
Pain and Rehabilitation Centre, and Department of Medical and Health Sciences, Linköping University, SE-581 85 Linköping, Sweden
Objective: To explore how demographics, pain, psychosocial factors and insomnia relate to the spread of chronic pain.
Methods: The study included 708 patients (68% women; median age 46 years; interquartile range 35–57 years) with chronic pain who were referred to a multidisciplinary pain centre. Spreading of pain was assessed using a questionnaire covering 36 anatomically predefined pain regions. Data were collected on demographics, pain symptoms, psychological distress, and insomnia (Insomnia Severity Index). Four sub-categories of chronic pain were established: chronic local pain, chronic regional pain medium, chronic regional pain heavy, and chronic widespread pain.
Results: The median number of pain regions was 10 (interquartile range 6–18). Prevalence of chronic pain was as follows: chronic local pain 9%, chronic regional pain medium 21%, chronic regional pain heavy 39%, and chronic widespread pain 31%. In the regression models, being a woman and persistent pain duration had the strongest associations with spreading of pain, but anxiety, pain interference, and insomnia were also important factors.
Conclusion: Spreading of chronic pain can only partly be explained by the simultaneous levels of insomnia. Female sex, pain duration, pain interference and anxiety appear to have more significant relationships with the spread of pain. Targeting these factors may lead to improvements in treatment and prevention strategies.
Key words: chronic pain; anxiety; depression; health; human; insomnia; Insomnia Severity Index; ISI.
Accepted Sep 6, 2016; Epub ahead of print Nov 30, 2016
J Rehabil Med 2017; 49: 63–70
Correspondence address: Péter Alföldi, Pain and Rehabilitation Centre, University Hospital, SE-581 85 Linköping, Sweden. E-mail: peter.alfoldi@regionostergotland.se
An increase in the number of musculoskeletal pain sites on the body reflects the spreading of chronic pain. Clinical practice distinguishes 3 types of chronic pain: chronic local pain (CLP), chronic regional pain (CRP), and chronic widespread pain (CWP) (including fibromyalgia) (1–3). There is growing evidence that spreading pain is more frequent than localized pain (4). In addition, spreading of chronic pain has been found to be significant for the prognosis of disability and is strongly associated with a decrease in overall physical, as well as psychological, health (1). Furthermore, in contrast to CLP, CWP has been linked with both greater general disability and greater work disability (2, 3).
Given the negative effects of CWP, understanding the factors that initiate and maintain spreading of chronic pain is crucial for developing prevention strategies and treatments. Female sex, higher age, family history of pain, depressed mood, and the number of pain sites at baseline may be risk factors for the transitioning of CLP/CRP to CWP (5). For patients with fibromyalgia, a prominent proportion of CWP, hyperexcitability and psychological mechanisms, such as anxiety, depression, sleep impairment, and daytime fatigue, may play a significant role in generalizing of pain (6, 7).
More recent attention has focused on exploring the relationship between insomnia and chronic pain (8–11). Insomnia, a type of sleep impairment, is a common complaint in patients with chronic pain; the prevalence varies between 50% and 80% (12–14). In our previous study of a chronic pain cohort at our university hospital, 65% of patients had clinically significant insomnia (15).
Bidirectional connection of insomnia and pain may seem obvious, but recent studies challenge a direct reciprocal directionality (16, 17). Α systematic review advocates that sleep impairment is a stronger predictor of chronic pain than chronic pain is of sleep impairment (18). Although several studies have explored the bidirectional connection between pain and insomnia (19–21), few have focused on the relationship between spreading of pain, CWP and insomnia (8, 22). However, these studies arrived at different conclusions; in part, these discrepancies can be traced to the fact that they used different definitions of spreading of pain, especially of CWP, and used different methods to measure insomnia. Thus, our knowledge of how spreading of pain is associated with insomnia is limited. Moreover, knowledge of whether this relationship can be explained by, for example, demographics, pain and psychosocial factors in chronic pain patients, is sparse.
