
From the 1Rehabilitation Center Kliniken Valens, Valens and 2Department of Geriatrics, Inselspital, University of Bern Hospital, Bern, Switzerland. *These authors contributed equally to this publication.
Objective: To evaluate patient characteristics predicting living at home after geriatric rehabilitation.
Design: Prospective cohort study.
Patients: A total of 210 patients aged 65 years or older receiving inpatient rehabilitation.
Methods: Candidate predictors evaluated during rehabilitation were: age, vulnerability (Vulnerable Elders Survey), multimorbidity (Cumulative Illness Rating Scale), cognition (Mini-Mental State Examination), depression (Hospital Anxiety and Depression Scale), living alone, previous independence in activities of daily living, fall risk, and mobility at discharge (Timed Up and Go test). Multiple imputation data-sets, bivariate and multiple regression were used to build a predictive model for living at home, which was evaluated at 3-month follow-up.
Results: A total of 210 patients (mean age 76.0 years, 46.2% women) were included in the study. Of these, 87.6% had been admitted to geriatric rehabilitation directly from acute hospital care. Follow-up was complete in 75.2% of patients. The strongest predictor for living at home was better mobility at discharge (Timed Up and Go test < 20 s), followed by lower multimorbidity, better cognition, and not living alone. In bivariate regression, living at home was also associated with age, fall risk, vulnerability, depression, and previous independence in activities of daily living.
Conclusion: Mobility is the most important predictive factor for living at home after geriatric rehabilitation. Assessment and training of mobility are therefore key aspects in geriatric rehabilitation.
Key words: rehabilitation; aged; treatment outcome; prognosis.
Accepted Oct 14, 2016; Epub ahead of print Jan 18, 2017
J Rehabil Med 2017; 49: 185–190
Correspondence address: Jan Kool, Rehabilitation Center Kliniken Valens, Taminaplatz 1, CH-7317 Valens, Switzerland. E-mail: jan.kool@kliniken-valens.ch
During the past decades the proportion of older people in Switzerland has increased. In 2015 29% of all citizens were over 65 years old and 5% were over 80 years old (1). Older age is associated with increased need for assistance with activities of daily living (ADL), reduced mobility, and a higher probability of referral to a long-term care facility (2). The Swiss Federal Office of Statistics (3) found that 6% of all citizens over 65 years of age live in a long-term care facility (ranging from 1% of persons aged 65–74 years to 48% of those over 84 years of age). Referral to a long-term care facility often occurs following hospitalization and associated decline in independence in primary ADL, such as mobility and self-care (4). Many community-dwelling patients are therefore unable to live at home after hospital discharge. Geriatric rehabilitation has the primary goal of enabling patients to return home.
It involves a multidisciplinary approach using a comprehensive set of assessment and treatment procedures to restore mobility, self-care abilities and cognitive function (5). Several randomized controlled trials have demonstrated the effectiveness of geriatric rehabilitation. It has been shown that rehabilitation does not increase the total cost of medical care (6, 7). A meta-analysis (6) concluded that geriatric rehabilitation improves functional independence and reduces mortality and placement in long-term care facilities, thereby increasing the proportion of patients living at home.
Improved insight into patient characteristics predicting living at home may support health professionals in goal setting and treatment planning for patients and their caregivers, which may improve allocation of resources. A recent review of predictors for living at home after geriatric rehabilitation concluded that lower age, independent mobility, being married, better cognitive status, and lower levels of depression were significantly associated with discharge home (8). There was insufficient evidence for the influence of living alone, comorbidity and length of stay on discharge home. Vulnerability, defined as the risk of deterioration in health and mobility, was predictive for death and functional decline (9). From the clinical point of view, it is relevant to note that some predictive factors are modifiable, while others are not. Age and being married are not modifiable by rehabilitation, whereas treatment can, for example, improve mobility and independence in ADL (10, 11).
The majority of studies included in a meta-analysis evaluating predictors for living at home after geriatric rehabilitation (8) were performed in Scandinavia and the USA. The influence on living at home was conflicting for ethnicity, living alone, and sex (8). A possible reason for these conflicting results is that patient populations, healthcare and social security systems differ between countries. These differences might change the predictive value of factors for living at home after rehabilitation. Switzerland has no insurance covering the full costs of long-term care facilities, and many patients cannot cover the costs of a long-term care facility themselves. Furthermore, the high level of familial support in Switzerland promotes familial care if health conditions allow living at home. Consequently, predictive factors for living at home may differ between Switzerland and other countries.
