
From the 1Occupational Therapy, Department of Community and Clinical Allied Health, School of Allied Health, La Trobe University, Bundoora, 2Neurorehabilitation and Recovery, Stroke Division, The Florey Institute of Neuroscience and Mental Health, Heidelberg, 3Living with Disability Research Centre, School of Allied Health, La Trobe University, Bundoora, 4Summer Foundation, Box Hill, 5Department of Occupational Therapy, Faculty of Medicine, Nursing and Health Sciences, Monash University, Clayton, Australia, 6Institute of Neuroscience and Physiology, Gothenburg University and Sahlgrenska University Hospital, Gothenburg, Sweden, 7Statistics and Decision Analysis, Florey Institute of Neuroscience and Mental Health, Heidelberg, 8Mathematical Sciences, School of Science, RMIT University, Melbourne, 9Department of Medicine, Monash University, Stroke Unit, Monash Health, Clayton, 10The Florey Institute of Neuroscience and Mental Health, Parkville, and 11Department of Medicine, Melbourne Brain Centre, Royal Melbourne Hospital, University of Melbourne, Parkville, Australia, and the START Research Team (www.START.csiro.au)
Objective: To quantify the association of depressive symptoms with retained activity participation 3 months post-stroke, after adjusting for neurological stroke severity and age.
Design: A cross-sectional observational study of retained activity participation and depressive symptoms in stroke survivors with ischaemic stroke.
Participants: One hundred stroke survivors with mild neurological stroke severity.
Methods: One hundred stroke survivors were recruited from 5 metropolitan hospitals and reviewed at 3 months post-stroke using measures of activity participation, Activity Card Sort-Australia, and depressive symptoms, Montgomery-Asberg Depression Rating Scale Structured Interview Guide (MADRS-SIGMA).
Results: The median percentage of retained overall activity participation was 97%, (interquartile range 79–100%). Using multiple median regression, 1 point increase in the MADRS-SIGMA was associated with a median decrease of 0.7% (95% CI –1.4 to –0.1, p=0.02) of retained overall activity participation, assuming similar neurological stroke severity and age.
Conclusion: The findings of this study establish the association of depressive symptoms with retained activity participation 3 months post-stroke in stroke survivors with mild neurological stroke severity. Clinical rehabilitation recommendations to enhance activity participation need to account for those with even mild depressive symptoms post-stroke.
Key words: stroke; social participation; human activities; depression, recovery of function; rehabilitation.
Accepted Oct 25, 2016; Epub ahead of print Jan 24, 2017
J Rehabil Med 2017; 49: 120–127
Correspondence address: Tamara Tse, Occupational Therapy, Department of Community and Clinical Allied Health, School of Allied Health, La Trobe University, Bundoora, VIC, 3086, Australia. E-mail: t.tse@latrobe.edu.au
Two-thirds of stroke survivors will sustain a disability that affects their ability to carry out everyday life activities (1). The International Classification of Functioning, Disability and Health (ICF) defines participation as “a person’s involvement in a life situation”(2); that is, doing everyday life activities, such as leisure, social and work activities. Since the endorsement of the ICF in 2001 (2), participation is considered a critical outcome of successful rehabilitation (3).
Depression is a common sequelae of stroke, with estimates of 30–60% of all stroke patients (4), and pooled estimated prevalence of 31% (5). However, the relationship between depression and participation after stroke is relatively unknown. Of the few studies investigating the relationship between depressive symptoms and participation there appears to be a relationship in particular with: social participation (Assessment of Life Habits: LIFE-H) 6 months post-stroke (6); participation restrictions (London Handicap Scale) 1 year post-stroke (7) and beyond (8); and participation restriction and satisfaction (Utrecht Scale for Evaluation of Rehabilitation-Participation) 6 months post-stroke (9). These studies have been conducted in Canada (6), Hong Kong (7), Italy (8) and the Netherlands (9) with sample sizes of 73–325 subjects. Given that the prevalence of depression is high early post-stroke and then declines in the months to years following stroke (10), it is also important to investigate the impact of depression on participation prior to 6 months post-stroke.
