
From the Clinical Department of Rehabilitation Medicine and Department of Medicine and Health Sciences, Linköping University, Linköping, Sweden
Objective: To assess changes in body composition, body weight and resting metabolic rate in patients who received intrathecal baclofen therapy for spasticity.
Design: Prospective, longitudinal, quasi-experimental, with a pre/post design.
Patients: Twelve patients with spasticity, fulfilling study criteria, and due for pump implantation for intrathecal baclofen therapy, completed the study.
Methods: Data were obtained before, 6 months and 12 months after commencement of intrathecal baclofen therapy as regards body composition (by skinfold calliper), body weight, and resting metabolic rate (by resting oxygen consumption). Spasticity was assessed according to the Modified Ashworth Scale (MAS) and Penn Spasm Frequency Scale (PSFS).
Results: A reduction in spasticity according to MAS occurred. Mean fat body mass increased and mean lean body mass decreased. Mean body weight showed a non-significant increase and resting metabolic rate a non-significant decrease.
Conclusion: This explorative study indicates that unfavourable changes in body composition might occur after intrathecal baclofen therapy. Since obesity and increased fat body mass contribute to an increased cardiovascular risk, these findings may indicate a need for initiation of countermeasures, e.g. increased physical activity and/or dietary measures, in conjunction with intrathecal baclofen therapy. Further studies, including larger study samples and control groups, are needed to corroborate these findings.
Key words: intrathecal baclofen; body composition; cardiovascular risk; obesity.
Accepted Sep 21, 2016; Epub ahead of print Dec 8, 2016
J Rehabil Med 2017; 49: 36–39
Correspondence address: Richard Levi, Clinical Department of Rehabilitation Medicine and Department of Medicine and Health Sciences, Linköping University, SE-585 85 Linköping, Sweden. E-mail: richard.levi@regionostergotland.se
Spasticity is a phenomenon accompanying upper motor neurone lesions of various aetiologies, e.g. spinal cord injury (SCI), multiple sclerosis (MS), cerebral palsy (CP), and stroke (1). Various operational definitions have been suggested, and in recent years, a definition proposed by Pandyan et al. (2) has been preferred. According to this definition, spasticity is “disordered sensorimotor control, resulting from an upper motor neurone lesion, presenting as intermittent or sustained involuntary activation of muscles”.
Spasticity, as such, may be of some functional benefit to the patient, e.g. by improving sitting, standing, transferring, walking and performance of activities of daily living (ADL) (3). In addition, previous research on patients with spinal cord injury and spasticity indicates that the degree of spasticity correlates with beneficial indices of body composition, i.e. less fat body mass and more lean body mass (4). Thus, not all instances of spasticity should be treated.
Excessive spasticity, however, may become painful and/or disabling, by increasing the risk of contractures, pressure ulcers and injuries, as well as by hampering ADL. In all cases of excessive and/or rapidly increased spasticity, any underlying triggering condition should be sought and eliminated, as all kinds of nociceptive stimuli may have this effect, and as in many cases concomitant pain may be masked by sensory and/or cognitive impairment. Only in conjunction with treatment of triggers, if present, the spasticity as such should be targeted symptomatically.
Treatment includes regular/daily stretching and range-of-motion exercises, i.e. physical therapy, but this is often insufficient (5). Oral baclofen is then typically the drug of choice (6). Alternatively, in case of excessive focal spasticity, injections of botulinum toxin may be used (7). However, some cases of generalized or regional, disabling spasticity are refractory to oral and/or local treatment. Also, some patients experience unacceptable side-effects of oral baclofen, e.g. lethargy (6). In such cases, intrathecal administration of baclofen via an implantable pump system may be indicated. Complications of ITB therapy related to implantation (e.g. local infection) and technical mishaps (e.g. motor stall and catheter malfunction), have been reported previously (8, 9). In addition, several studies on ITB treatment in children have reported weight gain (10–12). If this also proves to be the case in adult populations, it may well be of clinical importance to consider, as many paralytic patients already have an increased risk of acquiring cardiovascular disease (CVD) (13). Furthermore, data related to the effects of baclofen on body weight are conflicting, as oral baclofen has been shown to yield weight gain as a side-effect, but on the contrary also has been used as a drug for weight reduction in obesity (14). In addition to an increased CVD risk due to chronic immobilization, an increased prevalence of obesity within, e.g. SCI populations (15, 16), has been reported. Such obesity may be masked by a simultaneous loss of lean body mass. A paralysed patient may thus be obese (increased fat mass), despite having a normal body weight and/or body mass index (17). As obesity is a modifiable CVD risk factor, increased diagnostic vigilance and a more proactive preventative and interventional stance may be called for. Thus, untoward changes in body composition in conjunction with ITB therapy for spasticity should be evaluated.