The aims of this study were to investigate whether insomnia is associated with spreading of pain, and whether age, sex, anxiety, depression, pain interference, kinesiophobia, and pain acceptance explain the relationship between spreading of pain and insomnia. In addition, this study evaluates age and sex differences with respect to spreading of pain and insomnia.
This cross-sectional study includes patients with pain referred to our specialized pain rehabilitation clinic during a 1-year period. In total, 846 patients completed a battery of questionnaires with respect to the Swedish Quality Registry for Pain Rehabilitation (SQRP; http://www.ucr.uu.se/nrs/), as described below (15, 23). Before the assessment, all patients gave their informed consent. Age restrictions were not applied. Patients who reported that their pain had been a problem for less than 3 months and those who reported no anatomical regions with pain were excluded from this study. The study was granted ethics clearance by the Umeå University Ethics Committee (Dnr: 2013/192-31).
Since 1998, the SQRP has collected aggregated national data. The registry is based on questionnaires (validated Swedish versions) completed by patients with chronic pain referred to approximately 40 clinical departments, equating to > 90% coverage of the clinical departments of pain rehabilitation at the specialist level in Sweden (15, 23). Patients complete questionnaires on 3 occasions: at entry assessment, immediately after finishing a rehabilitation programme, and 1 year after completing a rehabilitation programme. The register includes descriptive variables of the patients’ backgrounds, pain characteristics, and scales for other symptoms (such as depression and anxiety) and aspects of function, activity/participation, and quality of life.
This study uses data from patients referred to the Pain and Rehabilitation Centre at the University Hospital in Linköping, Sweden. The selection of variables from the SQRP was based on their relevance to the present focus and on the results from our previous paper, which analysed the prevalence of insomnia and the correlation and relative importance of psychological and social demographic factors with insomnia in a similar population of patients with chronic pain (15).
Characteristics of pain. Pain intensity for the previous 7 days was registered using an 11-graded numeric rating scale (NRS7d) with numbers provided for guidance (0 = no pain and 10 = worst imaginable pain) (24). The duration of pain and the duration of persistent pain (in months) were also captured.
On a list of 36 anatomical predefined areas (18 on the left side and 18 on the right), the subjects marked those areas where they were experiencing pain. The number of the above predefined anatomical areas associated with pain was calculated and labelled as the number of pain regions. Thus, the number of pain regions ranged between 1 and 36, with higher values indicating higher spreading of pain. Next, chronic pain was operationalized into 3 categories: CLP, CRP with 2 subgroups (1 medium and 1 heavy), and CWP. These categories were defined as follows: CLP: 1–2 anatomical areas; CRPmedium: 3–6 anatomical areas; CRPheavy: ≥ 7 anatomical areas, but not CWP. CWP was present when patients reported pain in the spine and a minimum of 1 area on all 4 quadrants of the body according to the criteria of American College of Rheumatism definition (25). This study presents results both for the number of pain regions and for the above-defined chronic pain categories.
Hospital Anxiety and Depression Scale. The HADS, a short, self-assessment questionnaire, measures the level of anxiety and depression. HADS comprises 7 items in each of the depression (HADS-D) and anxiety (HADS-A) subscales. Possible subscale scores range from 0 to 21, the lower score indicating the least depression and anxiety level possible. A score of 7 or less indicates a non-case, a score of 8–10 indicates a doubtful case, and a score of 11 or more indicates a definite case. HADS is frequently used and has good psychometric characteristics (26).
Multidimensional Pain Inventory. MPI is a 61-item self-report questionnaire measuring psychosocial, cognitive, and behavioural effects of chronic pain. It has 3 sections. In the present study, several variables from Section 1 were used: e.g. MPI-Pain severity – a mean of 3 questions, 2 about pain intensity, score 0–6 (the lower score the less intense pain) and 1 how much suffering the pain causes the individual; MPI-Pain Interference – pain-related interference in everyday life, measured by the mean of 11 questions; MPI-Affective Distress, reflecting affective imbalance, a mean of 3 questions, 1 about mood, 1 about anxiety, and 1 about level of irritation (the lower score the more stable affect). The instrument has provided satisfactory psychometric properties (27).
