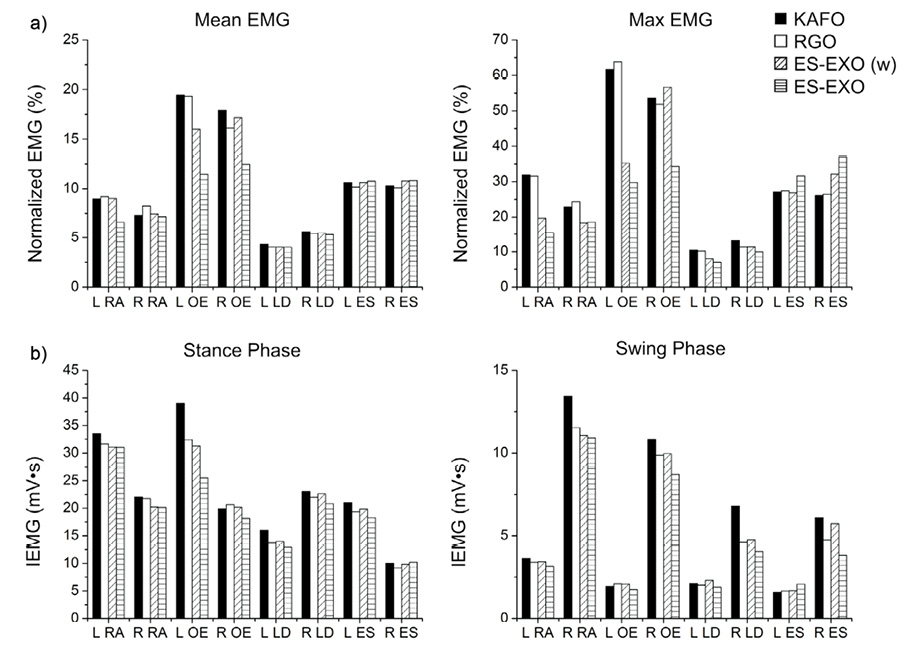
Trunk muscle activity patterns were evaluated by the linear envelope (Fig. 3). The mean and peak of the linear envelope were correlated with the average and maximum force produced by the muscle (Fig. 4a). The IEMG could be regarded as an indication of the total effort spent in the stance and swing phases (Fig. 4b).
Bilateral RA, OE, LD and ES activity patterns were similar in the 4 test conditions (Fig. 3). Bilateral RA, OE and ES activity presented obvious periodical characteristics in the gait cycle. In the single-support phase normalized EMG amplitudes of the RA, OE and ES increased on the leg-swing side, while on the leg-support side they remained stable with small fluctuations. Bilateral LD were relatively in low activities (< 20%) in a gait cycle. Additional bursts appeared in both the RA and OE waveforms close to the end of the single-support phase (heel striking) for KAFO and IRGO walking, and only in the OE waveform for ES-EXO (w) walking.
In terms of bilateral OE, the mean and maximum normalized EMG in ES-EXO walking were much smaller than in the other 3 conditions (Fig. 4a). It is worth noting that the maximum normalized EMG of bilateral ES in ES-EXO walking were the greatest among the 4 conditions, but that they were not significant (Fig. 4a, right panel). IEMG of bilateral RA in KAFO walking was greater than other conditions in the stance and swing phases, and was prominent for right RA in the swing phase (Fig. 4b). IEMG of left OE in the stance phase and right OE in the swing phase in KAFO walking were greatest among the corresponding 4 conditions (Fig. 4b). The IEMG of the left ES in the swing phase in ES-EXO walking was a little greater than in other conditions (Fig. 4b).