The objective of this study in a geriatric rehabilitation setting in Switzerland was therefore to evaluate predictive factors for living at home 3 months after discharge.
This prospective cohort study was conducted in Kliniken Valens-Walenstadtberg, a clinic for geriatric inpatient rehabilitation in the German-speaking region of Switzerland. Between February and November 2014 patients aged ≥ 65 years were recruited consecutively. The study was conducted in accordance with the principles of the Declaration of Helsinki 1975, revised 1983, and approved by the ethics committee of Kanton St Gallen, Switzerland (registration number EKSG 10/072/1B).
Participation in the study did not affect any aspect of geriatric rehabilitation. A standardized geriatric assessment was performed, together with individual goal-setting to plan rehabilitation interventions (12). Improving mobility was a high-priority goal, as most patients required assistance with walking. Patients received a mean of 3 treatment sessions per day, for a total of 2 h daily, 6 days per week. Treatment included individual physical and occupational therapy, medical exercise training in groups, and aquatic exercise. The indication for any treatment, including medication, was the responsibility of the rehabilitation team and was based on the patients’ needs.
All patients aged 65 years or more who were referred for geriatric inpatient rehabilitation were eligible to enter the study. Inclusion criteria were: sufficient understanding of German to answer the questionnaires and to provide written informed consent. Exclusion criteria were: medical conditions that interfered with completing the study questionnaires, e.g. severe psychiatric disorders, dementia, and severe hearing and visual impairments.
The dependent variable was living at home at 3-month follow-up. Independent variables or predictor candidates covered the Activity and Participation domain and contextual factors of the International Classification of Functioning, Disability and Health (ICF) Core Set for post-acute rehabilitation (13, 14). Predictor candidates in the Activity and Participation domain were: mobility, fall risk, ADL independence before hospitalization (yes/no), and vulnerability. Mobility was assessed with the Timed Up and Go test (TUG). Ninety-five percent of persons up to 65 years of age complete the TUG in 10 s or less (15). To allow analysis of all patients including those who were unable to stand up or walk, the results were re-coded into an ordinal scale. A time of up to 10 s was coded as 1, 11–20 s as 2, 21–30 s as 3, 31 s or more as 4, and unable to perform as 5. Fall risk (yes/no based on current walking ability, previous falls, use of walking aids) was evaluated in the nursing assessment, the ePA-AC (ergebnisorientiertes Pflege Assessment-acute care; outcome-oriented nursing assessment for acute care (16)). Vulnerability, defined as the risk for deterioration in health and mobility, was evaluated with the Vulnerable Elders Survey (VES-13) (9). The VES-13 is a patient administered 13-item questionnaire covering age (0–3), self-rated health (0–1), physical function (0–2), and functional disability (0–4). The total score is between 0 and 10, with 10 representing maximal vulnerability. Predictor candidates in the ICF domain of contextual factors were: age, sex, multimorbidity, cognition, depression, living alone, and mobility barriers (stairs outside or inside the patient’s home). Multimorbidity was assessed with the physician-administered Cumulative Illness Rating Scale (CIRS (17)). The CIRS rates the medical burden of 14 organ domains on a 0–4 severity scale, with a total score of 56 representing maximum medical burden. Cognition was evaluated with the Mini-Mental State Examination (MMSE 0–30, where best cognition is 30 (18)), and depression with the Geriatric Depression Scale (0–5, with a score of 0–1 indicating no suspicion of depression) (19)). Stairs outside or inside the patient’s home (yes/no) were considered as a potential barrier and candidate predictor for living at home.
All candidate outcome predictors were recorded at the beginning of rehabilitation, except for mobility. Mobility was assessed at the end of rehabilitation, since initial mobility was considered less relevant for living at home 3 months after rehabilitation. At the 3-month follow-up it was recorded whether patients were living at home. Patients were sent a postal questionnaire and, in case of non-response, contacted by telephone. All data collection was performed by a research assistant.
The sample size for logistic regression was determined a priori. Assuming 20 observations per predictor variable would be needed (20), a model with a maximum of 6 predictor variables would require a minimum of 120 patients.
Whether data were missing completely at random (MCAR), i.e. the probability of data being missing does not depend on the observed or unobserved data, was analysed by comparing descriptive statistics in patients with complete and incomplete data (21). If data were not MCAR, it was assumed that data were missing at random (MAR). MAR implies that the probability of data being missing does not depend on the unobserved data (21).