The aim of this study was to assess changes in body composition after initiation of ITB therapy for spasticity.
Patients were recruited consecutively from a regional waiting list of subjects due for pump implantation for ITB treatment of disabling spasticity. Inclusion criteria were: age 18 years or older; living in the southeast healthcare region in Sweden; patient subsequently underwent pump implantation. Patients due for pump re-implantation (i.e. who during the preceding 6 months prior to commencement of the study had received ITB treatment) were excluded.
The study received ethical approval from the regional ethical review board of Linköping (2012/181-31).
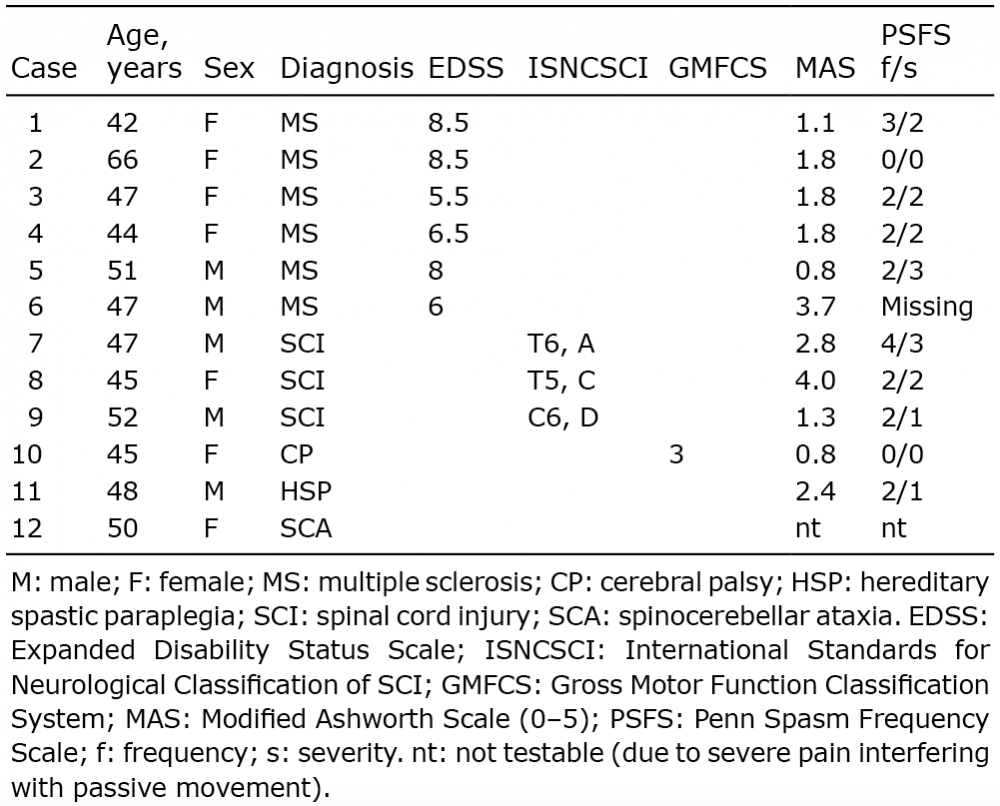
Patients eligible for participation in the study received oral and written information, and were asked for written consent. Those included in the study were assessed prior to pump implantation, and then again at 6 and 12 months post-implantation. Eighteen patients fulfilling the inclusion criteria were asked to participate. Five eligible patients declined participation and 1 patient was excluded while not tolerating the face mask necessary for resting metabolic rate (RMR) estimation. Thus, 12 patients completed the study. Their descriptors (age, sex, diagnosis, spasticity assessment at baseline, diagnosis-specific severity classification) are depicted in Table I. In this study, as patients served as their own reference, great care was placed on the application of identical measurement conditions at each data collection point.
