
From the 1Department of Rehabilitation Medicine, University of Malaya, 2University Malaya Medical Centre, Malaysia, 3Department of Health Sciences and Health Policy, University of Lucerne, Lucerne, 4Swiss Paraplegic Research (SPF), Nottwil, 5ICF Research Branch, a cooperation partner within the World Health Organization (WHO) Collaborating Centre for the Family of International Classifications in Germany (at DIMDI), Nottwil, Switzerland, 6Cheras Rehabilitation Hospital, 7National Head of Rehabilitation Medicine Services, Ministry of Health, Malaysia and 8SOCSO Rehabilitation Centre, Malacca, Malaysia
*Shared first authorship.
In February 2017, the World Health Organization (WHO) launched its historic ”Rehabilitation 2030: A Call for Action”. Scaling up rehabilitation in health systems requires concerted action across all 6 components of WHO’s Health Systems Framework. For rehabilitation, information about functioning is essential, as it is required for effective rehabilitation at all levels of the health system. What is missing is a countrywide demonstration project involving the implementation of a clinical quality management system for the continuous improvement of rehabilitation, both at the level of clinical care for individual patients and at the level of rehabilitation service provision. Consequently, the Department of Rehabilitation Medicine at the University of Malaya and University Malaya Medical Centre, together with the Cheras Rehabilitation Hospital of the Ministry of Health, and the Social Security Organisation (SOCSO) Rehabilitation Centre in Malacca, Malaysia, initiated a project to develop a Malaysian-wide clinical quality management system for rehabilitation (CQM-R Malaysia). The objective of this paper is to describe CQM-R Malaysia. First, a conceptual description of a CQM-R based on the International Classification of Functioning, Disability and Health (ICF) is set out. The methods, results and conclusions of a situation analysis conducted in January 2017 are then reported. Finally, the building blocks and implementation action plan developed for CQM-R Malaysia are presented.
Key words: clinical quality management; International Classification of Functioning, Disability and Health; rehabilitation; healthcare system.
Accepted Sep 6, 2017; Epub ahead of print Nov 16
J Rehabil Med 2018; 50: 00–00
Correspondence address: Gerold Stucki, Swiss Paraplegic Research (SPF), GZI Institute, SZ-6207 Nottwil, Switzerland. E-mail: gerold.stucki@paraplegie.ch
In February 2017 the World Health Organization (WHO) launched its historic ”Rehabilitation 2030: A Call for Action” (1). The call is based on the recognition of urgent need to scale up rehabilitation in health systems worldwide. The demand for rehabilitation services will increase in light of population ageing and the increasing number of persons living with injuries and non-communicable diseases (2). In many parts of the world this demand is not being met. WHO’s call for action is embedded in the United Nations’ (UN) strategy for Sustainable Development Goals 2030, in which health is seen as an issue that cuts across all 17 goals. As a basic health strategy, rehabilitation aims to optimize the functioning of individuals and the population and to minimize the experience of disability (3, 4).
Scaling up rehabilitation in health systems requires concerted actions across all 6 components of WHO’s Health Systems Framework relevant for health systems strengthening: governance, service delivery, financing, workforce, information, and health interventions (5). Although each component is important, health information, and a robust health information system, is vital for the success of all components (6). For rehabilitation, information about functioning is essential (7), both because the aim of rehabilitation is to optimize functioning, but also because functioning complements mortality and morbidity as the essential health indicators across WHO’s 5 health strategies (8).
Functioning information is required for effective rehabilitation at all levels of the health system: at the clinical level of professional–patient interaction; the level of service provision; and the level of policies and programmes (9). The standardized documentation of functioning at all 3 levels relies on the reference system provided by WHO’s International Classification of Functioning, Disability and Health (ICF) (10). The ICF provides the scientific basis for establishing the standards for ”what to document”; the ICF Generic Sets and ICF Core Sets for specific health conditions and situations, such as post-acute care and vocational rehabilitation, as well as the basis for qualitative linking and quantitative mapping of data that is collected using a wide range of data collection tools, including clinical tests and outcome instruments (11). Since scaling up of rehabilitation across the health system relies on functioning information at all levels, it is essential that functioning information is mainstreamed in national health information systems (7).