Participation is a broad concept and difficulties operationalizing it have been reported (11). Furthermore, participation is affected by contextual factors, particularly cultural contexts (2). In a review of participation measures used in clinical stroke studies, the Activity Card Sort (ACS) was identified as the tool that covered the most domains of the ICF Activities and Participation domains and met the most psychometric properties (12). The ACS was originally developed in the USA (13) and has been adapted to an Australian population (14). The ACS provides a unique measure of retained activity participation that reflects a change in, and not pre-existing restrictions in, activity participation.
The current research was undertaken to establish the percentage of retained activity participation 3 months after stroke and to explore the magnitude and significance of associations between depressive symptoms and retained participation in the early months after stroke. To the best of our knowledge, the relationship between percentage of retained activity participation and depressive symptoms has not been investigated previously. Since participation has been shown to be influenced by age and neurological stroke severity (8, 15), these factors were accounted for in the analysis. The primary hypothesis for this study was that: survivors of stroke with more depressive symptoms will report participation in fewer overall activities, relative to pre-stroke, after adjusting for neurological stroke severity and age. In addition, we explored whether depressive symptoms were associated with all or specific sub-categories of activity participation.
This study formed part of START-PrePARE (Stroke imAging pRevention and Treatment–Prediction and Prevention to Achieve optimal Recovery Endpoints after stroke), a large multi-centre cohort study investigating post-stroke recovery (16). The study is registered and approved by the Australian New Zealand Clinical Trials Registry (NTA0902, trial ID: ACTRN12610000987066). Participants are recruited into START-PrePARE either via the route as a sub-study of START-EXTEND (within 4.5–9 h post-stroke) (17) or via the START-PrePARE stand-alone study (within 3 days post-stroke) (16).
A cross-sectional observational study of retained activity participation, using the Activity Card Sort-Australia and depressive symptoms, using the Montgomery-Asberg Depression Rating Scale Structured Interview Guide (MADRS-SIGMA) was carried out 3 months post-stroke. All participants were tested on the same standardized outcome measures at the hospital, research institute, or in their own homes. Background demographic, neurological stroke severity, history of depression prior to stroke, and cognitive function data were gathered from the database of START-PrePARE. The interview to identify presence of depressive symptoms preceded the assessment of activity participation. To minimize observational bias, researchers were trained in all outcome measures and structured interview guides were used.
Ethics approval was obtained from the hospitals and tertiary institute involved in this study and followed ethical standards of the responsible ethics committee in accordance with the National Statement on Ethical Conduct in Human Research 2007. All participants gave written informed consent prior to the start of data collection.
To be included, participants had to have a diagnosis of ischaemic stroke, be 18 years or older, speak English, and not have a significant disability prior to stroke, as determined by a score of less than 2 on the Modified Rankin Scale (18). The hospitals recruiting for the study had to have over 350 beds and treat over 800 strokes per year. Participants were recruited from 5 acute hospitals with stroke units in the city of Melbourne, Australia. Melbourne has a population of approximately 4 million and the hospitals were within 21 km of the city centre.
The primary outcome was percentage of retained activity participation, as measured using the Activity Card Sort – Australia recovering version (ACS-Aus) (14). The ACS-Aus is a reliable and valid measure of activity participation (19). The ACS-Aus consists of 82 cards with photographs of older people doing different activities. Participants sort the cards into 5 groups to reflect their current activity participation (“not done prior to the illness/injury”= Not Applicable; “continued to do during the illness/injury”= 1; “given-up due to the illness/injury”= 0; “beginning to do again”= 0.5; and “new activity since the illness/injury”= 1). Scores are calculated to determine previous activity participation level, current activity participation level, and percentage of retained activity participation. A list of the activities and their sub-categorization is provided in Appendix I. The primary score used in this study was percentage of retained overall activity participation, with additional scores for sub-categories of leisure, social/educational and household activities.
The independent variable was depressive symptoms 3 months post-stroke. Depressive symptoms were assessed using the Montgomery-Asberg Depression Rating Scale Structured Interview Guide (MADRS-SIGMA) (20). MADRS-SIGMA scores of greater than or equal to 7 indicates presence of depressive symptoms (21) and scores higher than 17 are indicative of major depression (20).
