
From the 1Program in Health Sciences, Cardiology and Cardiovascular Sciences, 2Program in Respiratory Sciences, Universidade Federal do Rio Grande do Sul (UFRGS), 3Physiotherapy Course, Universidade Luterana do Brasil (ULBRA, Canoas/RS, 4Program in Sciences of Human Movement, UFRGS, 5Unit of Physical Therapy – Department of Intensive Medicine, Hospital de Clínicas de Porto Alegre (HCPA), 6Physiotherapy Course, UFRGS, Physiotherapy Service, HCPA, 7Graduate Program in Sciences of Human Movement, UFRGS, Graduate Program in Respiratory Sciences, UFRGS, 8School of Medicine (FAMED), UFRGS, Service of Intensive Medicine, HCPA, Porto Alegre/RS, Brazil. *These authors contributed equally to this work
Objective: To evaluate and compare the effects of neuromuscular electrical stimulation combined with conventional physical therapy on muscle thickness in critically ill patients. Design: Double-blind, randomized controlled trial.
Patients: Twenty-five patients participated in the study.
Methods: Patients on mechanical ventilation for 24–48 h were randomized to an intervention group (neuromuscular electrical stimulation + conventional physical therapy) or a conventional group (sham neuromuscular electrical stimulation + conventional physical therapy). Primary outcome was thickness of the rectus abdominis and chest muscles, determined on cross-sectional ultrasound images before and after the intervention.
Results: Eleven patients were included in the intervention group and 14 in the conventional group. After neuromuscular electrical stimulation, rectus abdominis muscle thickness and chest muscle thickness were preserved in the intervention group, whereas there was a significant reduction in thickness in the conventional group, with a significant difference between groups. There was a significant difference between groups in length of stay in the intensive care unit, with shorter length of stay in the intervention group.
Conclusion: There was no change in rectus abdominis and chest muscle thickness in the intervention group. A significant decrease was found in these measures in the conventional group.
Key words: electrical stimulation; muscular atrophy; intensive care unit.
Accepted Sep 13, 2016; Epub ahead of print Dec 8, 2016
J Rehabil Med 2017; 49: 40–48
Correspondence address: Ana M Dall’Acqua, P Graduate Program in Health Sciences: Cardiology and Cardiovascular Sciences, Universidade Federal do Rio Grande do Sul (UFRGS), 95555-000 Capão da Canoa, Brazil. E-mail: aninhadallacqua@hotmail.com
Intensive care units (ICUs) focus on treating critically ill patients. The mortality rate in these units in Brazil ranges from 5.4% to 33% (1, 2). According to the 2nd Brazilian Census of ICUs, the mean length of ICU stay ranges from 1 to 6 days (3) and, according to Williams et al. (4), the worldwide mean length of ICU stay is 5.3 days.
Seriously ill patients are often exposed to prolonged immobilization, which contributes to the development of neuromuscular complications (5, 6). Patients who stay in bed for long periods of time are prone to develop skeletal muscle weakness, leading to muscle atrophy and a loss of 3–11% of muscle mass in the first 3 weeks of immobilization (7). Such loss of muscle mass and muscle weakness are caused by acquired myopathy, polyneuropathy, or a combination of both (8). The development of polyneuropathy worsens the functional status of ICU patients, affecting 25–100% of patients ventilated for more than 7 days (9), with a prevalence of 58–96% of ICU patients (10). Two large studies evaluated survivors of acute respiratory distress syndrome at 3, 6 and 12 months and at 2, 3, 4 and 5 years after discharge from the ICU, and concluded that these patients have persistent functional disability 1 year after discharge from the ICU, and that most patients have extrapulmonary conditions, with muscle weakness and loss of muscle mass being most prominent (11, 12).
Neuromuscular electrical stimulation (NMES) is effective in the treatment of deficient muscles (13, 14). NMES is able to preserve muscle protein synthesis and prevent muscle atrophy during prolonged immobilization (15). Recently, NMES has been used to treat polyneuropathy in ICUs. This technique does not require active cooperation of the patient, and has a beneficial acute systemic effect on skeletal muscle microcirculation (16), offering structural and functional advantages to critically ill patients. Studies involving critically ill patients with chronic conditions, such as congestive heart failure and chronic respiratory failure, have suggested that NMES is safe and effective, improving peripheral (17, 18) and respiratory muscle strength in these patients (19–22).
