Yngve Roe, PhD and Sigrid Østensjø, PhD
From the Department of Physiotherapy, Faculty of Health Sciences, Oslo and Akershus University College of Applied Sciences, Oslo, Norway
OBJECTIVE: To expand on a previous systematic review of shoulder-specific outcome measures by investigating how concepts of functioning were conceptualized and measured, using International Classification of Functioning, Disability and Health (ICF) constructs as a reference.
METHODS: The material consisted of the linked content of 17 condition-specific measures. The distribution of the key concepts of functioning was assessed in relation to the 3 ICF levels: body level (body functions and structures), personal level (activities) and societal level (participation). Based on this categorization, the concepts were further explored; body functions as to whether they were informed by any contextual information, and activities and participation as to whether they measured a person’s capacity, capability or performance.
RESULTS: Seven measures assessed all 3 levels of functioning, 8 measured 2 levels, and 2 measured a single level. The majority of the 15 measures including body functions assessed a mix of decontextualized and contextualized functions. Of the 13 measures of activities, 7 measured capabilities, 4 performance and 2 used both constructs. In comparison, among the 11 measures of participation, 5 measured capabilities, 2 performance and 4 a mixture of these. No measure used the capacity construct.
CONCLUSION: Shoulder-specific outcome measures differ in their choice of measurement levels and measurement constructs. The inconsistent use of the capability and performance constructs to measure activities and participation, raise important questions about the suitability of the measures for their intended use.
Key words: ICF; outcome assessment (healthcare); shoulder pain; disability evaluation; World Health Organization; recovery of function; rehabilitation/cl [classification]; rehabilitation.
J Rehabil Med 2016; 48: 325–332
Correspondence address: Yngve Roe, Department of Physiotherapy, Faculty of Health Sciences, Oslo and Akershus University College of Applied Sciences, Postboks 4 St. Olavs plass, NO-0130 Oslo, Norway. E-mail: yngve.roe@hioa.no
Accepted Jan 20, 2016; Epub ahead of print Mar 17, 2016
INTRODUCTION
The point prevalence of shoulder pain in the general population is between 7% and 27% in adults younger than 70 years (1). Many cases of shoulder pain are long lasting; it has been shown that only 20% of patients with a new episode are completely resolved 6 months later (2). The associated disability is often multi-dimensional, involving a range of movement-related functions, daily activities and psychosocial functioning (3–5).
In rehabilitation, the primary outcome of treatment interventions is patient-reported disability. Within the field of shoulder pain rehabilitation, for this purpose a number of patient-reported measures and measures that contain a mix of patient- and clinician-reported sections, are available (6, 7). Thus far, there is no consensus on which aspects of functioning should be included in shoulder-specific outcome measures (8–10). The lack of clarity surrounding both the concepts to be included and measurement constructs makes it a challenge to select measures that capture the most important aspects of functioning in relation to the purpose and population.
With the approval of the International Classification of Functioning, Disability and Health (ICF) a universal framework and standard language is now available for analysis of concepts and constructs of measures (11). The bio-psycho-social perspective of the ICF is reflected in its 3 components: body functions and structures, activities, and participation. Whereas activities reflect the individual level, participation reflects the societal level of functioning.
When published, no formal distinction was made between the constructs of activities and participation in the ICF’s classifications (11). Following this endorsement, efforts have been made to empirically investigate the distinction between these 2 constructs (12, 13). By introducing capacity and performance as qualifiers, the ICF acknowledges the importance of context when measuring activities and participation. Capacity refers to an individual’s maximal ability in a standardized environment, while performance refers to what an individual actually does in the natural environment. A third construct, capability to perform a task in the daily environment, taking into account the physical and social environment in which the activity can or cannot be performed, has been suggested (14–16). The person environment interaction is the discriminating element between capacity, capability, and performance (16). The use of, and relationships between, these constructs, and the impact of the context on the measurement of body functions, have been scarcely investigated.