Tampa Scale for Kinesiophobia. TSK measures fear of pain and re-injury (28). The items are rated on a 4-point Likert scale, from ‘’strongly disagree” to ‘’strongly agree”. The total score has a range of 17 to 68; scores higher than 36 for women and higher than 38 for men indicate high pain-related fear. The TSK scale is a reliable assessment tool in chronic pain populations (28, 29).
Chronic Pain Acceptance Questionnaire. CPAQ measures acceptance behaviours and attitudes toward pain. CPAQ is a 20-item scale with 2 subscales: activity engagement independent of pain (score range 0–66; denoted CPAQ-engagement) and willingness to accept pain/need to control pain (score range 0–54; denoted CPAQ-willingness) (30). All items are rated on a scale from 0 (never true) to 6 (always true). The CPAQ is reliable and valid both in the English and Swedish versions (31).
Insomnia Severity Index. ISI is a reliable and valid instrument for detecting cases of insomnia with excellent internal consistency (32). The 7 items of the ISI are rated on a 5-point Likert scale (0–4). The scores of the 7 items are summed to create the total score of the ISI (maximum 28). The score is divided into 4 categories: no clinically significant insomnia (ISI 0–7); sub-threshold insomnia (ISI 8–14); moderate clinical insomnia (ISI 15–21); and severe clinical insomnia (ISI 22–28). Both total score and subcategories of ISI were used for descriptive purposes and univariate analyses, while only total score was used in the regression models.
All statistical analyses were performed using the statistical package IBM SPSS Statistics (version 22.0; IBM Inc., New York, USA). p < 0.05 (2-tailed) was considered significant in all tests. Data are presented as median and interquartile range (IQR) for continuous variables and as count (%) for categorical variables. The criteria for testing normality was ≥ ±2.00 for the skewness and ≥ ± 7.00 for the kurtosis, since the typical use of the Kolmogorov-Smirnov and the Shapiro-Wilk tests is not recommended for large sample sizes (33). The majority of variables showed skewness and kurtosis value no greater than recommended, thus we used parametric tests for data analysis. The independent Student’s t-test was used to evaluate sex differences on the ISI and the total scores for the number of pain regions. The χ2 goodness of fit test was used to compare the proportions of subcategories of chronic pain. The Pearson’s χ2 test was performed to compare categorical variables. Analysis of variance (ANOVA) was used to test the differences between the subgroups of chronic pain and other parameters/symptoms. Pearson correlation analysis was used for bivariate correlations (i.e. investigating the correlations between the number of pain regions and insomnia as well as other measurements). Multiple linear regression (MLR) models were performed to investigate the relative importance of insomnia (ISI) and other symptoms (i.e. variables with p < 0.05 in univariate analyses) for the number of pain regions (continuous variable). Multicollinearity was assessed by examining tolerance and the variance inflation factor (VIF). A tolerance of less than 0.20 or 0.10 and/or a VIF of 5 or 10 and above indicates a multicollinearity problem. However, in weak models a VIF of 2.5 may also indicate a multicollinearity problem (34). In addition, ordinal logistic regression (OLR) was used, with categories of pain treated as an ordinal outcome variable. Odds ratios (OR) and 95% confidence intervals (CI) are reported.
Of the 846 patients who completed the SQRP, 138 were excluded according to the exclusion criteria (16 reported pain duration of less than 3 months; 10 reported zero anatomical regions with pain; and 112 did not fully complete the duration of pain). Therefore, the final sample consisted of 708 patients with chronic pain.