Missing data reduce the power of the analysis and may lead to biased results (22). Multiple imputation (MI) of missing data improves both the power and the validity of subsequent analyses. MI was performed using the multiple imputation chained equations algorithm (21). Five MI data-sets were created based on the available data from all dependent and independent variables that were used in the subsequent primary analyses.
Logistic regression (23) was performed, with living at home at 3-month follow-up as the dependent variable and candidate predictors as the independent variables. Collinearity of candidate predictors, defined as an association > 0.7, was evaluated. In case of collinearity between two predictors, one of them was excluded from further analysis. Bivariate logistic regression was performed with candidate predictors in each MI data-set. Values of continuous and ordinal predictors were dichotomized using the receiver operating characteristic (ROC) curve, Joudas Index and computed odds ratios (ORs).
Multivariate regression was then performed in each MI data-set, using candidate predictors with a p-value < 0.05 in bivariate logistic regression and the likelihood-based backward procedure. A final model was fitted to the data using all candidate predictors that predicted living at home at 3-month follow-up in at least 2 out of 5 MI data-sets. The results from this final analysis were pooled. A secondary analysis was performed in complete cases (CC) and the results of the 2 analyses were compared. SPSS for Windows, version 23 (SPSS Inc., Chicago, IL, USA) was used for these statistical analyses.
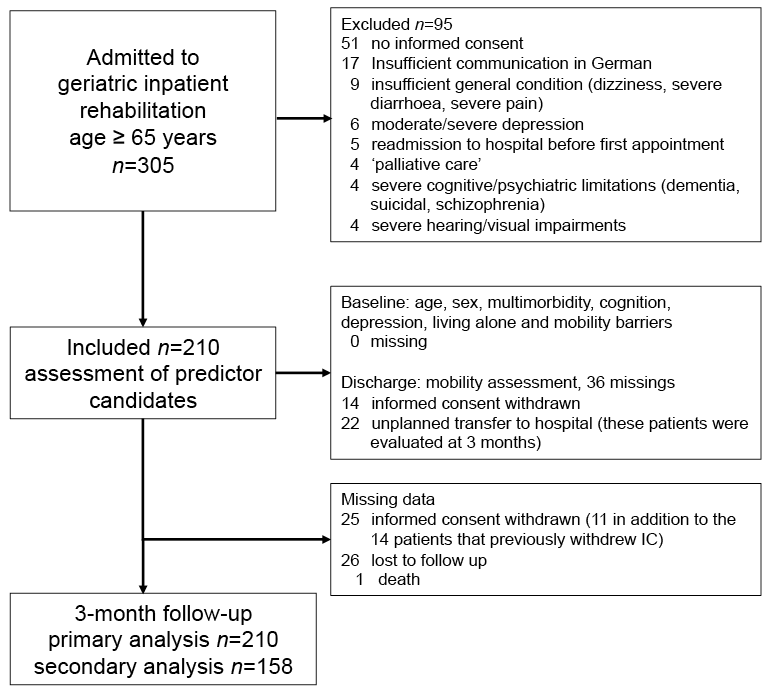
Fig. 1. Patient recruitment, characteristics and data collection.
Between February and November 2014 69% (210/305) of the patients aged 65 years or older who were admitted for inpatient rehabilitation were included in the study (Fig. 1). The main reasons for exclusion were: not consenting to participation (54%) and insufficient understanding of German (18%) preventing the completion of questionnaires.
Table I shows the baseline characteristics of the study population. Patients were elderly community dwellers. Most patients (77%) needed to climb stairs to enter their home. The majority of patients (87%) were admitted to rehabilitation after acute hospital care and 13% directly from home because of a decline in independence in primary ADL, such as mobility and self-care. Median length of stay at the rehabilitation centre was 20 days (interquartile range (IQR) 13–26 days).
Table I. Characteristics of the study population
Data were complete at baseline, when most predictors were recorded, and available for 88% (184/210) of subjects after rehabilitation, when mobility was recorded, and for 75% (158/210) of subjects at 3-month follow-up (Fig. 1). Withdrawal of informed consent and non-response were the main reasons for missing data after rehabilitation and at 3-month follow-up.