In a previous systematic literature review, we described the content of widely used measures for patients with shoulder pain by linking the content to the most precise ICF category (17). The review showed that frequently used generic measures, such as the Short Form 36 (SF-36), contain few additional concepts to those included in the most wide-ranging condition-specific measures. The present article aimed to expand our previous review of the shoulder-specific measures by also investigating their conceptual basis and measurement constructs, using the ICF constructs as a reference. First, we assessed how the item content of each measure was distributed on the 3 ICF levels of functioning: the body level (body functions and structures), the personal level (activities), and the societal level (participation). Secondly, we investigated how functions reflecting the body, personal, and societal levels were conceptualized and measured.
MATERIAL AND METHODS
Material
The material used in the present article was the assessment form of the 17 frequently cited condition-specific measures. Of these, 16 were identified in the previous literature review (17). In addition, a modified version of the American Shoulder and Elbow Shoulder Score (Modified ASES) was included (18). The Patient Self-Evaluation section of the ASES has a separate summed score (19). For this reason, this section and the Physician Assessment of the ASES were assessed separately. An overview of the 17 condition-specific measures in relation to the publication source and year, the number of citations, the type of measure, the targeted population, the number of items, and the type of score are displayed in Table I.
|
Table I. Characteristics of the condition-specific measures (n = 17) |
||||||||
|
Measure |
Citations, n |
Abbreviation |
Dissemination |
Year |
Type of measure |
Target population |
Items, n |
Type of score |
|
American Shoulder and Elbow Surgeons Standardized Form for Assessment of the Shoulder (19) |
77 |
ASES Patient Self-Evaluation |
Journal of Shoulder and Elbow Surgery |
1994
|
Patient reported
|
Shoulder disorder
|
18 |
Summed score (0–100) |
|
ASES Physician Assessment |
Journal of Shoulder and Elbow Surgery |
1994 |
Clinician reported |
Shoulder disorder |
29 |
Item score |
||
|
American Shoulder and Elbow Surgeons Standardized Form for Assessment of the Shoulder, patient reported section (18) |
3 |
Modified ASES |
Journal of Shoulder and Elbow Surgery/ Journal of Bone & Joint Surgery |
1996 |
Patient reported |
Upper-extremity disorder |
13 |
Summed score (0–100) |
|
Constant Murley Shoulder Score (28) |
124 |
Constant |
Clinical Orthopaedics & Related Research |
1987 |
Patient- and clinician reported |
Shoulder disorder |
11 |
Summed score (0–100) |
|
Disabilities of the Arm, Shoulder and Hand scale (24) |
51 |
DASH |
American Journal of Industrial Medicine |
1996 |
Patient reported |
Upper-extremity disorder |
30 |
Summed score (0–100) |
|
Disabilities of the Arm, Shoulder and Hand scale (11 item) (29) |
7 |
QuickDASH |
Journal of Bone & Joint Surgery |
1996 |
Patient reported |
Upper-extremity disorder |
11 |
Summed score (0–100) |
|
Flexilevel Scale of Shoulder Function (30) |
6 |
FLEX-SF |
Medical Care |
2003 |
Patient reported |
Shoulder disorder |
34* |
Summed score |
|
Oxford Shoulder Score (10, 31) |
11 |
OSS |
The Journal of Bone and Joint Surgery British/Archives of Orthopedic and Trauma Surgery |
1996 |
Patient reported |
Rotator cuff disorder |
12 |
Summed score (0–48) |
|
Penn Shoulder Score (32) |
5 |
Penn |
The Journal of Orthopaedic and Sports Physical Therapy |
2006 |
Patient reported |
Shoulder disorder |
24 |
Summed score (0–100) |
|
Rowe Shoulder Score (33, 34) |
31 |
Rowe |
The Journal of bone and joint surgery. American volume |
1988 |
Patient- and clinician reported |
Shoulder disorder |
8 |
Summed score (0–100) |
|
Shoulder Disability Questionnaire (25) |
14 |
SDQ-NL |
Journal of Clinical Epidemiology |
2000 |
Patient reported |
Shoulder disorder |
16 |
Summed score (0–100) |
|
Shoulder Pain and Disability Index (23, 35) |
31 |
SPADI |
The Official Journal of the Arthritis Health Professions Association |
1991 |
Patient reported |
Shoulder disorder |
13 |
Section scores Pain/functioning (0–100) |
|
Shoulder Rating Questionnaire (36) |