The variables adjusted for in our analysis were neurological stroke severity and age. Neurological stroke severity was measured 3 days post-stroke using the National Institute of Health Stroke Scale (NIHSS) (22), i.e. the earliest common time when NIHSS was assessed. A total score of less than 5 indicates mild neurological stroke severity (23).
In addition, the presence of history of depression prior to stroke and the presence of cognitive impairment at 3 months post-stroke were monitored, as these factors may also be associated with depressive symptoms (24). The history of depression prior to stroke questionnaire was adapted from the World Mental Health Survey Initiative Version of the WHO Composite International Diagnostic Interview (CIDI) (25). The first 3 questions ask participants to report if they have ever experienced a period of sadness; discouragement; or disinterest lasting for several days or longer. If participants responded yes, further questions were asked to identify the duration of the episode. Presence of history of depression was indicated if participants reported experiencing disinterest and either sadness or discouragement and for a period of at least 2 weeks. Presence of cognitive impairment was screened for using the Montreal Cognitive Assessment (MoCA) (26). Scores less than 23 are suggestive of cognitive impairment (27). Strategies for testing people with aphasia were developed for this study based on aphasia-friendly principals by Brennan et al. (28). Finally, return to work was also monitored for its association with depressive symptoms, given it is a common activity engaged in by adults. Participants were surveyed for their return to work status separately, as work is not included in the ACS-Aus.
Multivariable median regression analysis (29) was used to examine the relationship between percentage of retained overall activity participation and depressive symptoms, adjusting for neurological stroke severity and age. Median regression analysis estimates the median of the dependent variable, conditional on the values of the independent variable. It is more informative than parametric methods when the distribution scores are highly skewed, such as the distribution of the ACS-Aus scores in this sample. Pseudo R-squared for median regression (30) was used to measure how close the data were to the fitted median regression line. An a priori sample size and power calculation (16) proposed that a sample size of 100 would be sufficient to detect a small effect size based on a regression model including depressive symptoms, stroke severity, and age as independent variables, with a power of 0.8 (31).
As a hypothesis-generating investigation, the association of depressive symptoms was also examined in relation to the ACS-Aus sub-categories, adjusting for neurological stroke severity and age, using multivariable median regression analysis. No multiplicity corrections were applied for tests with sub-categories due to the exploratory nature of the analysis.
Factors that may influence depressive symptoms, such as history of depression prior to stroke, presence of cognitive impairment and return to work, were explored. The Mann–Whitney U test was used to test the differences in MADRS-SIGMA scores between: (i) those with history of depression prior to stroke and those without; (ii) those with cognitive impairment and those without; and (iii), those who had returned to work and those who had not returned at 3 months post-stroke in the subset who were working just prior to their stroke. Similarly, these factors may also influence stroke severity, and thus difference in NIHSS scores related to these factors were also tested for using the Mann–Whitney U test.
Finally, to further understand the relationship between depressive symptoms and activity participation and to test the robustness of the model, a post-hoc analysis was conducted to investigate the association between depressive symptoms and current activity participation level, adjusting for previous activity participation level, neurological stroke severity and age using ordinary least squares regression.
Descriptive statistics and Mann–Whitney U tests were conducted using SPSS, version 21.0 (IBM Corp.). Median regression analysis with bootstrapped standard error estimations and R-squared analysis was conducted using STATA 12.0 (StataCorp LP).