However, the successful implementation of a standardized documentation of functioning information at the clinical, services and national rehabilitation programming levels poses a unique challenge, since it depends on the possibility of forging a link between healthcare practice, science and governance (12). In the context of the current collaborative work-plan of the International Society of Physical and Rehabilitation Medicine (ISPRM) and WHO there are increasing efforts toward system-wide implementation of functioning information documentation at the regional and country levels, specifically in Europe (12, 13), China (14, 15), Japan (16) and Switzerland (17).
What is currently missing is a countrywide demonstration project involving the implementation of a clinical quality management system for the continuous improvement of rehabilitation, both at the level of clinical care for individual patients and at the level of rehabilitation service provision. Consequently, the Department of Rehabilitation Medicine at the University of Malaya (UM) and University Malaya Medical Centre (UMMC), together with the Cheras Rehabilitation Hospital of the Ministry of Health, and the Social Security Organisation (SOCSO) Rehabilitation Centre in Malacca have initiated a project to develop a Malaysian-wide clinical quality management system for rehabilitation (CQM-R). This project is understood as a direct response to WHO’s ”Rehabilitation 2030: A Call for Action”, and is intended to serve as a model for clinical quality management for rehabilitation worldwide.
The objective of this paper is to present the details of the Clinical Quality Management System for Rehabilitation in Malaysia (CQM-R Malaysia). First, a brief conceptual description of what constitutes a clinical quality management system based on the ICF is set out. Then, the methods, results and conclusions of a situation analysis of rehabilitation service provision conducted in January 2017 are reported. Finally, the building blocks and implementation action plan developed for CQM-R Malaysia, based on the insights gained from the situation analysis, are presented.
Quality management is a process of ensuring continuous improvement in care, and optimization of health outcomes, through a process of learning from successes and increasing the likelihood that these successes will make for stable improvements in clinical decision-making (18). As functioning is the key health indicator for rehabilitation, clinical quality management in rehabilitation is the process of continuous improvement toward the achievement of the outcome of interest, namely optimal functioning. The key to continuous quality management in rehabilitation and elsewhere is standardized information that unambiguously communicates functioning outcomes across episodes of care, as well as between research and clinical practice. For rehabilitation, continuous quality management relies on standardized reporting of functioning information and all relevant aspects of clinical practice and service provision. Functioning information that supports continuous outcome improvement is the basis for a ”learning health system”, encompassing not only clinical care, but programming and ultimately national policy (19). Table SI1 shows how functioning information can inform CQM-R Malaysia.
The goal of the situation analysis was to gain a shared understanding of provision of rehabilitation services along the continuum of care and across the perspective of the 3 ministries that provide rehabilitation services. The 3 ministries are: the Ministry of Higher Education (academic centres); the Ministry of Health (Cheras Rehabilitation Hospital and the rehabilitation services at state hospitals, district hospitals and in primary care); and the SOCSO (with its vocational rehabilitation service at Malacca).
The situation analysis was planned and coordinated by the head of the Department of Rehabilitation Medicine at UM and UMMC (LAL) and the consultant physical and rehabilitation medicine (PRM) physician responsible for the project (JPE) in cooperation with the head of clinical services of the Cheras Rehabilitation Hospital (YMY) and the Executive Director of SOCSO at Malacca (HH). The analysis was supported by a UM-visiting professor with a background in PRM, health policy and management, and expertise in applying the ICF in healthcare, and who serves as advisor to the International Society of Physical and Rehabilitation Medicine’s (ISPRM’s) liaison committee to WHO (GS). The situation analysis involved expert consultations and site visits.
At the Department of Rehabilitation Medicine, UMMC, responsible PRM consultants and rehabilitation professionals gave a structure presentation to the project leaders at this site (LAL, JPE, SA, GS) of their services, the numbers of enrolled patients, the workforce, intervention programmes and assessment tools, as well as their current and planned research agenda. The opportunities created by the hospital electronic health information system were discussed with the Deputy Director (Clinical) of the UMMC (Professor Nazirah Hasnan).
For the situation analysis at the Ministry of Health (MOH), the site visits took place at Cheras Rehabilitation Hospital and at the major district hospital at Sungai Buloh. At both locations the services provided, the assessment tools used and quality management and research efforts were presented comprehensively to the hospital leadership and the visiting experts (JPE, GS, SA). Information was provided with respect to the current and future possibilities for documentation using an electronic health information system.