Muscle cross-sectional area and/or thickness are strongly associated with force-generation capacity. However, few studies have been conducted in ICUs, especially involving trunk muscles, such as abdominal and chest muscles. Studies on NMES have suggested that this technique is useful in medical practice, with the purpose of preventing or decreasing loss of muscle mass and peripheral muscle atrophy in this population (23, 24). We could not find reports of its benefits in core muscle groups, such as the ones investigated in our study, as we know that loss of muscle mass does not affect only peripheral muscles. There is also mass loss in respiratory muscles, especially when patients cannot move and receive invasive mechanical ventilation (IMV). In these cases, the pectoralis major and the abdominal muscle have their alterations evaluated because they participate in the respiratory mechanism. To date, we could not find any descriptions of these alterations in the literature. Therefore, the main objective of the present study was to evaluate the effects of NMES combined with conventional physical therapy on rectus abdominis and chest muscle thickness compared with sham NMES combined with conventional physical therapy in patients receiving IMV.
This study was conducted in accordance with the principles of the Declaration of Helsinki and Good Clinical Practice. The procedures were performed in compliance with Resolution No. 466/12 of the Brazilian National Health Council. The study was approved by the research ethics committee of Hospital de Clínicas de Porto Alegre (HCPA No. 353.996). The trial is registered at ClinicalTrials.gov (NCT 02298114). The patients’ legal guardians signed an informed consent form.
A double-blind study (for outcome assessors and patients), with a per-protocol analysis, was conducted from August 2013 to August 2014 at the HCPA ICU. Eligible participants were all patients (both female and male, aged ≥ 18 years) who had been hospitalized for no longer than 15 days and had received at least 24 h of IMV. Exclusion criteria were: patients with neuromuscular diseases, such as stroke, multiple sclerosis, amyotrophic lateral sclerosis, myasthenia gravis, and Guillain-Barré syndrome, associated with motor deficits. In addition, patients were excluded if they: (i) were extubated within 48 h after inclusion in the study; (ii) had complications during the protocol, such as pneumothorax; (iii) had prolonged weaning (failed 3 spontaneous breathing trials); (iv) had a body mass index (BMI) > 35 kg/m2; (v) had a pacemaker; (vi) had haemodynamic instability (noradrenaline > 0.5 µg/kg/min for a mean arterial pressure > 60 mmHg) with a history of epilepsy or postoperatively with abdominal or chest incision; and (vii) used neuromuscular blockers for 2 or more consecutive days.
An assessor searched for potential trial participants via the HCPA’s computerized system. Patients’ electronic medical records were reviewed for identification data, medical diagnosis, and current medical conditions to assess patients for eligibility. The legal guardian of each eligible patient was approached for study enrollment, and those who agreed to participate were asked to sign the informed consent form.
A randomization sequence was created using the website www.randomization.com, with a 1:1 allocation ratio using blocks of 10 patients. To ensure confidentiality of the randomization sequence, it was generated by a blinded assessor who was contacted via telephone only after the participant had been included in the study and was ready to start the protocol.
Patients were randomly assigned to receive either NMES + conventional physical therapy (intervention group) or sham NMES + conventional physical therapy (conventional group). The NMES group received NMES for 30 min once a day + conventional physical therapy, whereas the conventional group received sham NMES for 30 min once a day + conventional physical therapy. The protocol was interrupted on day 7, when the patient was extubated, or if the patient died (whichever occurred first). NMES was administered in both groups by previously trained professionals for procedure standardization. Conventional physical therapy in both groups was performed by ICU professionals twice a day.
The primary outcome was the difference in rectus abdominis and chest muscle thickness of the dominant side from initial to final assessment between groups. Secondary outcomes included changes in diaphragm muscle thickness, and inhaling and exhaling diaphragmatic motion. Length of stay in the ICU and in the hospital, duration of IMV, successful extubation and death were also assessed.