15 |
SRQ |
The Journal of Bone and Joint Surgery |
1997 |
Patient reported |
Shoulder disorder |
21 |
Summed score (17–100) |
|
Simple Shoulder Test (37) |
46 |
SST |
The American Academy of Orthopedic Surgeons |
1993 |
Patient reported |
Shoulder disorder |
12 |
Summed score (0–12) |
|
University of California at Los Angeles shoulder rating scale (38) |
64 |
UCLA |
The Journal of bone and joint surgery |
1986 |
Patient- and clinician reported |
Rotator cuff disorder |
5 |
Summed score (2–35) |
|
Walch-Duplay Score for Instability of the Shoulder (39) |
5 |
Walch-Duplay |
Congress of the European Society of Surgery of the Shoulder and Elbow, Paris |
1987 |
Patient- and clinician reported |
Instability of the shoulder |
4 |
Summed score (0–100) |
|
Western Ontario Rotator Cuff Index (26) |
21 |
WORC |
Clinical Journal of Sport Medicine |
2003 |
Patient reported |
Rotator cuff disorder |
21 |
Summed score (0–2,100) |
|
Western Ontario Shoulder Instability Index (27) |
8 |
WOSI |
The American Journal of Sports Medicine |
1998 |
Patient reported |
Instability of the shoulder |
21 |
Summed score (0–2,100) |
|
*Adaptive measure with easy, middle or difficulty testlets, based on a single branching item. |
||||||||
To investigate whether any recent changes in the use of condition-specific measures have taken place, an updated search in Medline on studies published between August 2012 and December 2014 was conducted, using the same search strategy and inclusion and exclusion criteria as in the review (17). The updated search indicates less frequent use of the Constant and the Shoulder Pain and Disability Index (SPADI) and more frequent use of the American Shoulder and Elbow Surgeons (ASES), Disabilities of the Arm, Shoulder, and Hand Questionnaire (DASH) and its short version (QuickDASH). No new measures were identified.
Content and conceptual analyses
In the previous review, the item content of the included measures was linked to the ICF using the established rules (20, 21). For one of the measures, the DASH, an already published linkage, was used (22). For the present analyses, we preferred to link the DASH using the same procedure as described in detail in the original article (17). The results differed for 1 item (item 30). We linked the concepts “feeling less capable, less confident or less useful” to the ICF category “b152 Emotional functions” instead of a personal factor (22).
The current paper expands our previous content analyses by first investigating how the linked item content was distributed on the 3 ICF levels of functioning: body (body functions and structures), personal (activities), and societal level (participation). This classification of content was based on the recommendations from Whiteneck & Dijkers (12); ICF categories belonging to chapter d1-d6 (except the category “d660 Assisting others”) were classified as activities, and those belonging to chapter d7–d9 were classified as participation (Table II). To perform these classifications, we identified the key concept of every item. For example, in the item, “How severe is your pain; pushing with the involved arm?” (23), “pain” was recognized as the key concept.
|
Table II. Chapter structure of the activities and participation component (d) of the International Classification of Functioning, Disability and Health (ICF) |
|
|
d1 |
Learning and applying knowledge |
|
d2 |
General tasks and demands |
|
d3 |
Communication |
|
d4 |
Mobility |
|
d5 |
Self-care |
|
d6 |
Domestic life |
|
d7 |
Interpersonal interactions and relationships |
|
d8 |
Major life areas |
|
d9 |
Community, social and civic life |
Secondly, we investigated the constructs that were used to measure body functions, activities and participation. To classify how body functions were requested, we considered whether a concept of body function was informed by any contextual information. Using the most frequent concept, “pain”, as an example, it can be requested without any contextual information, e.g. “Please rate the severity of the following symptoms in the last week; arm shoulder or hand pain” (24), or informed by contextual information, e.g. “My shoulder hurts when I open or close a door” (25). In the first example pain was classified as a decontextualized sensation and in the second as a contextualized sensation.