For the situation analysis at SOCSO, its executive director (HH), and its responsible PRM physician (OKG) and rehabilitation manager (TEW) presented the SOCSO’s mission and presented and discussed its vocational rehabilitation programme, the current state of implementation of the ICF and assessment tools and the electronic health record system with the expert team (JPE, SA, GS).
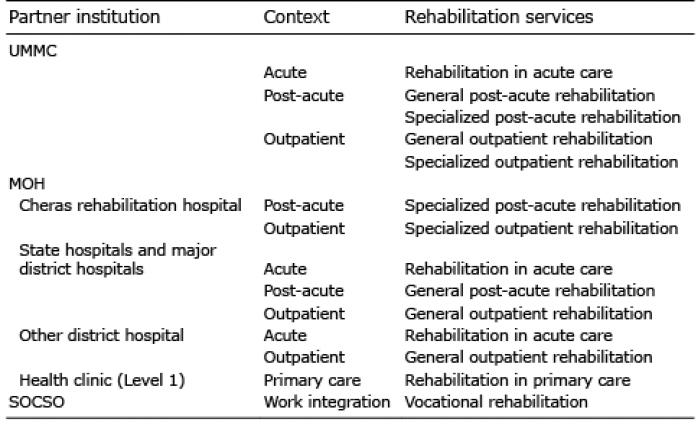
The UMMC is currently the only 1 of 5 academic medical centres in Malaysia that offers comprehensive rehabilitation services. Until now, the UMMC has also been the only training centre for PRM specialists in Malaysia; in 2018 the University Technology MARA (UiTM) will also develop rehabilitation services and a PRM trainee programme. The services at UMMC are thus representative of the services provided by academic centres under the auspices of the Ministry of Higher Education in Malaysia. These services are summarized in Table I, and a detailed description is available in Table SII1.
It was found that all rehabilitation professionals use standardized data collection tools, including clinical tests, expert assessments (e.g. the modified Barthel index (20)) and questionnaires (e.g. SF36 (21) or KOOS (22)). While the teams are well acquainted with these data collection tools, there is currently no standardized documentation system based on the ICF or standardized time-points with few exceptions.
The electronic health record system allows for the addition of forms accepted as standards by the hospital administration. Also, scoring algorithms can be implemented, allowing for immediate access to scores calculated based on data entered on a form.
Under the auspices of the MOH there is a single comprehensive free-standing rehabilitation facility; the Cheras Rehabilitation Hospital. It serves as a reference centre for rehabilitation services provided at state and district hospitals by the MOH. Table I gives an overview of the organization of health services provided by the MOH. In addition to the rehabilitation services provided at Cheras Rehabilitation Hospital, rehabilitation services are provided at state and major district hospitals under the auspices of MOH’s medical division. Under MOH’s public health division, physiotherapy and occupational therapy, but no PRM specialist care, is offered at the highest level of community-based health clinics (level 1). The rehabilitation services provided by MOH are summarized in Table I and described in detail in Table SII1.
Assessments are used according to standards defined by the MOH. In Hospital Sungai Buloh, an electronic health record system allows for selection of assessment tools for data entry, whilst at Cheras Rehabilitation this documentation is still done manually. While different facilities currently use different systems, a new health information system will be implemented across all MOH’s facilities in the next few years.
Table I. Overview of rehabilitation services in Malaysia identified in the situation analysis. They include the services provided by the University Malaya Medical Center (UMMC), the Ministry of Health (MOH) at its only freestanding rehabilitation hospital at Cheras, as well as at its 16 state and major district hospitals, other district hospital, and health clinics, and by the Social Security Organisation (SOCSO) at its Malacca facility
SOCSO is the only centre for vocational rehabilitation, work integration and disability management in Malaysia under the Ministry of Human Resources. Vocational rehabilitation is prioritized over compensation. Rehabilitation professionals document functioning with the wide range of existing ICF Core Sets, including the ICF Core Set for Vocational Rehabilitation. Also, SOCSO is developing a full Rehab-Cycle® with assessment, assignment, intervention and evaluation based on the ICF (23, 24), in light of WHO’s International Classification of Diseases (ICD) diagnosis and applying the new International Classification of Health Interventions (ICHI) (www.who.int/classifications/ichi/en/) for classifying specific interventions. SOCSO has also developed standards for what to document, when and for whom, very much in line with the envisioned development of clinical assessment schedules (CLASs) (25) for CQM-R.