There were 225 (32%) men (median age 51, IQR 38–61 years) and 483 (68%) women (median age 44, IQR 33–55 years) in the investigated pain cohort. Age differed significantly between the sex (p < 0.001). The median duration of pain was 61 months (IQR 20–142 months) and duration of persistent pain was 25 months (IQR 4–90 months). Most of the patients (70%) reported severe pain intensity (i.e. NRS7d >7/10) with a median pain intensity of 7 (IQR 6–8).
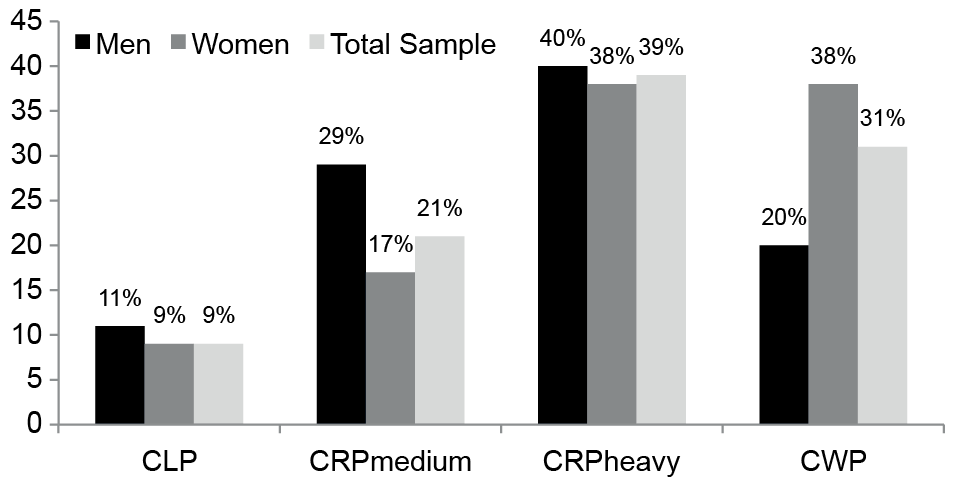
The median number of pain regions was 10 (IQR 6–18). Women had a higher number of pain regions than men (p < 0.001). The prevalence of chronic pain in terms of the 4 pain categories is shown in Fig. 1. A larger percentage of the total sample of patients had CRPheavy (39%) compared with CLP (9%), CRPmedium (21%) and CWP (31%) (p < 0.001). There was a significant difference between the sex in the proportions of categories of pain (p < 0.001); CLP was reported by 9% of women and 11% of men, CRPmedium by 17% of women and 29% of men, CRPheavy by 38% of women and 40% of men, and CWP by 36% of women and 20% of men.
Fig. 1. Percentages of the 4 categories of pain by sex and total sample. CLP: chronic local pain; CRP: chronic regional pain; CWP: chronic widespread pain.
Adults (age range 25–64 years) reported a significantly higher number of pain regions compared with youth (14–24 years) and seniors (65 years and over) (p < 0.001) (Fig. 2). However, age did not differ significantly between the 4 cate-gories of chronic pain (p = 0.075). Significant differences were found among the 4 categories of chronic pain and the following parameters: sex (female); pain duration; duration of persistent pain; pain intensity previous 7 days; Insomnia Severity Index; HADS-Anxiety; HADS-Depression; MPI-Pain severity; MPI-Pain-related interference with everyday life; and MPI-Affective distress. TSK, CPAQ-Engagement, and CPAQ-Willingness did not differ significantly between the 4 chronic pain categories (Table I).
Fig. 2. Median values of the Insomnia Severity Index (ISI) and the number of pain regions by different age groups.