After inclusion in the trial and before starting the protocol, all participants underwent ultrasound of the chest and abdominal muscles for assessment of muscle thickness and diaphragmatic motion. Ultrasound examination was performed on 2 different occasions: on the first day of participation in the study (24–48 h of IMV) and on day 7 of IMV or 24 h after extubation.
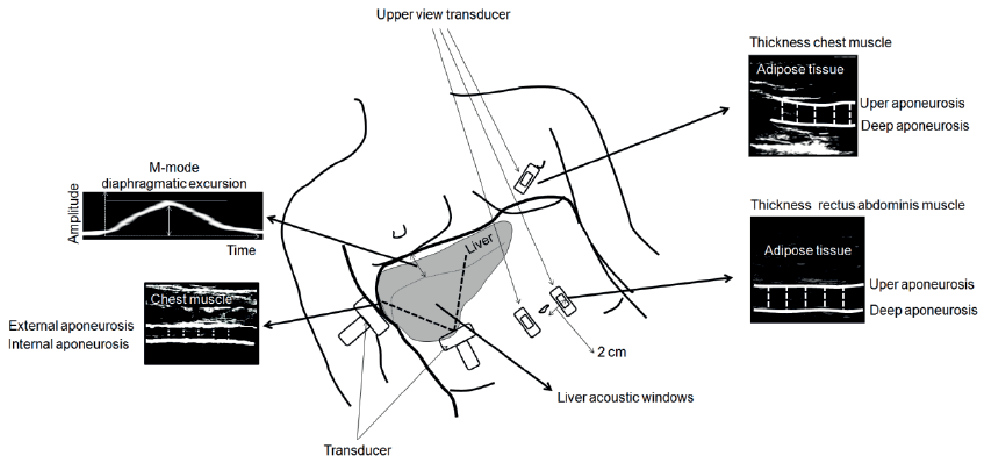
Muscle thickness was determined on cross-sectional ultrasound images. With the patient lying supine and the head of the bed elevated at 30°, real-time B-mode scanning was performed using a 3.5-mm, 7.5 MHz linear-array transducer (Sonosite®, Washington, DC, USA). The scanning head was coated with water-soluble transmission gel to provide acoustic contact without depressing the dermal surface. The sites for image acquisition were determined using anatomical parameters reported in the literature (25). To assess the chest muscle, the midpoint of the sternum was determined. Starting at this point, the transducer was positioned obliquely toward the nipple line, seeking to reach an area of larger muscle belly. To assess the rectus abdominis muscle, we obtained the measure at a lateral distance of 2 cm from the umbilicus.
After the sites were marked on the skin, a cross-sectional image was acquired, which included the chest and rectus abdominis muscles. Because the transducer is 3.5 cm long, muscle thickness was adopted as the preferred measure, as it was not always possible to capture the total area of the rectus abdominis muscles. Thus, muscle thickness was determined based on measurements performed between the inner edge of the upper and lower aponeuroses of the chest and rectus abdominis muscles. The specific measure of the rectus abdominis muscles was collected during maximal inspiration, because there is a dynamic change in the thickness of the muscle due to the movement of the abdomen during breathing. Five measurements were taken based on each image. A mean measurement was determined to establish the muscle thickness.
For ultrasound-based measurement of diaphragmatic muscle thickness, the patient was placed in the supine position. The transducer was positioned perpendicularly to the diaphragm in the intercostal space over the tenth rib on the anterior axillary line, the image was acquired and the thickness was measured at the end of inspiration.
For assessment of diaphragmatic motion, the ultrasound transducer was positioned through the anatomical window provided by the liver between the mid-clavicular position and the anterior axillary line towards the skull. Thus, the transducer was placed in a medial, cranial, and dorsal position, making it possible for the ultrasound beam to reach the posterior third of the diaphragm (26, 27).
Inhalation and exhalation diaphragmatic excursion was measured on M-mode ultrasound images. The inhalation excursion was determined by measuring the vertical height of the base of the beginning of inhalation up to the peak slope at the end of inhalation, and the exhalation excursion was determined by measuring the vertical height of the inhalation peak until return to the base.