Kinematic parameters
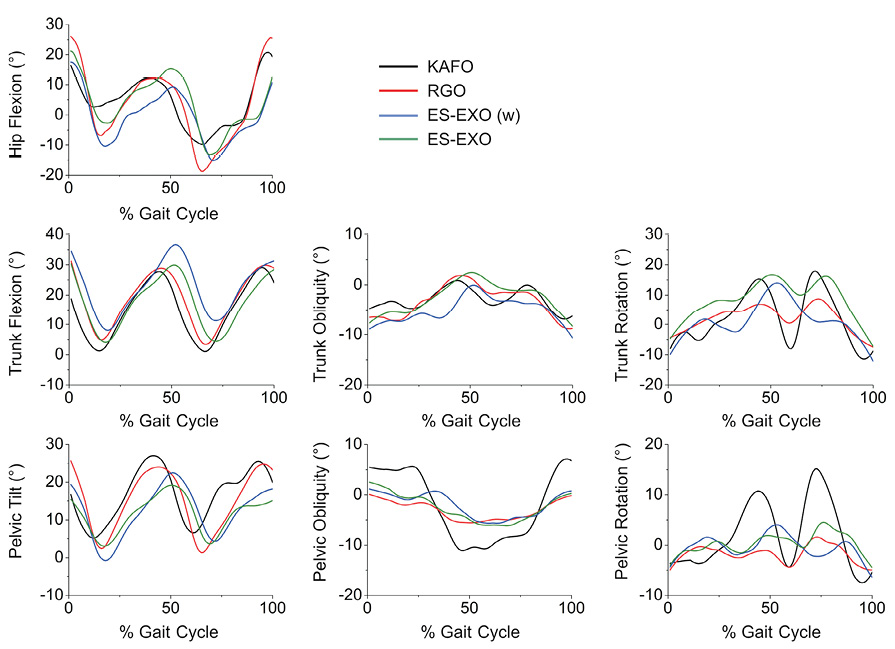
Analysis of kinematic performance was performed by comparing the temporal spatial data (Table II), as well as the ROM for the pelvis and trunk in 3 dimensions and the hip joint in the sagittal plane (Fig. 5).
|
Table II. Temporal spatial data |
||||
|
Un-powered exoskeleton |
Step length, m |
Walking speed, m/s |
Stride duration, s |
Swing duration, s |
|
KAFO |
0.17 |
0.10 |
4.11 |
0.60 |
|
IRGO |
0.12 |
0.06 |
4.91 |
0.75 |
|
ES-EXO (w) |
0.15 |
0.09 |
4.19 |
0.63 |
|
ES-EXO |
0.18 |
0.12 |
3.50 |
0.51 |
|
KAFO: knee-ankle-foot orthosis; IRGO: isocentric reciprocating gait orthosis; ES-EXO: energy-stored exoskeleton; ES-EXO (w): energy-stored exoskeleton without springs. |
||||
The step lengths of KAFO and ES-EXO walking were comparable and larger than in the other 2 conditions. The participant walked fastest with the ES-EXO and the speed was twice with that of the IRGO. Stride and swing durations in the ES-EXO condition were significantly reduced.
The trends of averaged angular movement waveforms (Fig. 5) in the 4 conditions were similar in the hip joint in the sagittal plane, and the pelvis and trunk in the sagittal, coronal and transverse planes. However, there were differences in range of joint movement. Obliquity of the pelvis in the KAFO condition was out of the range exhibited by the other conditions. In the transverse plane, the participant rotated the trunk and pelvis in a relatively smaller range with the IRGO, and to a predominantly larger degree with the KAFO. In the sagittal plane, the range of hip and trunk motion in the IRGO condition was smaller than in a case study by Johnson et al. (a female with spina bifida at T12, hip motion ranged from 15° extension to 40° flexion) (7).
DISCUSSION
Relationship between trunk muscle activities and kinematics
This case study investigated the trunk muscle activities and kinematics of a subject with complete T10 SCI, when walking with different un-powered exoskeletons in a gait cycle. Despite substantial heterogeneities between the 4 different exoskeletons, many trunk muscle EMG patterns and gait characteristics were similar and presented periodic changes.
Moments produced by trunk muscles can contribute to the power of the lower limbs. The movement of upper limbs and trunk caused lower limb motion. RA involved trunk flexion and obliquity (8). Normalized amplitude of RA in the single-support phase increased significantly, while the contralateral counterpart did not change much. This may be because the participant generated more muscle force to laterally bend than to flex the trunk when walking with un-powered exoskeletons. OE bilaterally compresses the abdomen and flexes the trunk; unilaterally rotating the trunk to the opposite side (8). OE had the same changing trends as RA in the single-support phase. The changes in the bilateral OE were not identical. Therefore, it could be concluded that the participant generated more muscle force to rotate the trunk. ES extends and laterally bends the trunk (8). In the swing phase (right leg), the IEMG of the right OE in 4 conditions were much higher than on the left side, meaning that the participant swung their leg not only through the moments generated by trunk flexion and extension (7), but also by trunk rotation. The normalized amplitude of the ES in the double-support phase decreased significantly, while the contralateral counterpart changed little. This could infer that the participant generated more muscle force to laterally bend trunk. The asymmetric EMG activities of bilateral RA, OE and ES may have been caused by: (i) asynchronous movements of the left and right sides of the body; (ii) differences between bilateral residual muscle strengths; and (iii) daily usage habits and the way the participant moved.