Table I. Four categories of chronic pain with respect to the Insomnia Severity Index and other examined variables
For the same pain cohort, we recently reported a similar ISI median of 17 (IQR 12–21) and that the majority of the cohort (65.3%) had clinical insomnia (15). In the present calculation there was no significant difference between sex in ISI total score (p = 0.100). However, adults (age range 25–64 years) reported significant higher levels of ISI total score compared with youths (14–24 years) and seniors (65 years and over) (p < 0.001) (Fig. 2). With respect to the 4 pain categories, the median total ISI score was 14 (IQR 6–18) for CLP, 16 (IQR 9–20) for CRPmedium, 17 (IQR 12–22) for CRPheavy, and 19 (IQR 15–23) for CWP (Fig. 3). Significant differences in levels of insomnia between the 4 pain groups were found (p < 0.001) (Table I). Post hoc comparisons using the Bonferroni test showed that the CLP group was significantly different (p < 0.001) from the CRPheavy and CWP groups. However, the CRPmedium subgroup did not differ significantly from the CLP and CRPheavy groups (p > 0.05), but the CRPmedium subgroup differed significantly from the CWP group (p < 0.001) (Fig. 3).
Fig. 3. Box-plot of the median values of the Insomnia Severity Index (ISI) by categories of pain, based on the number of pain regions. CLP: chronic local pain; CRP: chronic regional pain; CWP: chronic widespread pain.
Moreover, 7% of the CWP subgroup had no clinically significant insomnia, 18% had sub-threshold insomnia, 44% had moderate clinical insomnia, and 31% had severe clinical insomnia. These figures differed significantly when we compared the 4 categories of chronic pain with respect to the 4 subcategories of ISI (p < 0.001). Interestingly, 75% of the CWP had clinical insomnia (Table I).
The next step in the analysis was the assessment of the correlations between the number of pain regions (i.e. spreading of pain) and the ISI, as well as other pain and health characteristics. The number of pain regions correlated positively with the ISI (r = 0.25; p < 0.001) and significantly (p < 0.01) with almost all other investigated factors (Table II). However, no significant correlation was found between number of pain regions and CPAQ-Willingness, whereas the number of pain regions correlated negatively with CPAQ-Engagement.
Table II. Correlations of number of pain regions, Insomnia Severity Index, and other variables; correlation coefficients are presented
Using MLR, the number of pain regions was regressed in order to understand the importance of ISI vs other symptoms and some socio-demographic variables (Table III). By means of multicollinearity, 3 variables (pain duration, NRS7d, and MPI-affective distress) were excluded due to collinearity with duration of persistent pain, MPI-Pain Severity, and HADS-Anxiety, and Depression. (The mean VIF was 2.56 and the mean tolerance was 0.39 and the correlation coefficients were above 0.70). When we excluded those variables, the regression model resulted in a mean VIF of 1.56 and a mean tolerance of 0.64 for all independent variables; values that indicate no multicollinearity.
Table III. Regression results (multiple linear and ordinal logistic regression models) of the number of pain regions (spreading of pain) in patients with chronic pain (upper analysis) and categories of chronic pain (CLP, CRPmedium, CRPheavy, and CWP) based on the number of pain regions treated as an ordinal outcome (lower analysis)
The results of the MLR revealed that the number of pain regions depended to some extent on different symptoms, including ISI (Table III). Specifically, female sex, ISI, persistent pain duration, MPI-Pain interference and HADS-Anxiety, had direct associations with the number of pain regions. We further regressed the categories of pain based on the number of pain regions (CLP, CRPmedium, CRPheavy, and CWP) treated as an ordinal outcome, and this produced very similar results with respect to the most important variables (Table III).
This cross-sectional study explored the associations between insomnia, pain and psychological distress and spreading of pain in patients with chronic pain. A few studies (8, 9, 11, 22) have examined this connection. Notably, we used a more comprehensive system of distinguishing between chronic pain categories to reflect spreading of pain: CLP; 2 types of CRP, CRPmedium and CRPheavy; and CWP. We found that the majority (70%) of patients in the present cohort had more or less severe widespread pain (CRPheavy + CWP). Spreading of pain is increasingly perceived as an important pain characteristic that needs to be better understood in order to capture the complexity of chronic pain (11). As expected, we found significant, but limited, correlations between the number of pain regions and pain intensity/severity (r: 0.220–0.233) (Table II). Furthermore, significantly more women than men had CWP, a finding that agrees with the well-known fact that widespread pain, including fibromyalgia, is 6 times more common in women (35).