Patients with available follow-up data were younger (75.4 vs 77.7 years) and healthier (CIRS score 11.9 vs 12.3) at baseline, compared with patients with missing follow-up data. They had better scores for mobility (TUG 24 vs 29 s), cognition (MMSE 24.9 vs 22.6) and depression (GDS 0.7 vs 0.9). Because data were not MCAR, results from complete case analysis may be biased and primary analysis in MI data-sets is preferred.
After 3 months, 86.8% of patients lived at home (pooled results of 5 MI data-sets). All correlations between independent variables or candidate predictors were <0.7. Therefore, all candidate predictors were used for further analysis. Living at home at 3-month follow-up was predicted by age, multimorbidity, depression, living alone, cognition, mobility, fall risk, ADL independence before hospitalization, and vulnerability in 2 or more MI data-sets. Table II shows ORs (pooled results from MI data-sets) that were significant for mobility (TUG<20 s.), multimorbidity, vulnerability and ADL independence before hospitalization. Sex and mobility barriers (stairs outside or inside the patient’s house) were not included in any of the bivariate regression models in each of the 5 MI data-sets with living at home at 3-month follow-up as the dependent variable.
Table II. Odds ratios (OR) of predictor candidates for living at home 3 months after rehabilitation, in order of increasing upper bound of the OR’s 95% confidence interval (95% CI)
According to the final model (Table III), the log odds of a patient living at home at 3-month follow-up was associated with better mobility, lower multimorbidity, higher levels of cognition, and not living alone. The final model did not include age, depression, fall risk, ADL independence before hospitalization and vulnerability. The strongest single predictor for living at home was mobility.
Table III. Logistic regression analysis of 210 patients living at home at 3-month follow-up (pooled results from 5 multiple imputation data-sets). The tests used were: Mobility: Timed Up and Go Test, 5-point ordinal scale from 1= normal to 5= unable to perform; multimorbidity: Cumulative Illness Rating Scale 0–56 (maximal multimorbidity), cognition: Mini-Mental State Examination 0–30 (maximal cognition), living alone 1= yes, 0= no. Nagelkerke R2= 0.32
In the secondary analysis in complete cases (158/210, 75%), 9.5% of patients were not living at home at 3-month follow-up. This rate was 39% lower than in the MI data-sets (13.2%). The same procedure was used to fit a model to the data in complete cases. The final model included multimorbidity (CIRS) and cognition (MMSE), but not living alone and mobility (TUG). ADL independence before rehabilitation was also included.
This study evaluated candidate predictors for living at home after geriatric rehabilitation in patients referred for rehabilitation directly after acute inpatient hospital treatment. The strongest predictor for living at home was mobility at discharge, measured with the TUG. Other predictors for living at home were: lower multi-morbidity, better cognition, and not living alone. In bivariate regression, living at home was also associated with age, fall risk, vulnerability, depression, and ADL independence before hospitalization, but these factors were not included in the final multivariate prediction model because inclusion did not further improve prediction of living at home.
Our results are consistent with those of a systematic review in which mobility, cognition, absence of depression, age, and ADL-independence, assessed with the Functional Independence Measure (FIM), predicted living at home (8). The FIM is a composite score covering motor ADL, such as walking and cognitive functions. The review did not assess the predictive validity of the TUG for living at home after geriatric rehabilitation. The TUG is a short and simple test that can be used anywhere and is the only predictor identified in this study that was not included in the review. Mobility evaluated with the TUG may be particularly important in Switzerland, as most of the patients return home and are cared for by relatives or health professionals. In this setting it is often mandatory that patients are mobile with a low risk of falls, as they are not always supervised.
As expected, age predicted living at home if used as single predictor. However, in the present study age was not included in the final prediction model based on multivariate regression. This result confirms that age should not be used to select patients for referral to rehabilitation. In our study, living alone before hospitalization increased the risk of placement in a long-term care facility, while its influence was uncertain in previous studies summarized in that review (8). In other research, functional and cognitive status measured with the FIM predicted living at home (8). Our study measured mobility with the TUG and cognition with the MMSE. Other research identified functional status at the beginning of geriatric inpatient rehabilitation as a predictor for discharge home (24).
Vulnerability, assessed with the VES, was associated with living at home in our study as well as in other studies in geriatric populations (25, 26). Vulnerability was not included as a predictor in the final multivariate model. A possible reason is that, in our study, the 3 VES domains, age, limitation in physical function, and functional disability, were also used as single predictor candidates that were more predictive than the VES.