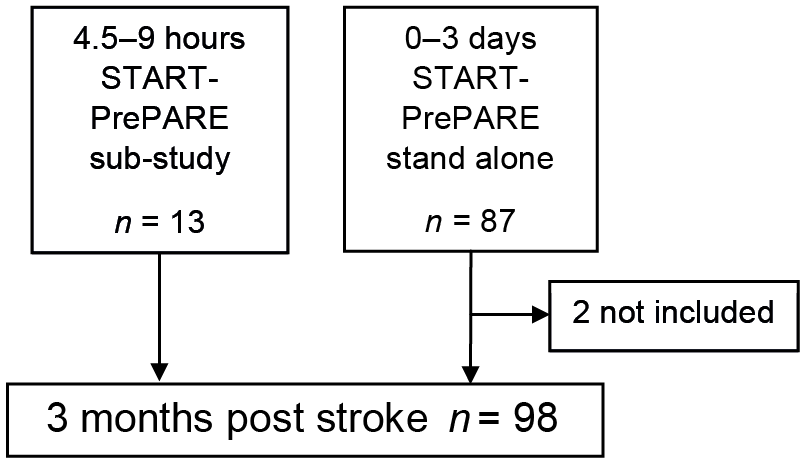
One hundred stroke survivors were recruited into the START-PrePARE sub-study (n = 13) or the stand-alone study (n = 87) between June 2010 and April 2013. Participants were assessed at 3 months post-stroke follow-up appointment. Four assessors collected the data. The first author collected data on 86 of the 100 participants, and 3 research assistants collected the data on the 13 other participants. Of the 100 participants, 70 were assessed at the research institute, 29 at home and 1 at a hospital. One male participant was not able to attend his 3-month appointment and hence did not complete the ACS-Aus and the MADRS-SIGMA. Inspection of the MADRS-SIGMA and the ACS-Aus scores revealed that 1 male participant had a MADRS-SIGMA score of 33 and retained activity participation of 163%. This participant was deemed an outlier and was removed from the analysis.
The flow of participants through the study is illustrated in the Fig. 1. The resultant group analyzed (n = 98) comprised 28 women (29%) and 70 men (71%) with a mean age of 66 years (SD 13; range 27–90 years). The majority of participants lived at home (96%). One participant was in hospital at 3 months post-stroke.
Fig. 1. Flow of participants through the study.
The majority of participants lived at home (96%). One participant was in hospital at 3 months post-stroke. Seventy participants were married and close to half were retired (47%). Mean time since stroke at time of assessment was 99 days (SD 16 days). The median score on the MoCA was 27 (IQR 25–29), suggesting that the study group, on average, was not cognitively impaired (< 23 on the MoCA). The number of participants with presence of depressive symptoms (≥ 7 on the MADRS-SIGMA) was 42 (42%), a similar proportion to previous studies using the MADRS post-stroke (21). Eighty-seven of the participants had NIHSS < 5 and the median NIHSS score was 1.0 (IQR 0.0–3.0), consistent with mild neurological stroke severity. Participant characteristics are shown in Table I.
Table I. Participants’ characteristics and activity participation outcomes 3 months post-stroke
The median percentage of retained overall activity participation 3 months post-stroke was 97% (IQR 79–100%). The sub-category of household activities had the highest percentage of retained activity participation compared with leisure activities and social/educational activities (see Table I for details). Current and previous activity participation levels at 3 months post-stroke are shown in Table II.
Table II. Current and previous activity participation level at 3 months post-stroke
Assuming similar age and neurological stroke severity, an increase of 1 point on the MADRS-SIGMA was associated with a median decrease of 0.7% (95% CI –1.4 to –0.1, p = 0.02) of retained overall activity participation. The squared correlation between the fitted values and the dependent variable (pseudo R-squared) was 0.28. No excessive collinearity was observed (mean variance inflation factor was below 2.5 and the condition number below 10) (32). Table III presents the summary of the regression model. Depression score was also associated with overall current activity participation after accounting for previous activity participation, neurological stroke severity and age, using linear regression as described in the methods and as shown in Table IV.
Table III. Regression coefficients of depressive symptoms on percentage of retained activity participation for overall activities, leisure activities, social/educational activities, and household activities, after adjusting for stroke severity and age
Table IV. Ordinary least squares (95% CI) regression coefficients of depressive symptoms on current activity participation level for overall activities, leisure activities, social/educational activities, and household activities, after adjusting for previous activity participation level, neurological stroke severity and age
Assuming similar age and neurological stroke severity, an increase of 1 point on the MADRS-SIGMA was associated with a median decrease of 0.8% (95% CI –1.2 to –0.4, p < 0.01) of retained leisure activity participation (see Table II). We did not observe an independent association for retained social/educational activities or household activities.
Twenty participants had a history of depression prior to stroke. These participants were not significantly different from those without a history of depression in MADRS-SIGMA scores (U = 719, p = 0.32) or NIHSS scores (U = 786, p = 0.73).
Fourteen participants had cognitive impairment. These participants were not significantly different from those without cognitive impairment in MADRS-SIGMA scores (U = 474, p = 0.24), but had significantly higher NIHSS scores than those without cognitive impairment (U = 341, p < 0.01).