We further specified that insomnia was associated with the number of pain regions. Our findings are consistent with previous studies showing that severe sleep problems were associated with CWP (8, 22). Moreover, we found that a higher level of spreading of pain was related to a variety of other pain-related measures as well as psychological factors such as anxiety, depression, and coping aspects (Table I). Similarly, Schuh-Hofer et al. found that, in addition to anxiety, other factors could contribute to the pathomechanism of insomnia and chronic pain (36).
The most important factors associated with both the number of pain regions and the categories of pain (Table III) were female sex, persistent pain duration, anxiety, pain interference, and insomnia. With respect to the multivariate analysis, the spreading of pain, as well as the presence of CWP, can only partly be explained by the simultaneous levels of insomnia according to ISI. Specifically, we found that pain interference, pain duration, and anxiety were stronger regressors than insomnia. Other variables (including pain severity and depression) were not associated with pain spreading. In addition, other studies have reported significant associations between spreading of pain and anxiety (37). Pain-related fear behaviours, measured by TSK, did not show consistent correlations with spreading of pain although general anxiety aspects, according to HADS, correlated significantly with spreading of pain (Table III). Pain intensity aspects differed between the pain categories (Table I), a finding also reported by other studies (38), but these aspects were not significant in the regression models (Table III). On the other hand, pain intensity may have an indirect effect via pain interference, which was a significant regressor (Table III). As with other studies, we found that female sex was associated with spreading of pain (Tables I and III), but we could not confirm an age dependence (3, 5). However, our final models accounted for only 20–22% of the total variance of spreading of pain (Table III), indicating a low influence of all studied variables and that other factors may be stronger regressors. The literature on CWP discusses the role of peripheral factors, in addition to the role of central and psychological mechanisms, in the initiation and perpetuation of CWP. Our results also agree with our previous findings that suggest a low level of interaction between ISI and other factors/symptoms in patients with chronic pain (15).
The results of the multivariate analysis, to some extent, support other prospective studies that suggest that insomnia is a strong predictor of CWP (8, 9, 22). In a 17-year follow-up study, Nitter et al. found that that non-specific health complaints and impaired sleep predict an unfavourable course of pain, especially transition from CRP to CWP (9). Possible explanations for this discrepancy with respect to the importance of sleep problems could be the different designs (cross-sectional vs longitudinal) and the fact that the majority of these studies evaluated sleep problems with only single items instead of trying to catch clinical insomnia. We used a well-validated self-reported instrument (i.e. the ISI) to identify clinically significant insomnia and not just general sleep problems (39).
This study has some limitations. First, the cross-sectional design is unable to establish causal relationships. A long-term longitudinal design is necessary in order to explore the causal links between spreading of pain and insomnia as well as other variables. In addition, self-reports of insomnia and the other variables under investigation (e.g. pain aspects and psychological distress) may be affected by recall bias. However, well-validated scales were used to assess these variables. Finally, we did not explore the potential role of pharmacological treatment on the relationship between spreading of pain and insomnia and the other variables investigated.
Acknowledging these caveats, we found that higher levels of a variety of factors are related in higher levels of spreading of chronic pain. This study suggests that a large part of the association between ISI and spreading of pain can be attributed to differences in sex, pain interference, pain duration, and anxiety. Nevertheless, an independent association between spreading of chronic pain and insomnia remains. Thus, it is reasonable to assume that sufficient sleep may have a protective role against pain. Sleep is associated with deactivation of the pain matrix in parallel with deactivation of the ascending arousal system (40). An important clinical implication is that a combination of reductions in pain interference, anxiety, and insomnia might be part of a chronic pain intervention; a strategy that might prevent worsening of pain with respect to spatial distribution. It is vital to understand whether this is an effective approach, since CWP and spreading of pain are associated with prominent negative implications. Future studies should further examine the role of insomnia, pain, and psychological aspects in relation to peripheral tissue mechanisms, and alterations in nociceptors and the central nervous system.