Based on the widely available expertise in standardized data collection, the experience of SOCSO with applying the ICF, the coherent provision of rehabilitation services across the 3 perspectives, and the openness of the leadership across the partner organizations to cooperate in the continuous improvement of individual patient care and service provision, it was concluded that the implementation of a CQM-R in Malaysia is both important and feasible.
To implement CQM-R in Malaysia the following decisions were made: (i) to establish a governance structure involving the leadership from the 3 perspectives; (ii) to decide on a meaningful name for the project; (iii) to develop a framework for the description of rehabilitation services and the specification of CLASs for these services; (iv) to develop ICF-based standards and ICF-based data collection tools where such standards and tools are currently missing; (v) to develop the capacity for applying the ICF in CQM-R Malaysia; (vi) to align CQM-R Malaysia with other efforts towards improving quality in healthcare in Malaysia; (vii) to identify research opportunities arising from the implementation of CQM-R Malaysia; and finally, (viii) to develop an implementation action plan in light of points 1–7 for the time period 2017–2020, with an outlook of envisioned steps beyond 2020.
The governance was established in consultation with the leaders from the 3 perspectives. The leadership of the Department of Rehabilitation Medicine at UM consulted with the dean’s office at UM (Dean and Deputy Dean for research), the leadership of Cheras Rehabilitation Hospital consulted with the Director General of the MOH, and the leadership of SOCSO consulted with the Chief Executive Officer and the scientific committee for Accident Prevention, Disability Management, and Health Promotion.
The governance model consists of a steering committee, a scientific committee, general and local coordinators. The founding members of the steering committee are the head of the Department of Rehabilitation Medicine of UM and UMMC (LAL), the head of Rehabilitation Clinical Services at Cheras Rehabilitation Hospital (YMY), and the Executive Director of SOCSO Rehabilitation Center (HH).
The steering committee appointed the head of the scientific committee (JPE) for the period 2017–2020 (with the possibility of re-election). The scientific committee chair is mandated to nominate members in consultation with the 3 partners; the nominees will be confirmed by the steering committee. The steering committee also appointed a general coordinator for the project for the period 2017–2020 (SA) and will appoint coordinators at each partner organization. The steering committee will meet at least once a year; the scientific committee will meet throughout the year as needed for the scientific development and implementation of CQM-R Malaysia.
As the goal of the project is to implement a learning system at the individual level of clinical decision-making, at the level of individual rehabilitation services, and by means of benchmarking across comparable rehabilitation services, the term ”quality management” rather than the term ”quality assurance” was deemed suitable. To optimize the project’s visibility and to foster identification with the project by clinicians from the various disciplines engaged in rehabilitation, the terms clinical and rehabilitation were added resulting in the name ”Clinical Quality Management System for Rehabilitation for Malaysia” or simply ”CQM-R Malaysia”.
A prerequisite for the development of an ICF-based CQM-R is a shared understanding of current rehabilitation services provision and recommendations for the documentation of functioning. This requires the standardized description of rehabilitation services by applying a classification such as the International Classification of Services Organization in Rehabilitation (ICSO-R) (26, 27) and consensus on CLASs (25) that specify ”what ICF categories to document, for whom, and when”.
Table II shows the framework for the classification of rehabilitation services and the specification of CLASs developed by the steering group (LAL, YMY, HH), the chair of the scientific committee (JPE), the general coordinator (SA) and the advisor (GS).
Table II. Framework for the classification of rehabilitation services and the specification of clinical assessment schedules (CLASs). For each of the 7 types of rehabilitation services and corresponding specializations of rehabilitation services (7 specialized post-acute rehabilitation services and 8 specialized outpatient rehabilitation services) a proposal for a default ICF Set and a proposal for optional the International Classification of Functioning, Disability and Health (ICF) sets are shown. They will serve as the starting point for national consensus conferences aiming to specify the CLASs for these rehabilitation services
From a health system perspective, 7 types of rehabilitation services were identified, ranging from rehabilitation in acute care to general and specialized rehabilitation in post-acute and outpatient care, rehabilitation in primary care and vocational rehabilitation. For specialized post-acute rehabilitation 7 subtypes of rehabilitation services and for specialized outpatient rehabilitation 8 subtypes were identified (Table II).