Of the 50 participants who were working prior to their stroke, 34 (68%) had returned to work. These participants were not significantly different from those who had not returned to work in terms of MADRS-SIGMA scores (U = 220, p = 0.28), but had significantly lower NIHSS scores than those who had not returned to work (U = 132, p < 0.01).
This is the first study to quantify the percentage of retained activity participation and the association of depressive symptoms with retained activity participation 3 months post-stroke in stroke survivors with mild neurological impairment. Depressive symptoms were associated with retained activity participation overall, after adjusting for stroke severity and age; factors that have previously been associated with participation. These findings indicate that an increase of one depressive symptom was associated with an approximately 1% decrease in retained activity participation, which is equivalent to participating less in one previous activity. This was the case even in stroke survivors with mild neurological severity. The current findings extend those of earlier studies (6, 15) by measuring activity participation in the early months after stroke, and identifying the influence of depressive symptoms on overall activity participation. Participating in previous life activities is associated with life satisfaction after stroke (33) and physical and mental health in older adults (34). Identifying the modifiable factors that may impact on activity participation in stroke survivors may help clinicians identify stroke survivors who are at risk of poor participation outcomes and make more targeted rehabilitation recommendations to enhance activity participation. Our findings suggest that those with depressive symptoms should be monitored for participation outcomes in the sub-acute phases of recovery after stroke, as these individuals retain fewer (Table III and IV) overall activities. However, a 2-pronged approach, in which clinical interventions are focussed on improving participation alongside interventions targeting mood (35) may be a better approach to enhancing participation and low mood.
Investigation of depressive symptoms and the ACS-Aus sub-categories revealed that MADRS-SIGMA scores were negatively associated with percentage of retained leisure activity participation. Evidence has shown that engaging in leisure activities is related to an experience of enjoyment (36) and may be why we found a negative association with depressive symptoms. We did not, however, find a significant association for social/educational activities or for household activities. An explanation for why percentage of retained social/educational activities did not demonstrate an observed relationship with depressive symptoms could be that family and friends played a role in initiating and maintaining social activities with those experiencing depressive symptoms.
In contrast to previous findings (24), we did not observe a relationship between history of depression prior to stroke and depressive symptoms at 3 months post-stroke. This may be due to the questionnaire we used to derive history of depression. This tool may have overestimated history of depression. We identified 20 participants (20%) with a history of depression prior to their stroke, which is higher than that reported in the general population (14%) (37). Other studies have used prescribed antidepressants at stroke as a measure of history of depression. When we looked at participants’ medication at baseline only 6 participants were on antidepressants at baseline. These participants did not have significant different MADRS scores at 3 months compared with those not on antidepressants at baseline. The direct influence of history of depression on activity participation was not investigated in our study due to a priori sample size and power calculations based on a regression model of 3 independent variables (16); however, this warrants future investigation.
A significant association between cognitive impairment and depressive symptoms was not observed. This appears to be at variance with previous studies that found an association with cognitive impairment (24). One reason for this could be that the proportion of participants with cognitive impairments was smaller (14%) than in previous studies (20%) (24).
We did not find a significant difference in depressive symptoms between those who had or had not returned to work. Although this finding was similar to a previous study (38), the analysis conducted was exploratory and the findings are not conclusive.
The percentage of retained activity participation score reflects a change in activity participation following an injury, such as stroke, and not a score reflecting the actual number of activities the participants performed prior to their stroke. It is possible that the relationship between depressive symptoms and activity participation may be different when the actual number of activities engaged in is considered. An alternative method of scoring the ACS-Aus is the current activity participation level, which is the sum of activities the participant is currently performing. To further our understanding of participation at 3 months post-stroke we conducted a post-hoc investigation of actual activities engaged in. The current activity participation level scores were normally distributed. We therefore tested the relationship between the overall current activity participation level scores and depressive symptoms, adjusting for previous activity participation level scores, neurological stroke severity and age using ordinary least squares regression. A similar relationship was found between depressive symptoms and number of activities; a 1 point increase in MADRS-SIGMA was associated with a mean decrease of 0.5 in current activity participation level score. This is equivalent to participating less in one activity; the same findings as when percentage of retained activity participation was used. These findings were cross-validated using multivariable median regression, and similar results were found.