Table I. Patient characteristics
Spasticity. Spasticity was assessed using the Modified Ashworth Scale (MAS) in the 0–5 version (18) and the Penn Spasm Frequency Scale (PSFS) (19), pre-implantation, and 6- and 12-months post-implantation. MAS was assessed for each individual, before and after treatment (12 months) in the same spastic muscles of the lower limbs and is presented as a mean value. Measurements were made by 2 physiotherapists working together, who had extensive training and experience in spasticity evaluation and treatment.
Body weight and body mass index. Body weight (kg) was measured by a calibrated scale adapted also for wheelchair users, in a standardized fashion. Body mass index was calculated based on registered weight and reported height.
Resting metabolic rate. RMR was estimated using a single portable equipment measuring resting oxygen consumption under standardized conditions (FitMate®) (20).
Body composition. Body composition was calculated based on anthropometry with a skinfold calliper (Slim Guide Caliper) (21, 22), according to a standardized procedure, including measurements of skinfold thickness over the triceps brachii, biceps brachii, subscapular region and abdominal region laterally, above the pelvis. Data collectors calibrated techniques in using the skinfold calliper before the study start.
Data was transformed, according to the Durnin-Womersley equation (23), to percentages of fat body mass. As body weight was recorded, relative and absolute lean body mass could also be calculated.
Due to the small study group and the non-normally distributed measures, data were analysed by non-parametric methods (SPSS statistics version 23). Wilcoxon matched-pairs test was used for assessment of pre-post differences. The significance level was set at p ≤ 0.05.
The effect of ITB therapy on spasticity in the study group is depicted in Table II. A reduction in spasticity, as measured by MAS, was found (p ≤ 0.01). Although not a focus of this study, the confirmation of spasticity reduction is relevant for subsequent interpretation of the primary study results.
Table II. Intrathecal baclofen effects on spasticity (n = 11)
A mean, relative and absolute, increase in fat body mass and decrease in lean body mass was found (p ≤ 0.05 and p ≤ 0.01 respectively). By contrast, no change occurred as regards mean body weight or RMR, although a trend was seen towards an increase in body weight and reduction in RMR. See Table III and Figs 1–3 for details.
Table III. Changes in metabolic indices as calculated by Wilcoxon signed-rank test. Test of significance refer to comparison between baseline and 6 and 12 months. No statistically significant differences were found between 6 months and 12 months (n = 12)
Fig. 1. Change in body weight (BW), fat body mass (FBM) and lean body mass (LBM) comparing baseline with 12 months post implantation (kg).
Fig. 2. Change in fat body mass (kg) from baseline to 6 and 12 months after pump implantation.
Fig. 3. Change in lean body mass (kg) from baseline to 6 and 12 months after pump implantation.
The study shows an increase in fat body mass and a decrease in lean body mass during the first year after commencement of ITB therapy, changes in body composition clearly exceeding the expected spontaneous changes in body composition in SCI and MS populations found in previous studies (24, 25). Weight gain and/or increase in fat body mass as a side-effect of ITB therapy has been reported in paediatric populations (10–12), but has not hitherto been studied in adults. As the required dose is vastly smaller in ITB compared with that of oral medication, any direct effects of the intrathecally delivered drug on metabolism is considered highly unlikely. Instead we hypothesize that the effect is mediated through the diminution of muscular hyperactivity.
The finding of untoward changes in body composition in the presence of stable levels of RMR is noteworthy. We find it likely that the significant changes in body composition thus primarily were due to a decrease in activity-related/activity-triggered spasticity, rather than due to any changes in resting-state spasticity. Such spasticity reduction may lead to both a decrease in lean body mass (due to decreased muscle activity) and to an increase in fat body mass (due to decreased energy expenditure) in the absence of any changes in RMR.