The authors acknowledge research nurse Eva-Britt Lind for her valuable help. The study was supported by grants from the Vårdal Foundation (Rehsam) and AFA Insurance.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize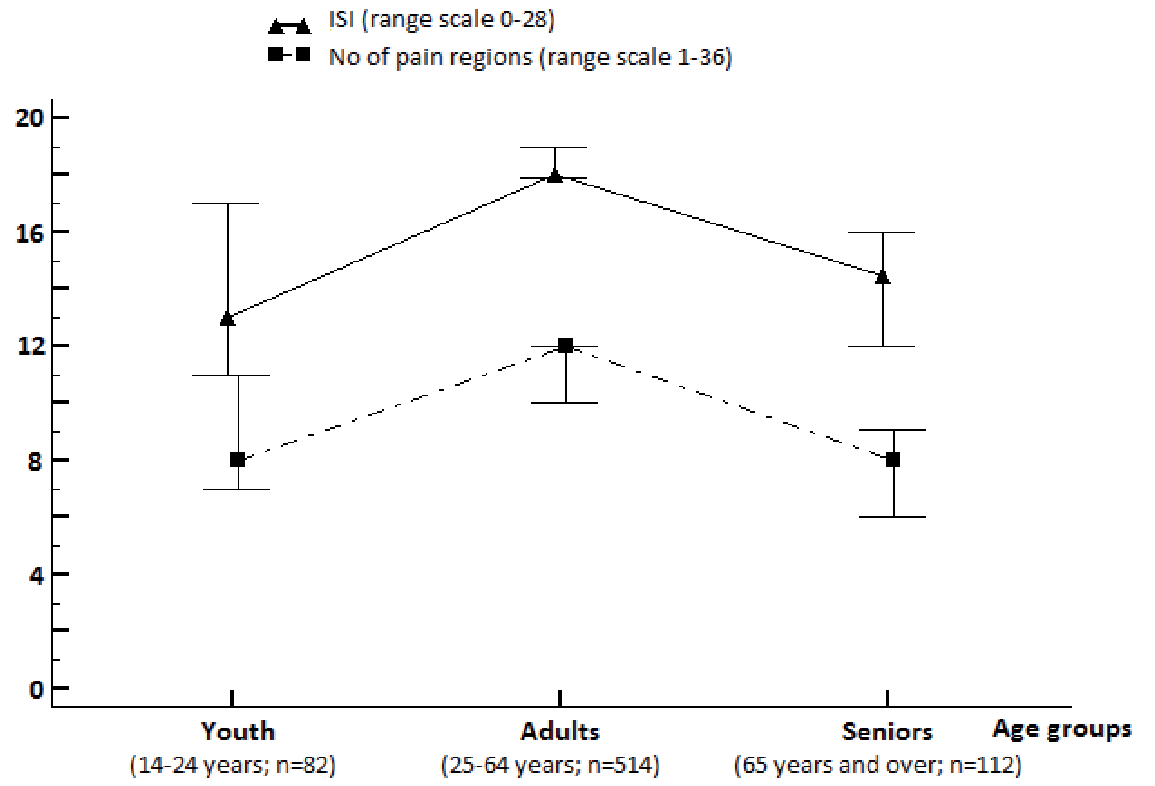 