The normalized EMG waveforms of the bilateral LD did not change significantly and maintained a relatively low %MVC. This may be because the LD with attachments to T1–L5 of the spine were not severely injured and had been strengthened by lengthy training. It could also be explained by LD having primary effects on the shoulder joint and shoulder girdle, which contribute to obliquity, rotation, and extension of the spinal column. These LD functions could cause complex motion patterns that were difficult to infer from the EMG signals.
Effects of different un-powered exoskeletons on trunk muscle activities
The mean and maximum normalized EMG of the OE in the KAFO and IRGO conditions were much higher than those in the ES-EXO condition. The maximum values occurred on heel strike. Compared with the ES-EXO condition, in the KAFO condition the participant swung their leg, not only through flexing, but also through rotating the trunk and pelvis without stored energy components. Compared with the ES-EXO (w), a lack of pelvic shell caused a large rotation range of the trunk and pelvis, which probably required greater muscle force. In the IRGO condition, hip flexion was driven by contralateral hip extension through the reciprocal rocking pelvic band (9). Users usually adopt a flexed trunk posture to ensure stability through increasing the area of support created by the feet and the walker (7). Consequently, it is difficult to extend the hip joint on the support side. The data in this study demonstrated the point. Therefore, the participant still attempted to swing the leg through rotating the trunk and pelvis. However, the rotation range of the trunk and pelvis were limited, since they were rigidly linked. The inharmonious interaction between the participant and the IRGO caused low walking speed, small step length and large muscle force.
In the ES-EXO condition, the energy stored in tensile spring 1 in the last gait cycle released when the leg swung and, in the meantime, the contralateral hip joint extended, and tensile spring 1 on the hip extension side was stretched passively in the swing phase. The energy stored in tensile spring 1 was generated by contraction of the ES on the hip extension side, which was proved as the IEMG of the ES on the hip extension side in the ES-EXO condition was greater than in other conditions. The energy was released mainly to compensate for the muscle effort of the OE in the swing phase.
When the localized muscles of the trunk repeatedly contract, maintaining a high level of recruitment, this can result in fatigue, which may reduce walking duration and distance. An un-powered exoskeleton that can recruit trunk muscles evenly and smoothly rather than make specific muscles (e.g. the OE and RA) produce great force suddenly may be more suitable and consume less metabolic energy.
Study limitations
Measurement error came mainly from marker placement. Pelvis and lower limb markers were difficult to attach to the skin, as the un-powered exoskeletons prevented direct placement, except for the pelvis in the KAFO condition. In addition, we only investigated 4 pairs of typical superficial trunk muscles. However, many other muscles (e.g. transverse abdominus, obliquus internus, etc.) also play important roles in trunk and pelvic motion.
Conclusion
The study subject generated large muscle force to olaterally bend and rotate the trunk, and swung his leg through the moments generated, not only using trunk flexion and extension, but also using trunk rotation. In the ES-EXO condition, the energy generated by ES contraction was stored in tensile spring 1 and released in the next gait cycle to compensate for energy generated by the OE and to provide moment for hip flexion. These findings prompt further development of un-powered exoskeletons and further investigation into the functions of trunk muscles in patients with SCI when walking with un-powered exoskeletons.
ACKNOWLEDGEMENTS
The study was supported by grants from National Key Technology R&D Program of China (grant number 2012BAI34B02). The authors are grateful to the participant who cooperated with the investigation and the National Research Center for Rehabilitation Technical Aids, China for equipment support. Special thanks are extended to Professor Zhixiu Hao for advice on manuscript revision.
REFERENCES