Some predictors of rehabilitation outcome, such as age and being married, are not modifiable by rehabilitation. Such predictors are of limited value as they improve our knowledge about the probability of living at home, but do not provide any opportunity for treatment to improve outcome. The fact that mobility is the strongest predictor for living at home is very positive because geriatric rehabilitation improves mobility (6).
This study has several strengths. It is the first study in Switzerland to evaluate geriatric rehabilitation outcome in a large sample of patients (n = 210). Patients were recruited consecutively, and the majority of all patients referred for rehabilitation (70%) were included. Therefore, the results can be considered as representative for patients referred for geriatric rehabilitation after acute hospital care in Switzerland. Candidate predictors for living at home 3 months after rehabilitation covered not only health-related, but also physical and social/environmental factors.
The level of loss to follow-up in this study can be considered as acceptable, taking into account the longitudinal design and the difficulty of collecting follow-up data in geriatric patients. Patients with missing follow-up data were older and less healthy, leading to an increased risk of bias in the results of a complete case analysis. To reduce bias and improve the validity of results, the primary analysis was performed in MI data-sets. Mobility and living alone were included in the prediction model based on all cases (n = 210), but not in the model in cases with complete data (n = 158). This difference indicates that missing data may have led to bias. The proportion of patients living in a long-term care facility at 3-month follow-up was 9.5% in complete cases and 13.2% in cases with missing data. The predictive models for living at home at 3-month follow-up were, in part, different in MI data-sets and complete cases. This difference demonstrates the importance of the MI analysis, which is considered more valid than complete case analysis.
Excluding patients from the study participation may have reduced the generalizability of the results. The exclusion rate of 31% in the present study was quite low. However, exclusion mainly affected patients with severely impaired cognition, thus reducing the variance of cognition among patients. It is assumed that cognition would be a stronger predictor if all patients had been available for the analysis.
Mobility was the most important predictor of living at home. Geriatric rehabilitation can improve mobility. Increasing treatment dose by prolonged duration of exercise may improve outcome, but is expensive. Further research to improve the cost-effectiveness of geriatric inpatient rehabilitation is therefore needed. Geriatric rehabilitation does not seem to increase the total cost of medical care (6, 7, 27). Nevertheless, to improve the cost-effectiveness of rehabilitation, research should focus on patient selection for inpatient and outpatient geriatric rehabilitation, and on improvement of rehabilitation protocols. Increased use of healthcare technology might improve cost-effectiveness. A study is currently evaluating whether exergames promoting mobility are an attractive alternative to conventional self-regulated exercises for elderly people (28). More research is needed into exergames in geriatric rehabilitation in order to improve ease of use and efficacy. To improve geriatric rehabilitation further research is needed in patients with marked cognitive dysfunction, including dementia. Patients with marked cognitive dysfunction were excluded from our study. The current evidence-base for choosing treatment options for these patients is extremely weak, and communication difficulties and a lack of outcome assessments validated for research in this population hinder research in this area.
Mobility is the most important predictive factor for living at home following geriatric rehabilitation that has been shown to improve mobility (6). As limited mobility is a major risk factor for falls, and falls are associated with high mortality and morbidity, our results indicate that it is mandatory to improve mobility. Treatment planning and goal setting should focus primarily on mobility and should include walking, strength and balance training.
Despite the proven effectiveness of geriatric rehabilitation for improving mobility, Swiss health insurance is restrictive in covering the costs in patients with mobility restrictions. Increasing financial resources for geriatric rehabilitation through health insurance would improve mobility, thereby decreasing referrals to long-term care facility, reducing costs and improving quality of life in the elderly population. Improving community-based geriatric rehabilitation for older persons in Switzerland may be cost saving.