The muscle ultrasound examination was repeatedly assessed on 2 separate days, based on 10 images for each region. The intraclass correlation coefficient for the test-retest muscle thickness measurements was r = 0.996 for the chest muscle, r = 0.998 for the rectus abdominis, r = 0.972 for the diaphragmatic muscle thickness, and r = 0.985 for the diaphragmatic excursion. All ultrasound examinations were performed by the same highly experienced professional (4 years), who was blinded to group assignment. All ultrasound measurements were expressed in cm. Fig. 1 shows a representative transducer position.
Fig. 1. Data collection environment.
In the intervention group, NMES was performed using a 4-channel Neurodyn II (Ibramed®, São Paulo, SP, Brazil). Only the dominant side of each patient was considered for analysis, and hairy body areas were shaved, as necessary. The negative electrodes were placed in the motor points of the following muscles: chest muscles (pectoralis major muscle fibres) and rectus abdominis muscles bilaterally. A second (positive) electrode was positioned distally to the first, at a site close to the muscle that was being electrically stimulated, totalling 1 channel with 2 electrodes for each muscle (Fig. 2).
Fig. 2. Representative image of the positioning of electrodes on the straight muscles of the abdomen and chest to perform the protocol.
Each NMES session lasted 30 min. One minute was added every 2 days of administration. The following parameters were used: 50 Hz frequency, pulse duration 300 ms, rise time 1 s, stimulus time (ON) 3 s, decay time 1 s, and relaxation time (OFF) 10 s. Intensity was increased until muscle contraction was visible or could be identified through palpation. In conscious patients, intensity was adjusted according to their tolerance (23, 24).
The conventional group received sham NMES following the same protocol applied to the intervention group. The procedure was blinded; however, the intensity was adjusted at a sensory level, i.e. without visible or palpable muscle contractions. The standard maximum intensity in this group was 5 mA.
Conventional (chest and motor) physical therapy was administered in both groups by ICU professionals twice daily for 30 min. The protocol consisted of functional-diagonal movements based on the proprioceptive neuromuscular facilitation (PNF) stretching technique for the upper and lower extremities (2 sets of 10 repetitions per set of each diagonal movement bilaterally). At first, physical therapy was administered in a passive manner if the patient was sedated. The exercises evolved to assisted movements and active resisted movements according to the patient’s cooperation. Manual bronchial hygiene techniques were performed, such as chest compression-vibrations, manoeuvres with an Ambu bag (bag-squeezing), and suction of secretions when necessary.
The protocols were initiated after the baseline evaluation within the first 48 h of IMV. During protocol administration, the following parameters were monitored in both groups: heart rate, respiratory rate, mean blood pressure, peripheral oxygen saturation, and ventilatory frequency.
On day 7 of the protocol or upon extubation (whichever occurred first), all patients were assessed again by ultrasound and continued to receive only conventional (chest and motor) physical therapy provided by the ICU professionals until ICU discharge.
The sample size calculation was based on a pilot study of 10 patients for the variable cross-sectional area of abdominal and chest muscle thickness using the statistical program Winpepi. These measures were adjusted using a delta value, defined as the measures of final muscle thickness subtracted from the baseline measures divided by the number of days the participant remained in the protocol. For an effect size of 0.7 standard deviations (SD) between the 2 groups, with a 5% significance level and power of 80%, a sample size of 18 patients (9 patients per group) was required.
Data storage, arrangement, and maintenance were performed using a MS Excel 2007 spreadsheet. Data were expressed as mean and SD. Student’s t-test for independent samples was used to compare the means, and the χ2 test or Fisher’s exact (when more than 25% of the cells had the expected frequency < 5) were used to compare means between groups for qualitative data. The Shapiro–Wilk test was used to test the normality of distribution, and Levene’s test was used to assess homogeneity of variance for all group comparisons. A generalized estimating equations (GEE) model with Bonferroni’s correction was used to assess intra- and inter-group interaction for primary and secondary outcomes. In the GEE model, possible confounding factors were controlled by adjusting for septic and non-septic patients, Acute Physiology and Chronic Health Disease Classification System II (APACHE II) score > 25 and < 25 end ICU stay. Statistical analysis was performed using SPSS, version 20.0. The level of significance was set at 5% (p ≤ 0.05).