The assessment of the activities and participation concepts was based on the 3 constructs presented in the introduction to distinguish activity: capacity, capability and performance (15, 16). To perform this classification we first decided on whether the measurement construct reflected what a person can do (capacity or capability) or does do (performance). The further distinction between capacity and capability was based on the context, a standardized environment, for example a test situation (capacity) or a daily environment (capability). To give some examples of the classification: the measurement construct of the item “Please rate your ability to do the following activities in the last week; wash your back?” (24), was classified as a capability, whereas “How much difficulty do you have dressing or undressing” (26), as performance.
The conceptual analyses within body functions, activities and participation were conducted independently by 2 reviewers (YR and SO). The agreement was 87% within body functions and 89% within activities and participation. Cases of disagreement were resolved by discussion between the 2 reviewers.
RESULTS
A total of 17 condition-specific measures were included in the analyses (Table II). From these measures, 289 key concepts were linked to the body level (body functions and structures), personal level (activities) and societal level (participation) of functioning. Within the body level, 126 concepts were recognized, 132 within the personal level and 31 within the societal level. Three concepts (related to medication) were linked to environmental factors and 11 concepts were deemed not covered by the ICF.
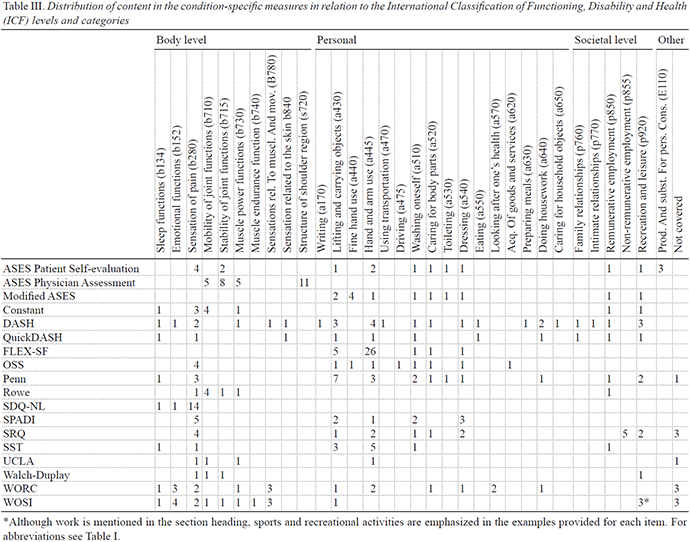
The distribution of the key concepts for each measure in relation to the body, personal and societal levels of functioning is shown in Fig. 1, and in more detail in Table III.
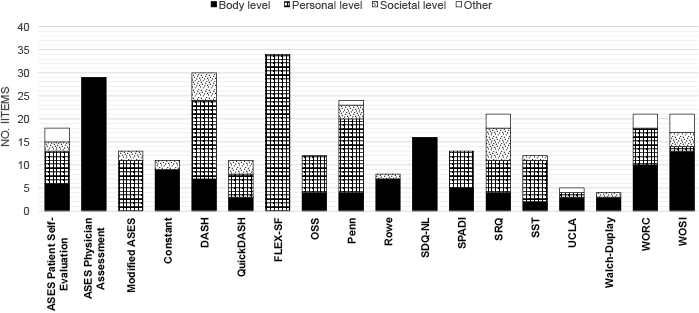
Fig. 1. Distribution of the concepts included in the condition-specific measures in relation to the body, personal, and societal levels of functioning. For Abbreviations see Table I.