 Click to show fullsize
Click to show fullsize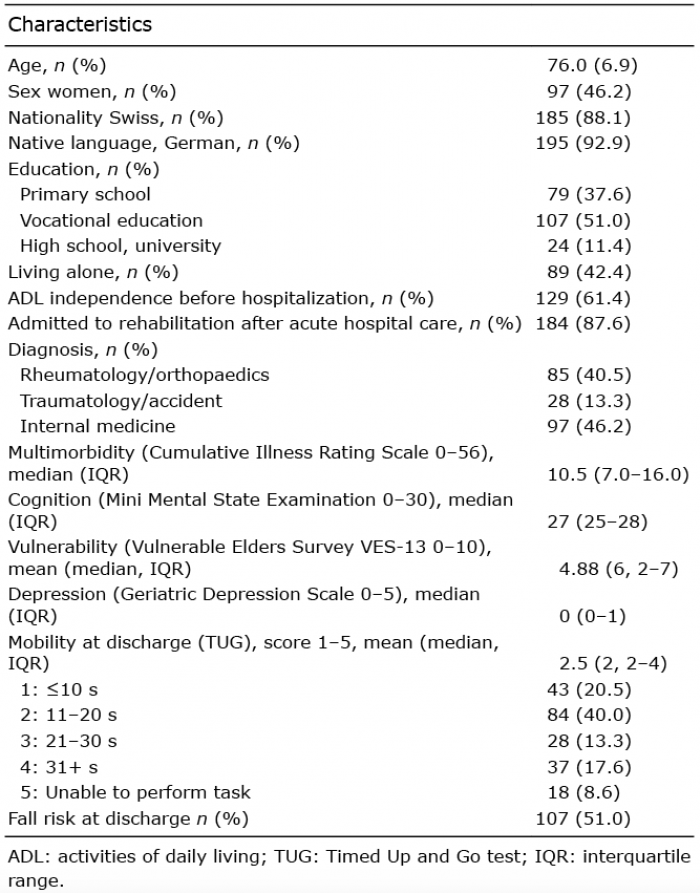 Click to show fullsize
Click to show fullsize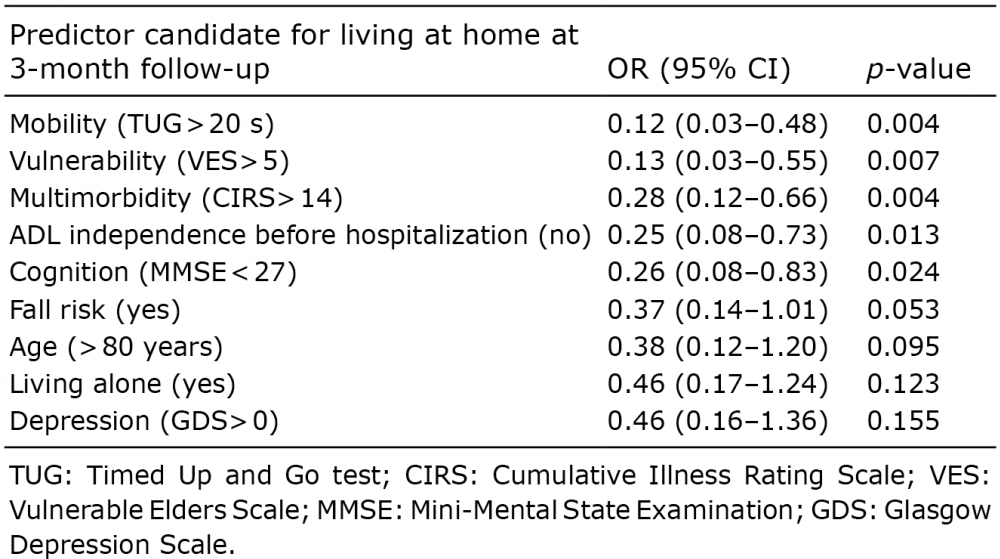 Click to show fullsize
Click to show fullsize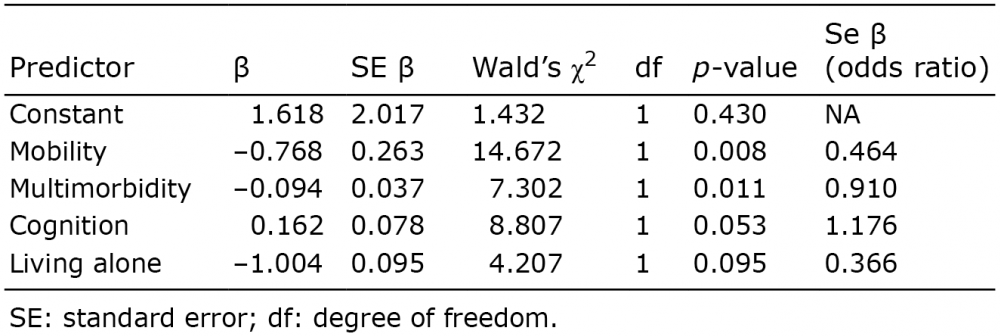 Click to show fullsize
Click to show fullsize