From August 2013 to August 2014, 1,321 patients were screened for eligibility. Of these, 1,283 were not eligible for the study. Thirty-eight patients were randomized to the intervention group (n = 19) and to the conventional group (n = 19). Eleven patients in the intervention group and 14 in the conventional group completed the protocol and were included in the final analysis. Fig. 3 shows the flow of participants, including losses to follow-up and exclusions after randomization.
Fig. 3. Study flowchart. Encephalic vascular accident (EVA)
Table I shows the characteristics of the study sample.
Table I. Sample characteristics
Table II describes the comparison between the baseline measurements of muscle thickness between the groups, showing that there was no statistical difference between the groups in terms of measurements of chest and abdominal muscles at baseline.
The intensity in the intervention group caused palpable or visible contraction in 100% of patients. The mean stimulation on the major pectoralis was 53 mA (SD 15), whereas it was 68 mA (SD 18) on the abdominal muscle. In the control group, which received placebo NMES, the stimulation for all patients was up to 5 mA, not causing visible or palpable contraction in the patients. During administration of NMES, there were no complications or significant changes in vital signs.
Table II. Comparison of baseline muscle thickness between groups
There was a statistically significant difference between the intervention and conventional groups in abdominal and chest muscle thickness (p > 0.001). Considering the comparison between the initial and final assessment within each group, there was no change in muscle mass in the intervention group, whereas there was a statistically significant decrease in these measures in the conventional group (p > 0.001). Even after adjusting for potential confounders (sepsis and APACHE II), the results remained significant (p < 0.001) (Table III and Fig. 4). The effect size for chest muscle thickness and abdominal muscle thickness was 1 and 0.9 SD, respectively.
Table III. Comparison of muscle thickness between groups
Fig. 4. Individual behaviour of the thickness of chest and abdominal muscles at baseline and at the end of the study for each group. (A) Variation in chest muscle thickness (CT) in the intervention group. (B) Variation in abdominal muscle thickness (AT) in the intervention group. (C) Variation of CT in the control group. (D) Variation of AT in the control group.
There was a significant difference in length of ICU stay, which was shorter in the intervention group than in the conventional group (p = 0.045). There was no statistically significant difference in diaphragm muscle thickness or inhaling and exhaling diaphragmatic motion between the 2 groups. Likewise, the comparison between baseline and end evaluation within each group showed no significant differences. Even after adjusting for APACHE II and sepsis, the values remained non-significant (p > 0.05) (Table IV). The effect size for inhaling diaphragmatic motion, exhaling diaphragmatic motion and diaphragm muscle thickness was 0.7, 0.6, and 0.02 SD, respectively.
Table IV. Comparison of diaphragmatic motion and thickness between groups
This study demonstrated that intervention using NMES combined with conventional physical therapy preserved the chest and rectus abdominis muscle thickness in critically ill patients on IMV. This finding is consistent with those reported by Gerovasili et al. (28), who evaluated 26 individuals, divided into control and intervention groups, and found that patients undergoing NMES applied to the quadriceps muscle as well as the control group showed decreased muscle mass. However, this decrease was significantly lower in the NMES group, suggesting that NMES may have a protective effect against muscle wasting. Nevertheless, Poulsen et al. (29) applied NMES to the quadriceps muscle, using the contralateral limb as a control, and found no difference in muscle mass between the stimulated and non-stimulated side, as assessed by computed tomography. Gruther et al. (30) used ultrasound to investigate the effects of NMES on the thickness of the quadriceps muscle during the acute phase (less than 7 days of hospitalization) and in the long term (more than 14 days after admission) in critically ill patients. The authors found increased thickness only for long-term patients who started NMES after 2 weeks of ICU admission. However, there was no increased thickness in acute patients. This is in agreement with the present findings, which demonstrated no change in muscle mass even when the NMES protocol was started early (up to 48 h of ICU admission).