Seven measures contained key concepts reflecting all 3 of the body, personal and societal levels: the ASES (Patient Self-Evaluation), DASH, QuickDASH, Penn Shoulder Score (Penn), Shoulder Rating Questionnaire (SRQ), Simple Shoulder Test (SST) and Western Ontario Shoulder Instability Index (WOSI). Concerning the ASES, the Patient Self Evaluation section requested functions representing all levels, whereas the Physician Assessment section requested only body functions and structures. Eight measures reflected 2 levels of functioning, of which 4 measures concerned body functions and activities (the Oxford Shoulder Score (OSS), SPADI, University of California at Los Angeles shoulder rating scale (UCLA) and WORC), 3 measures concerned body functions and participation (the Constant, Rowe and Walch Duplay) and 1 measure concerned activities and participation (the Modified ASES). The last 2 measures reflected concepts from a single level; the Shoulder Disability Questionnaire (SDQ) covered the body level, and the Flexilevel Scale of Shoulder Function (FLEX-SF) covered the personal level.
In the conceptual analyses, we first investigated whether the body level functions were measured decontextually or contextually (Fig. 2). Of the 15 measures covering body functions and structures, 11 requested a mix of decontextualized and contextualized information, 2 included contextualized information alone (the Shoulder Disability Questionnaire (SDQ-NL) and the SST), and 2 included decontextualized information alone (the Physician Assessment section of the ASES and the Walch-Duplay). The most frequently requested concept, pain, was measured in 48 items, of these 14 were decontextualized and 34 contextualized. When pain was decontextualized it was requested in terms of severity or type of pain. Pain as a contextualized experience was measured in 3 ways: pain in relation to a defined activity, pain interference with daily activities, or pain as a cause of activity limitations. Two other concepts, sleep and emotional functions, were included in 8 and 9 items, respectively. They were in all cases contextualized, referring to the affected body part, most often the shoulder. Emotional functions were requested in 4 measures, the DASH, SDQ-NL, WORC and WOSI. The concepts that were classified as emotional functions in these measures were frustration, bad temper, concern and depression (24–27).
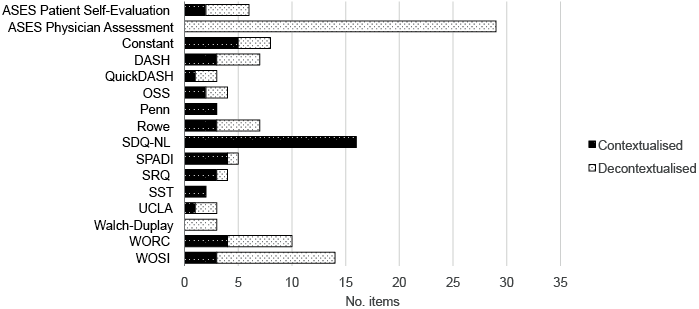
Fig. 2. Distribution of contextualized and decontextualized body level concepts. For abbreviations see Table I.
No measure utilizes the capacity construct to measure activities or participation. Of the 13 measures that contained activities (Fig. 3), 7 measured capabilities (the ASES Patient Self-Evaluation, Modified ASES, DASH, QuickDASH, Penn, SST and UCLA), 4 measured performance (the FLEX-SF, SPADI, WORC and WOSI) and the last 2 (the OSS and SRQ) use both constructs, with the OSS mainly using capability and the SRQ mainly using performance. Of the 11 measures that included participation concepts (Fig. 4), 5 measured capabilities (the ASES Patient Self-Evaluation, Modified ASES, Penn, Rowe and SST), 2 measured performance (the Constant and Rowe) and 4 measured a mix of capability and performance (the DASH, QuickDASH, SRQ and WOSI).