With the advancement of interventions for acute stroke, the majority of those surviving stroke have mild neurological stroke severity (39). However, as we found, even in a group of stroke survivors with mild neurological stroke severity, depressive symptoms influenced retained activity participation, as well as the number of activities stroke survivors engaged in. To further understand this relationship between activity participation and depressive symptoms, it will be important to explore this topic from the stroke survivors’ perspective. An integrated research approach, such as using qualitative methods in conjunction with quantitative methods, will allow for a more in-depth investigation into and understanding of activity participation and its influencing factors after stroke.
The aim of this study was to quantify the association of depressive symptoms with retained activity participation 3 months post-stroke, adjusting for stroke severity and age. Other factors that may have been associated with retained activity participation, such as cognition (40), were not included in the analysis due to a priori sample size and power calculations based on a regression model of 3 independent variables (16). Cognitive function was monitored in this study and demonstrated a small variance. Future studies could investigate the relationship between cognitive function, depressive symptoms and activity participation after stroke.
Another limitation was the measure of participation in our sample. The ACS-Aus was developed for a population aged 60 years or older. Although our participants had a mean age of 66 years, the age range was 27–90 years. Nevertheless, the ACS is a comprehensive, reliable and valid measure of participation (12) and, to date, no other study has investigated participation in an Australian stroke cohort 3 months post-stroke using the ACS-Aus. Moreover, age was adjusted for in our analysis.
The study population was restricted to a group of stroke survivors with mild neurological stroke severity. Whilst this was not planned a priori, it does limit the generalizability of our findings to survivors with mild neurological stroke severity. Furthermore, the low number of females recruited to our study is another factor limiting generalizability. Nevertheless, even in this sample with mild severity, a significant independent relationship arose between depressive symptoms and activity participation. Therefore, even in stroke survivors with mild neurological stroke severity, activity participation and depressive symptoms must be considered in the early months after stroke.
The authors acknowledge and thank the participants, lead investigators and study co-ordinators from the START recruiting sites; in particular, those from the START-PrePARE recruiting sites: Austin Hospital (Helen Dewey), Epworth Hospital (Richard Gerraty), Monash Medical Centre (Henry Ma), Royal Melbourne Hospital (Bruce C.V. Campbell), and Western Hospital (Tissa Wijeratne). The authors also thank the Commonwealth Scientific and Industrial Research Organization (CSIRO) management and research teams involved in this research, in particular Lance Macaulay and the CSIRO data analytics team (Simon McBride, Karen Harrap, Chris Stanbridge). Finally, the authors acknowledge and thank the management and research team of the START programme of research (www.START.csiro.au).
Financial support for the research was received from the Commonwealth Scientific and Industrial Research Organization (CSIRO) of Australia, Flagship Collaboration Fund through the Preventative Health Flagship; and support for analysis, write up and researchers from the Victorian Government’s Operational Infrastructure Support Program; James S. McDonnell Foundation 21st Century Science Initiative in Cognitive Rehabilitation-Collaborative Award (#220020413); NHMRC Centre of Research Excellence in Stroke Rehabilitation and Brain Injury (APP1077898); an Australian Research Council Future Fellowship awarded to LMC [#FT0992299]; and a La Trobe University Post Graduate Scholarship and Florey student scholarship awarded to TT.