As for the secondary outcomes, there was no statistically significant difference between groups in diaphragm thickness or inhaling and exhaling diaphragmatic motion. There was a significant difference only in the number of days of ICU stay, with a shorter stay in the intervention group compared with the conventional group. The implementation of early mobilization programmes, which is the type of intervention proposed in our study, may lead to a reduction in length of ICU stay (31). The use of IMV may also induce diaphragmatic dysfunction, reducing the patients’ force generation capacity and mobility (32, 33). Martin et al. (34) used physical therapy to assess the improvement in peripheral and respiratory muscle strength and functional status of mechanically ventilated patients, and found a positive correlation between upper limb strength and ventilation weaning time. However, in our study, there was no statistically significant difference regarding days of IMV and re-intubation rate. In a previous study conducted by our research group, we found increased inspiratory and expiratory muscle strength by administering NMES using Russian current in the rectus abdominis and abdominal oblique muscle in inpatients with COPD compared with the control group (19).
The most prevalent ICU admission diagnosis in our study was sepsis (60%). Studies conducted in ICUs involving the use of NMES have demonstrated that the most common diagnoses on admission are sepsis, COPD, and trauma (28, 30, 35). Sepsis is known to generate a reaction of protein hypercatabolism in the muscles, contributing to loss of muscle mass. Loss of muscle mass is partially attributed to sepsis and to multiple organ dysfunction syndrome, use of drugs, such as neuromuscular blockers, and immobilization (36). Therefore, we adjusted the outcomes by dividing our patients into septic and non-septic, and the results were statistically significant even after the adjustment. The re-intubation rate in the intervention group was 25% against 38% in the conventional group. Routsi et al. (37) applied NMES to the quadriceps and peroneus longus muscles of critically ill patients and found reduced weaning time in the intervention group. However, in agreement with our findings, there was no significant difference in the re-intubation rate between groups. Conversely, a study conducted by Abu-Khaber et al. (38), evaluating the prevention of muscle weakness and facilitation of weaning from mechanical ventilation in critically ill patients using NMES in the quadriceps muscle and starting the protocol within the first 2 days of mechanical ventilation, reported unclear conclusions about the role of NMES in facilitating the weaning process. In addition, the number of days on mechanical ventilation was lower in the NMES group compared with sham stimulation, but the statistical significance level was very low (p = 0.048).
In our study, APACHE II score was similar in both groups. In a systematic review on the use of NMES in intensive care, Parry et al. (39) concluded that patients with an APACHE II score greater than 20 did not benefit from NMES to preserve muscle mass. Conversely, individuals with an APACHE II score lower than 16 showed better muscle response to NMES. Such negative results may be linked to the correlation between NMES intensity and disease severity, because the excitability of muscle tissue in this condition may induce dysfunctions of the muscle membrane compromising its contraction and increasing catabolism, thus enhancing loss of muscle mass (29). However, our findings demonstrated positive effects in terms of preservation of muscle mass, even after adjusting the values for patients with APACHE II score > 25 and < 25, which suggests that NMES may prevent loss of muscle mass even in patients with high APACHE II score.
The mean NMES duration in the current study was 5 days in the intervention group. In comparison with our study, the duration of treatment was significantly longer (in days) in previous studies using NMES in the peripheral muscles of critically ill patients; therefore, these studies showed positive results regarding muscle mass gain (28, 29). The study by Routsi et al. (37) used 55 min/day of NMES, demonstrating positive results in terms of muscle mass and development of polyneuropathy. In our study, we initially used 30 min of NMES in the rectus abdominis and chest muscles, adding 1 min every 2 days, and found positive results in terms of muscle thickness. Such findings suggest that the initial daily use of 30 min of NMES benefits critically ill patients.
The parameters used in the NMES protocol of our study were designed and established by the research team with great theoretical knowledge about the principles of NMES. Therefore, we were able to achieve the desired muscle fibre recruitment in these muscle groups, with the purpose of recruiting fast and slow twitch fibres, based on the positive results described previously in the literature, using parameters very similar to the ones used in our study, in order to increase peripheral muscle strength and the potential benefits related to the preservation of the muscle mass of critically ill patients (23, 24, 39).
We decided to use ultrasound to evaluate muscle and diaphragmatic behaviour in the administration of NMES because it is a valuable tool in the management of ICU patients. Ultrasound examination makes it possible to quantify diaphragmatic motion and accurately assess muscle atrophy (40). The choice of this tool appears to be more accurate for muscle assessment in ICU patients (28) and overcomes many of the problems associated with anthropometric and body composition measures, such as oedema, which may be a source of bias when assessing muscle thickness (30). Currently, ultrasound is the most reliable method and its validity is well established in intensive care (39).