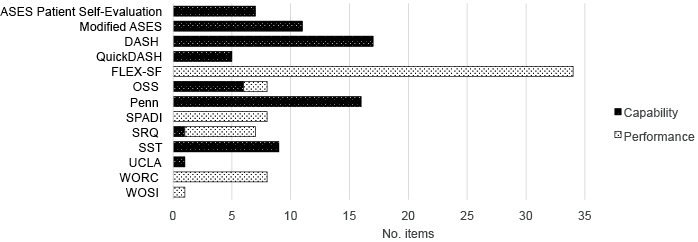
Fig. 3. Distribution of capability and performance constructs at personal level of functioning. For abbreviations see Table I.
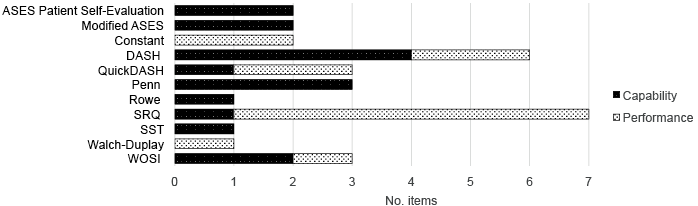
Fig. 4. Distribution of capability and performance constructs at societal level of functioning. For abbreviations see Table I.
DISCUSSION
Using the ICF constructs as a reference, the content and measurement constructs in 17 widely used shoulder-specific measures were thoroughly analysed. The results showed considerable differences with regard to the levels and domains of functioning included, and how the item content was conceptualized and measured.
The content of 7 measures, the ASES (Patient Self-Evaluation), DASH, QuickDASH, Penn, SRQ, SST and WOSI covered all 3 levels of functioning (body, personal and societal) (Fig. 1 and Table III). All of these measures made use of a single summed score, which is intended to represent the impact of shoulder pain on functioning. A fundamental requirement for summed rating scales is the unidimensionality of the measured construct (40). The dimensionalities of 2 of the multilevel measures, the DASH and QuickDASH, were investigated using both classical test theory and item response theory (Rasch) (24, 41, 42). For the DASH, neither the unidimensionality, nor the key domains identified by the developers were confirmed (24, 41). Due to these findings, the scoring method and future development of the DASH and QuickDASH have been debated (43). We assume that the 2 DASH measures are not the only multilevel measures with unidimensionality problems. This illustrates the challenges of designing measures that cover different levels of functioning of relevance for the patient, and at the same time have sound psychometric properties (24, 44). The increased use of item response theory may encourage the development of measures that cover a single, underlying trait (40, 45).
Another important issue in disability measurement is the framing of questions; specifically the effect of the context implied by the questions. Among the 15 measures that included body level functions, the most common approach was to request a mix of decontextualized and contextualized information (Fig. 2). Pain was requested in 15 of 17 measures (Table III). In line with recommendations for assessment of pain (46), we found that many of the measures requested both the severity/type of pain, and how pain interferes with daily activities. Pain interference, however, was contextualized differently. This can be illustrated with 2 DASH items. The framing of the question: “To what extent has your arm, shoulder or hand problem interfered with your normal social activities with family, friends, neighbours or groups?” (24), points to a biopsychosocial understanding of pain that incorporates a dynamic interaction between physical, psychological, and social factors. In comparison, the question “Were you limited in your work or other regular daily activities as a result of your arm, shoulder or hand problem?” (24), indicates a causal relationship between pain and activity limitations. Such a relationship was assumed in many measures, making use of such terms as “because of” and “due to”.
In the taxonomy of the Association for the Study of Pain (IASP), pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage (47). Altogether 4 measures, the SDQ-NL, DASH, WORC and WOSI, requested emotional experiences. The emotional experiences were in all cases contextualized, such as in the WORC item, “How much frustration do you feel because of your shoulder?” (26). There is evidence to suggest that psychological factors, such as worrying and lack of vitality, are associated with persistent pain (5, 48). There is also emerging evidence about the effectiveness of treatment interventions that are based on screening of risk factors (49, 50). These findings suggest that emotional distress should be implemented in the baseline assessment of patients, rather than in outcome evaluations. For this purpose validated screening instruments, such as the Orebro Screening Questionnaire, is available (51).