The description of rehabilitation services including both a classification-based and a narrative description of the 7 main types and 7 plus 8 subtypes of rehabilitation services will be developed in 2017 under the auspices of the steering group in close collaboration with the developers of ICSO-R (26, 27). The proposed descriptions will be discussed and possibly modified in consensus conferences in 2018. It is envisioned that 7 conferences will be held to reach agreement on the descriptions of the 7 main types and the 7 subtypes for specialized post-acute rehabilitation and 8 subtypes for specialized outpatient rehabilitation. The conferences for specialized post-acute rehabilitation and specialized outpatient rehabilitation will include consensus-building for 7 and 8 subtypes, respectively. To achieve a coherent set of CLASs it is envisioned that experts across specific health conditions will be involved in the consensus building for a specific health condition.
Table II presents the proposed ICF categories to be included in CLASs (25) for the 7 types and 7 plus 8 subtypes. The proposed domains for CLASs, as shown in Table II, will be discussed and possibly modified in the consensus conferences in 2018. These conferences will apply a method developed by the ICF Research Branch in cooperation with the UEMS PRM Section and Board (12, 25).
In addition to reviewing and potentially modifying the proposed ICF categories to be included in CLASs, participants will be asked to reach agreement on the time-points at which the proposed ICF categories should be documented and to develop recommendations for data collection in specialized rehabilitation beyond documentation of the ICF Generic-30 Set.
Tables SIII and SIV1 show the description of use and ICF categories of the ICF Generic-6 Set, the ICF Generic-7 Set and the ICF Generic-30 Set, respectively. To illustrate the combined documentation applying the ICF Generic-30 Set together with ICF Core Sets for specialized rehabilitation, Table SIV1 illustrates the example of Spinal Cord Injury. The proposed documentation for vocational rehabilitation, the Brief ICF Core Set for Vocational Rehabilitation with 13 categories, and the Derived ICF Core Set for WORQ with 44 categories, that served as basis for the development of the Work Questionnaire (WORQ) (28, 40) are shown.
The situation analysis showed that for 2 indications there is no currently available ICF Core Set: amputee rehabilitation in specialized outpatient rehabilitation, and paediatric specialized rehabilitation both in the post-acute and outpatient context.
A PRM consultant of the department of rehabilitation medicine at UMMC (CTY) together with the general coordinator (SA) will therefore cooperate in the final studies toward developing the ICF Core Set for Amputee Rehabilitation under the auspices of the International Society of Prosthetics and Orthotics (ISPO) (49).
By the same token, the department will support the ICF Research Branch in its effort to develop a preliminary version of an ICF Core Set for Pediatric Rehabilitation based on current experiences with the development of ICF Core Sets for children and youth with cerebral palsy (52).
The situation analysis also showed that there is a need for a clinical data collection tool that is simple and can be used across rehabilitation services in Malaysia. Therefore it was decided to develop a translation of the ICF Clinical Data Collection Tool for Bahasa Malaysia based on an established protocol (13, 15). Since most health professionals speak English or Bahasa Malaysia with patients who are native speakers of Tamil and Mandarin, it was not considered a necessity at this point to develop a language version in Tamil and Mandarin. If necessary a Tamil and Mandarin version can be developed later.
To increase user acceptance, it was decided to use the name ”ICF Clinical Tool” rather than ”ICF Clinical Data Collection Tool” (13, 14).
With respect to vocational rehabilitation there was a decision to consider the use of the work questionnaire (Work Rehabilitation Questionnaire (WORQ); http://myworq.org/) (26) developed in collaboration with the International Labor Organization (ILO) and the ICF Research Branch. In the near future it will be possible to report data collected with WORQ for the ICF categories of the Derived ICF Set for the WORQ (28, 40) in 44 categories, which include the 13 categories of the Brief ICF Core Set for Vocational Rehabilitation (40) using transformation tables that will be developed for Malaysia based on Rasch methodology (11, 53, 54). As the WORQ can be both expert- and self-administered it allows for follow-up of patient’s functioning after a stay at SOCSO vocational rehabilitation through postal questionnaires. The development of a translation of the WORQ for Bahasa-Malaysia and the development of country modification of the English reference version and the Chinese-Mandarin reference version for Malaysia can follow an established protocol and will be supported by the ICF Research Branch and the lead developer of the WORQ (Professor Reuben Escorpizo).