Our findings are limited by a relatively small number of patients who underwent NMES sessions. Furthermore, sedation and the use of vasopressor drugs might have affected microcirculation in these patients.
Further studies with larger samples might provide subgroup analysis to identify the potential beneficial effects of NMES when applied to the muscles involved in respiratory mechanics in different populations, since the initial results of this approach are positive in the prevention of loss of muscle mass in these muscle groups.
In conclusion, there was no change in rectus abdominis and chest muscle thickness in critically ill patients in the intervention group (neuromuscular electrical stimulation+conventional physical therapy); however, we found a significant decrease in these measures in the conventional group (sham neuromuscular electrical stimulation + conventional physical therapy). In addition, the length of ICU stay was significantly shorter in the group receiving active NMES.
The authors would like to thank all of the physiotherapists, specialist nurses and physicians involved with recruitment and data collection. This study is supported by the research funding agencie Fundo de Incentivo à Pesquisa e Eventos (FIPE) do HCPA.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize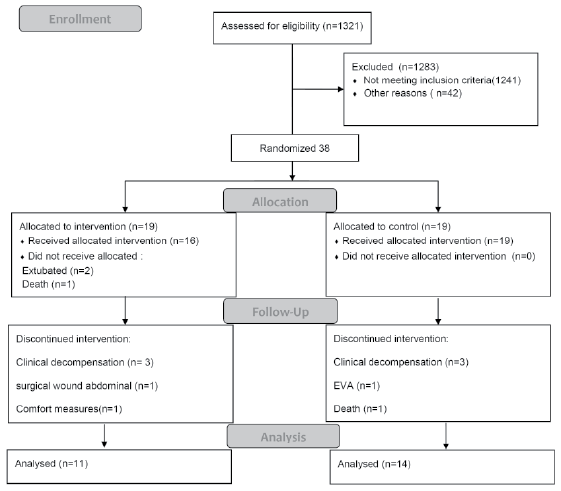 Click to show fullsize
Click to show fullsize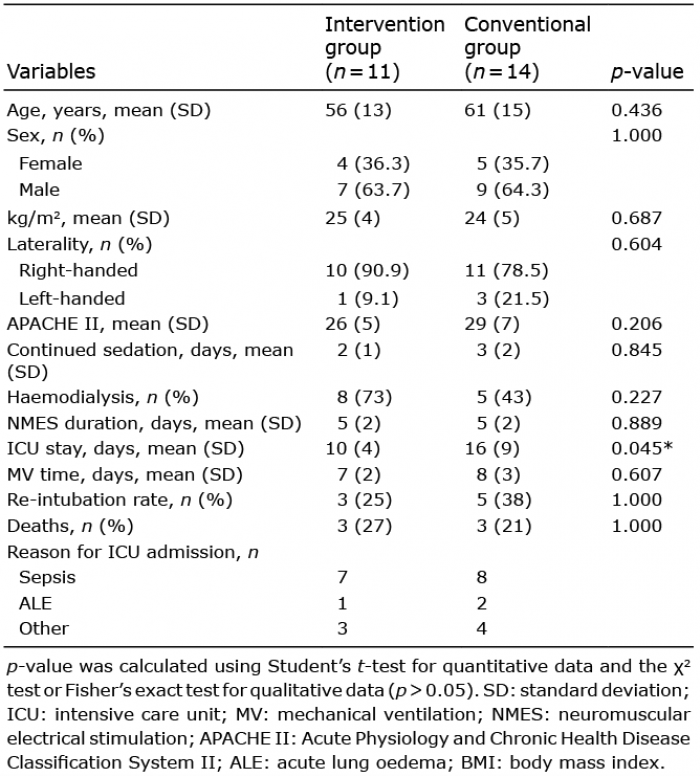 Click to show fullsize
Click to show fullsize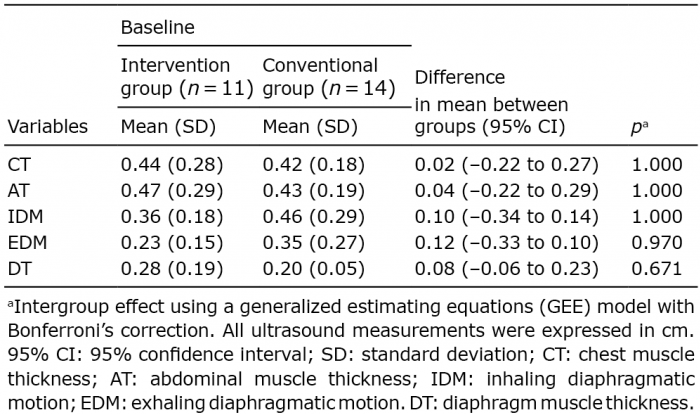 Click to show fullsize
Click to show fullsize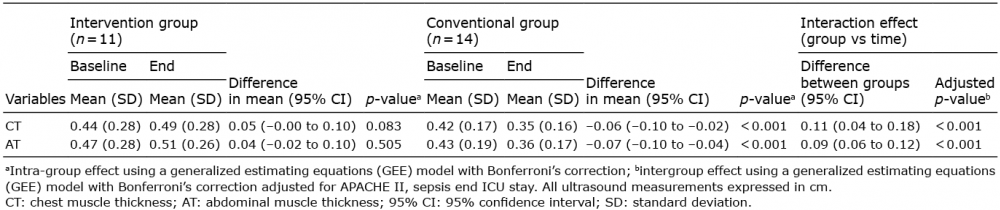 Click to show fullsize
Click to show fullsize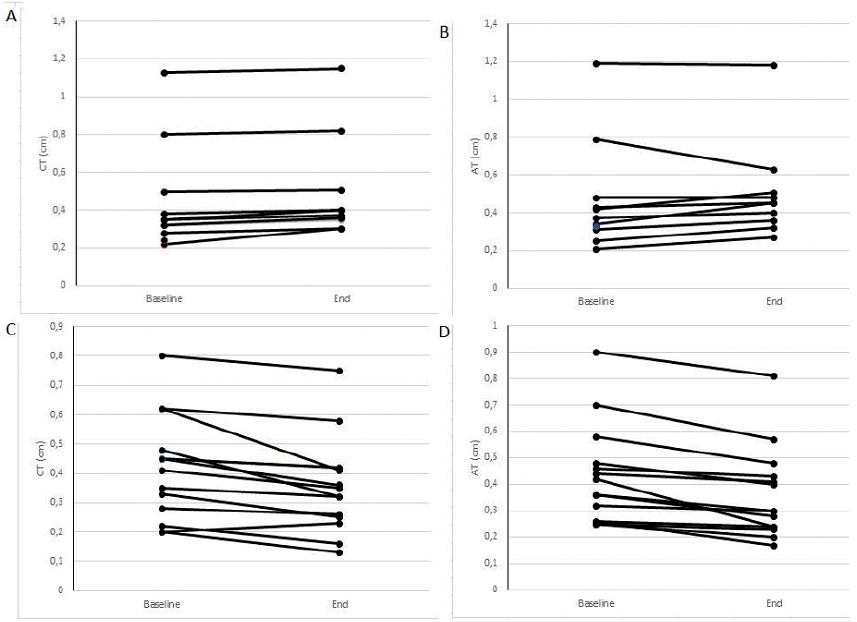 Click to show fullsize
Click to show fullsize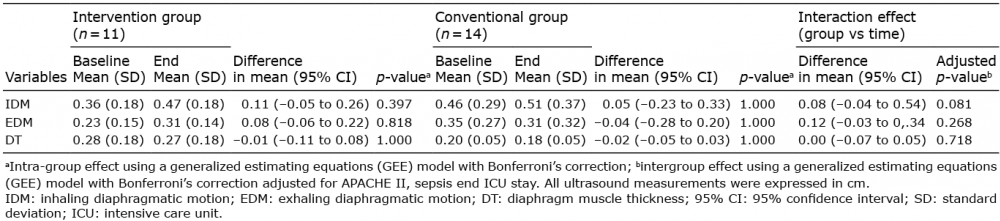 Click to show fullsize
Click to show fullsize