This study is limited by the relatively small study group, the diversity of diagnoses and the choice of measure for body composition, as skinfold calliper measurements have not been validated specifically for individual diagnoses. Thus, the results should be interpreted as hypothesis generating, in view of further research, with larger study populations and control groups.
In conclusion, this explorative study lends support to the impression that ITB therapy may generate untoward effects on body composition, with an increased fat body mass and a decreased lean body mass. Findings may be clinically relevant, as patient groups eligible for ITB typically already have an increased CVD risk and an undesirable tendency towards obesity, thus necessitating further caloric restrictions and/or exercise prescription in conjunction with this treatment.
Marie Lannesand, PT, and Eva Härkegård, PT, for valuable assistance in data collection. Madeleine Wikström, RN, MSc, for coordinating patients and data collection.


 Click to show fullsize
Click to show fullsize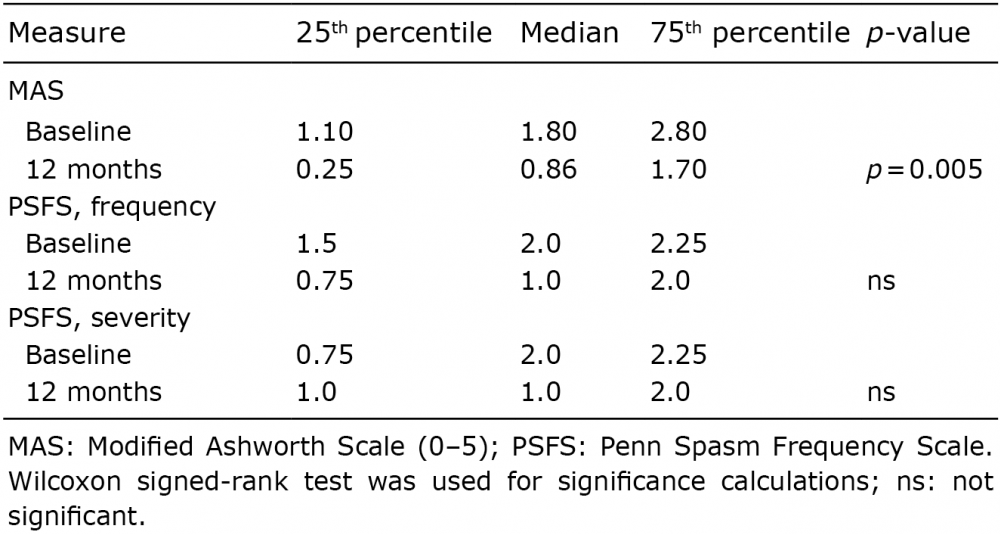 Click to show fullsize
Click to show fullsize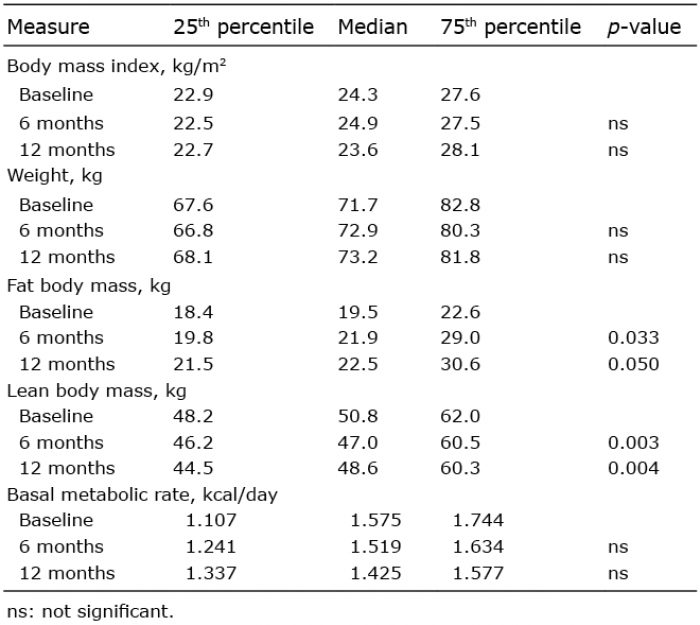 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize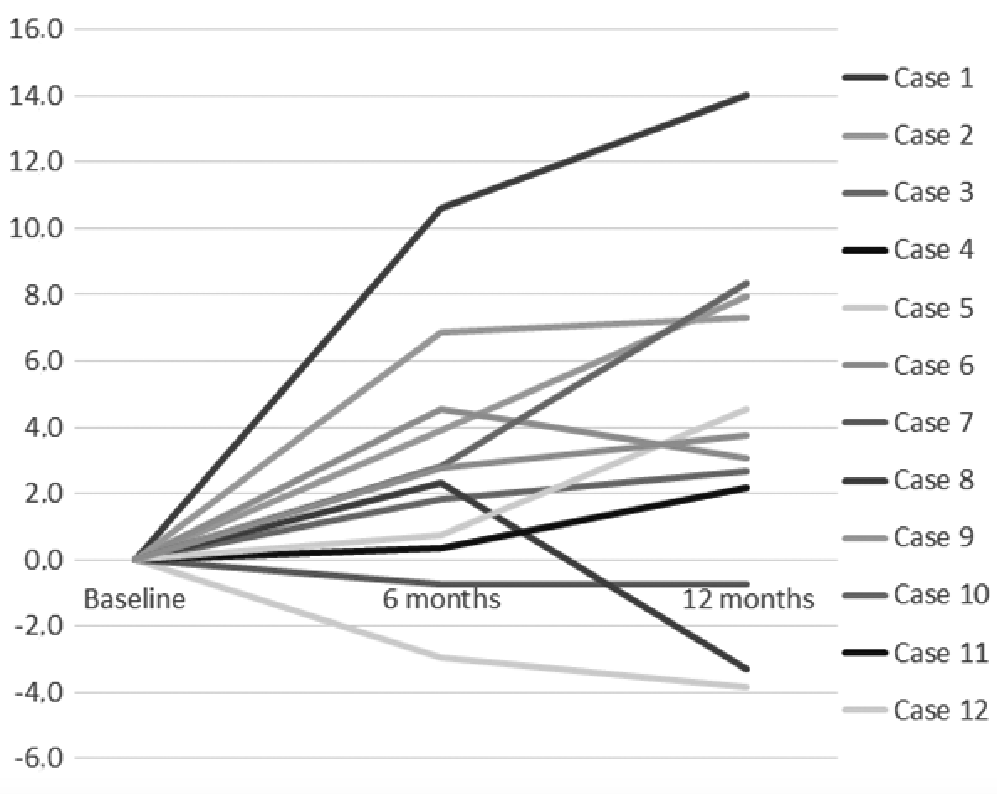 Click to show fullsize
Click to show fullsize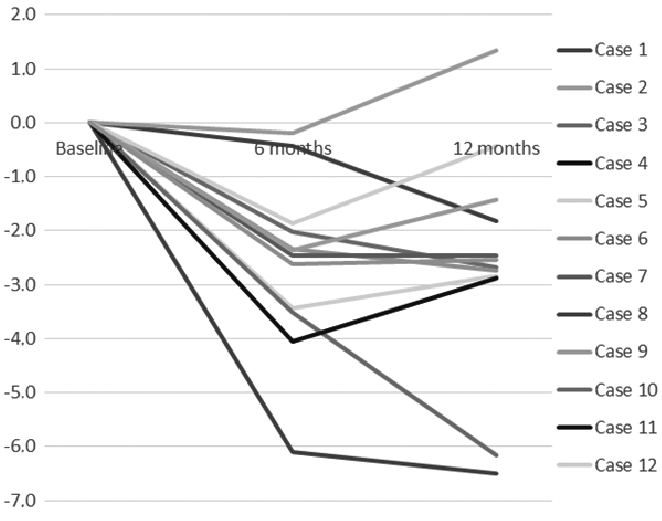 Click to show fullsize
Click to show fullsize