The situation analysis showed that SOCSO had the most in-depth ICF training of its staff. UMMC had ICF training for its leaders, as did MOH. It was therefore decided to implement a systematic training programme for the ICF and CQM-R.
As a first step a train-the-trainer workshop will be given by the coordinator of the ICF Research Branch (Melissa Selb). It is intended to involve trainers representing the various rehabilitation professionals across the 3 partner organizations to ensure target group-specific training.
The second step foresees the development of a training programme for CQM-R developed jointly by the 3 partners of CQM-R Malaysia and the ICF Research Branch. Through the development of joint training materials and regular training for new staff a coherent implementation of CQM-R Malaysia can be assured.
The situation analysis highlighted the role the Malaysian Society for Quality in Health (MSQH) should play in the implementation of CQM-R Malaysia. MSQH is recognized as the national accreditation body and standards for healthcare facilities and services. MSQH is dedicated to improving the quality of Malaysia’s healthcare through voluntary accreditation. Specific to Rehabilitation Medicine Services (Service Standard 17 in MSQH 5th Edition draft), the quality indicators cover a wide range of aspects, including documentation as to whether functioning is being assessed in a timely manner. Therefore, CQM-R is complementary to MSQH, as it provides a measurement-improvement system for functioning.
At UMMC the situation analysis also resulted in the identification of reporting requirements for ongoing cohort studies in the area of tuberculosis. While we identified no direct overlap, the potential redundancy of information needs to be considered in the implementation phase.
Based on the presentations by the various teams at UMMC it became clear that many data collection efforts in the context of research projects could greatly benefit from a standardized documentation of functioning information.
Firstly, standardized documentation for rehabilitation services using CLASs allows for clinical epidemiological analysis of functioning outcomes in relation to person and health condition characteristics as well as inputs in terms of rehabilitation interventions and modifications of the environment and strengthening of the resources of the person.
Secondly, it allows for quasi-experimental studies; for example, a year-by-year comparison of outcomes occurring, with documented changes in clinical rehabilitation care provision. It will be possible to make concrete changes in clinical rehabilitation care by adding, for example, a new intervention and to compare the outcomes with the outcomes of previous years.
Thirdly, it will be possible to efficiently implement nested projects; that is, more in-depth data collection in addition to the standard data collection required as dependent or independent variables for a specific project with a concrete hypothesis. Also, randomized trials become feasible with this model.
Table SI1 shows the implementation action plan integrating the key elements described above. The most important consideration for implementation is a stepwise process at the clinical and service level, as summarized in Table III.
At the clinical level, the first goal is to systematically implement standardized data collection with the ICF Clinical Tool across rehabilitation services, as shown in Table II for the time-points specified in the consensus conferences in 2018.
Table III. Clinical quality management at the clinical and rehabilitation service level (informed by Table I in Stucki G, Bickenbach J. Functioning information in the learning health system. Eur J Phys Rehab Med 2017; 53: 139–143)
The implementation of rehabilitation management, including a rehabilitation plan with sequential rehabilitation cycles, will be achieved through a demonstration project for SCI rehabilitation in close collaboration with a similar project at Swiss Paraplegic Research (SPF) and the Swiss Paraplegic Center (SPZ). Informed by this project, other multi-disciplinary teams engaged in specialized post-acute and outpatient rehabilitation will be encouraged to implement an ICF-based rehabilitation management programme.
Following the implementation of CQM-R at the clinical level, planned for 2017–2020, it is envisioned that measurement-for-improvement systems for individual rehabilitation services will be implemented. This will be coordinated with the possible governmental efforts to develop and implement benchmarking across rehabilitation programmes with the goal of learning how to achieve best-functioning outcomes. To inform these developments, SOCSO is considering a demonstration project on implementing a measurement-for-improvement system for an individual rehabilitation service, as it can rely on an already implemented ICF-based documentation system.
The project presented here provides a sound basis for the system-wide implementation of CQM-R in Malaysia at all levels, ranging from clinical decision-making to continuous improvement of individual rehabilitation services and benchmarking across Rehabilitation Service Programmes.