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize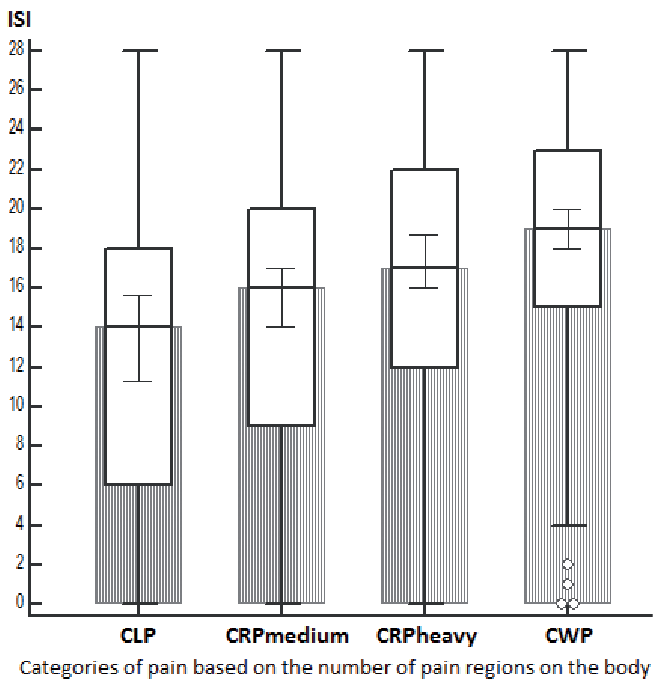 Click to show fullsize
Click to show fullsize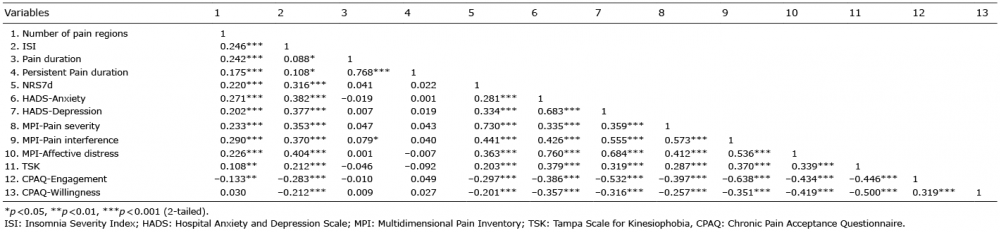 Click to show fullsize
Click to show fullsize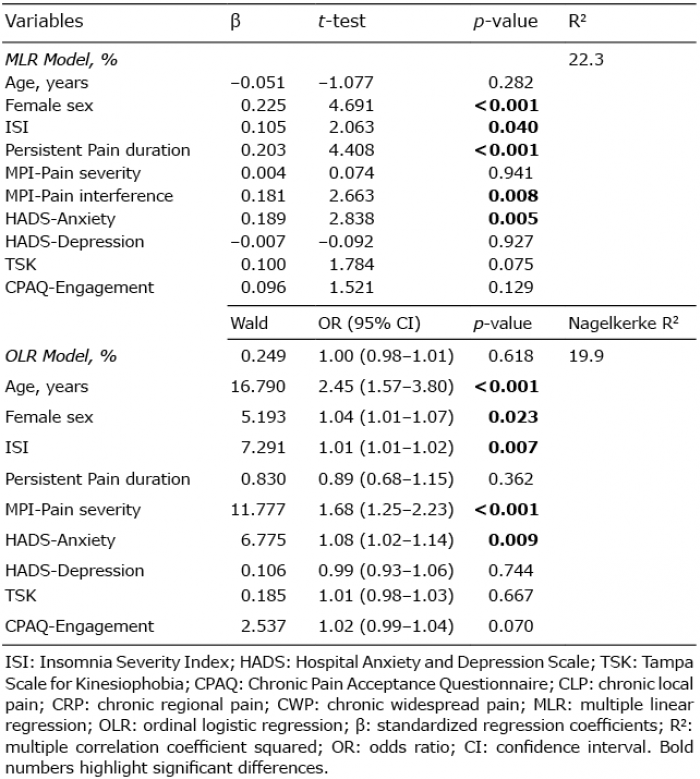 Click to show fullsize
Click to show fullsize