The ICF supports the use of 2 qualifiers, capacity and performance, to measure activities and participation (11). Introduction of an opportunity qualifier, e.g. the ability of an individual to perform a task in the daily environment, taking into account the physical environment (capability), has been suggested (14–16). None of the measures included concepts reflecting the capacity construct. Among the 13 measures that included personal level concepts (activities), 7 made use of the capability construct and 4 used performance, whereas only 2 made use of both constructs (Fig. 3). In comparison, 4 of 11 measures used a mix of constructs to measure the societal level (Fig. 4), 5 used the capability construct and 2 the performance construct. Thus, the conceptual distinctions exposed by disability experts are not fully reflected in the shoulder-specific measures (52, 53). As an example, the developers of the DASH aimed to capture “difficulty doing activities in any domain of life (..) due to a health or physical problem” (24). The term “doing” reflects the performance construct (16); however, the majority of the DASH concepts were conceptualized as capabilities referring to what the person “can do” in the context of daily activities.
The implicit assumption is often that a person’s capacity or capability reflects his/her upper limits of performance. However, little is known about the relationship between a person’s capacity, capability, and performance or about change in functioning over time in patients with shoulder pain disorders. Capacity or capability may be favoured as an outcome when the objective is to detect the early clinically important change in disability. Over short time periods, interventions may improve capacity and capability, but such improvements may not have had sufficient time to be integrated into performance (15). Williams presents a strong argument for considering the social importance of activities in understanding differences between capacities and performance (52). Performance depends on more than just capacities and functional capabilities, such as personal factors and policies that are beyond the scope of the healthcare (14, 15). In the recently updated guide to physical therapy practice from the American Physiotherapy Association (APTA) (54), it is recommended to take into consideration the differences between the highest level of functioning of which the individual is capable and the highest level of functioning that is likely to be habitual for that individual. However, the implications for assessment of functioning are not discussed further.
The considerable variations we found in the distribution of the content in the condition-specific measures indicate disparate views on not only what to measure, but also how to measure the included concepts. Previous reviews have provided useful information about the psychometric properties of shoulder-specific measure (3, 55–58). However, the selection of a measure depends on many factors including the research questions or clinical purpose, the type of intervention and the instrument’s content and measurement constructs. Our findings may help professionals to select a measure that best capture the study or clinical purpose and the outcome parameters. For example, if considering use of the DASH or QuickDASH, professionals should acknowledge that both reflects a biopsychosocial understanding of functioning, request a mix of contextualized and decontextualized information on body functions, and measure both capabilities and performance. The QuickDASH is almost as wide-ranging as the DASH, although each of its included concepts is measured by only a single item. However, in both research and in clinical practice there is a need for ways to document more specific outcomes in more depth. If detailed information about pain in interaction with daily activities is of concern, the SDQ-NL and the SPADI would be appropriate alternatives. When mobility performance functions of the arm are important outcomes, the FLEX-SF may be the preferred measure.
This article has some limitations concerning the conceptual analyses of the measurement constructs. To date, there are no established guidelines to guide conceptual analysis of the measurement constructs. A third independent researcher was not consulted for the concepts that were classified differently by the 2 authors. We suggest that our analyses can be a way to start developing more standardized procedures for conceptual analyses based on the ICF constructs.
In conclusion, the ICF-based analyses showed a variation in the number of, and the levels of, functioning that were included in the measures. Of the body level functions, pain was measured both decontextualized and contextualized, whereas sleep and emotional functions always were measured contextualized. Activities and participation was measured either as a capability or performance. The use of these constructs seemed to be inconsistent within and between the measures. These differences in distribution of content and measurement constructs should be considered in the selection of measures.
REFERENCES