 Click to show fullsize
Click to show fullsize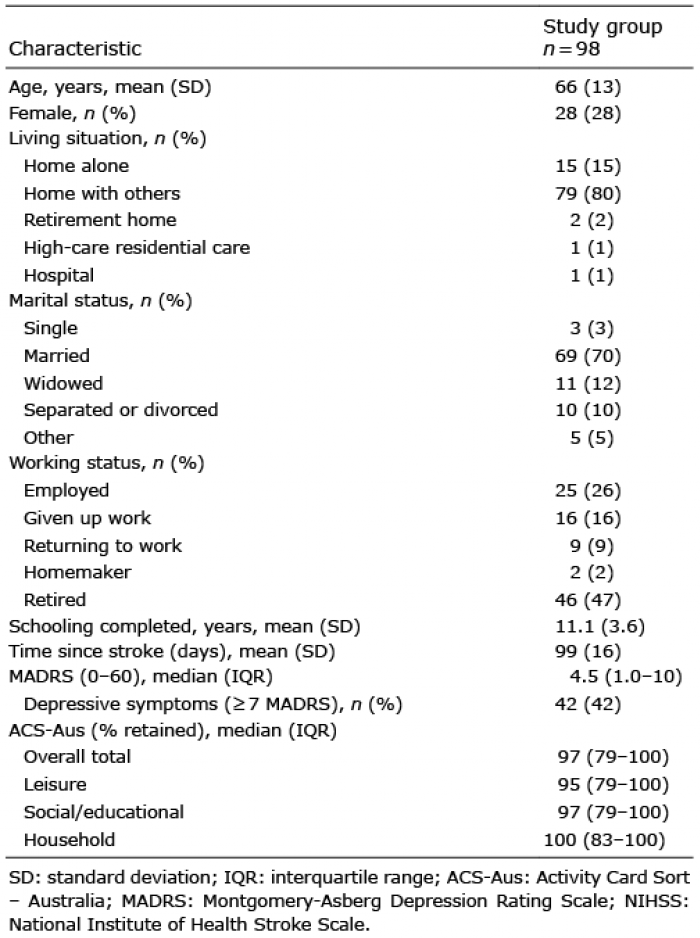 Click to show fullsize
Click to show fullsize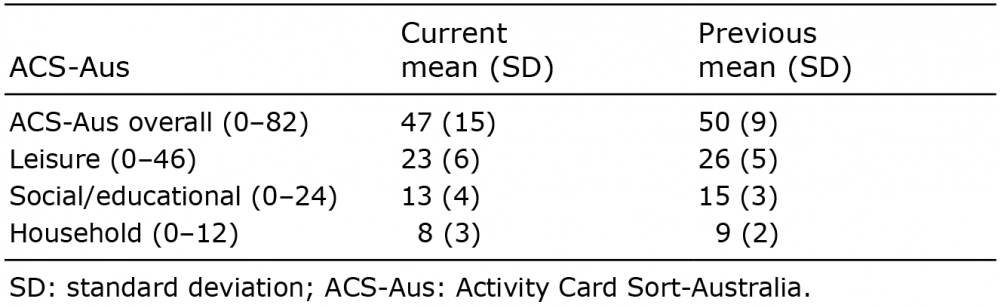 Click to show fullsize
Click to show fullsize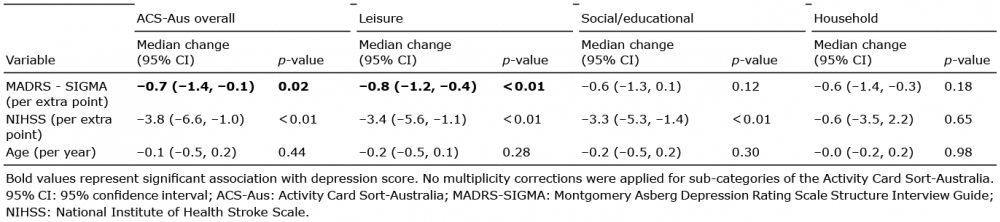 Click to show fullsize
Click to show fullsize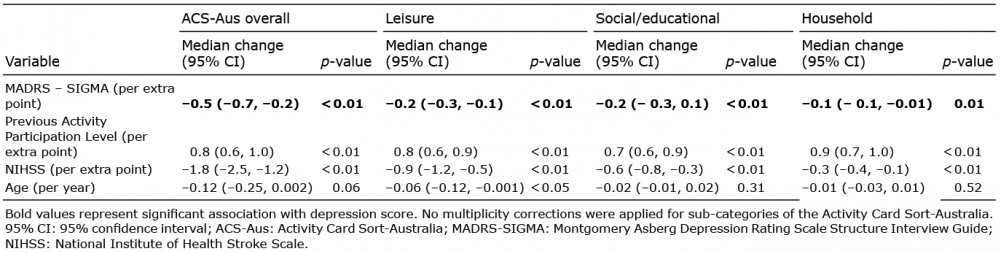 Click to show fullsize
Click to show fullsize