To the best of our knowledge the implementation of CQM-R Malaysia is the first of its kind worldwide, as it aims to develop a countrywide and ICF-based measurement improvement system at both the clinical and service level. The CQM-R Malaysia project is also unique as it comprehensively integrates rehabilitation services under the auspices of the Ministry of Higher Education, the MOH, and the Ministry of Human Resources with its Social Security Organisation.
As this is a pioneer project it will encounter a number of challenges. The first challenge is the application of ICSO-R (26, 27), a classification that is currently being refined. The collaboration with the developers of ICSO-R will ensure that the description of rehabilitation services in Malaysia is closely aligned with ICSO-R. In turn, the Malaysian experience in applying the current version of ICSO-R is expected to provide valuable lessons on how to improve the classification.
Secondly, the method for developing CLASs currently relies on a single experimental workshop (25). Consequently, this methodology will need to be developed further during the consensus conferences planned for 2018. The experience of conducting the consensus conferences in Malaysia is expected ultimately to inform the development of a protocol that can be used by countries worldwide aiming for the system-wide implementation of the ICF in rehabilitation as well as the implementation of a national CQM-R.
Thirdly, the implementation will rely on both paper-based and electronic documentation, depending on the IT options offered at the different facilities. Having 2 different modes of documentation provides the opportunity to qualitatively study the similarities and differences, as well as the utility of these 2 implementation modes in implementing the ICF and CQM-R. The lessons learned from Malaysia can then be shared with the international scientific community. Moreover, the experience of integrating ICF tools in existing electronic health record systems could provide valuable practical information to other medical specialties interested in the documentation of functioning including primary care, geriatrics and anaesthesiology.
The project also provides the opportunity to further strengthen rehabilitation in practice, science and governance, and to spearhead the implementation of the ICF in health information systems, both at the clinical and national statistical level. It also emphasizes the importance of functioning information beyond the rehabilitation community to stakeholders of the healthcare system at large, including policymakers.
The proposal for implementing the ICF in rehabilitation and CQM-R in Malaysia presented in this paper is only the starting point for scaling up rehabilitation services in Malaysia. It promotes the flexibility of adding rehabilitation services or modifying currently offered services and the continuous improvement of the health system at all levels by learning from its implementation experience. Last but not least, in line with WHO’s ”Rehabilitation 2030: A Call for Action”, the Malaysian proposal can also serve as a model framework for other countries that are striving to scale up rehabilitation services.


 Click to show fullsize
Click to show fullsize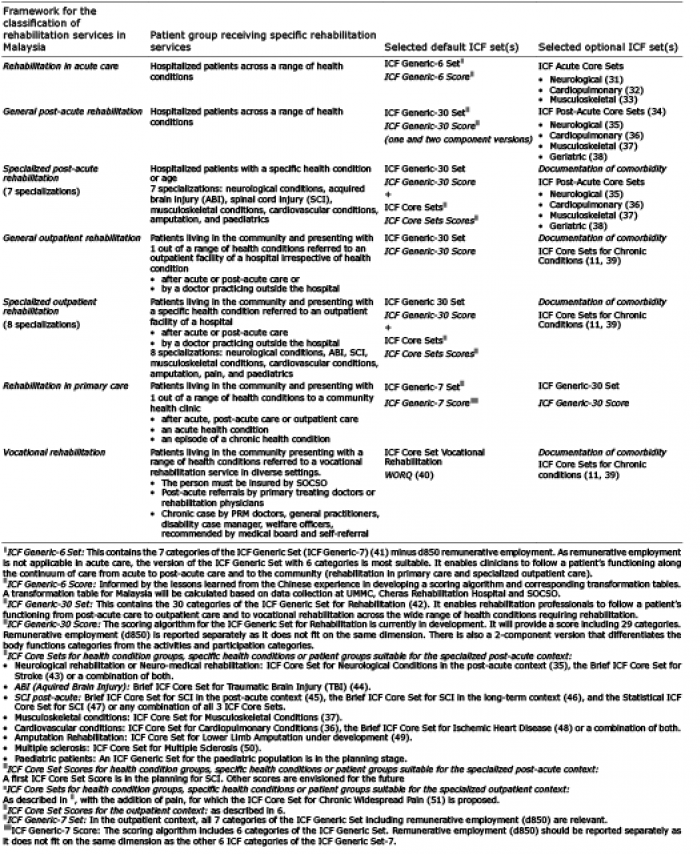 Click to show fullsize
Click to show fullsize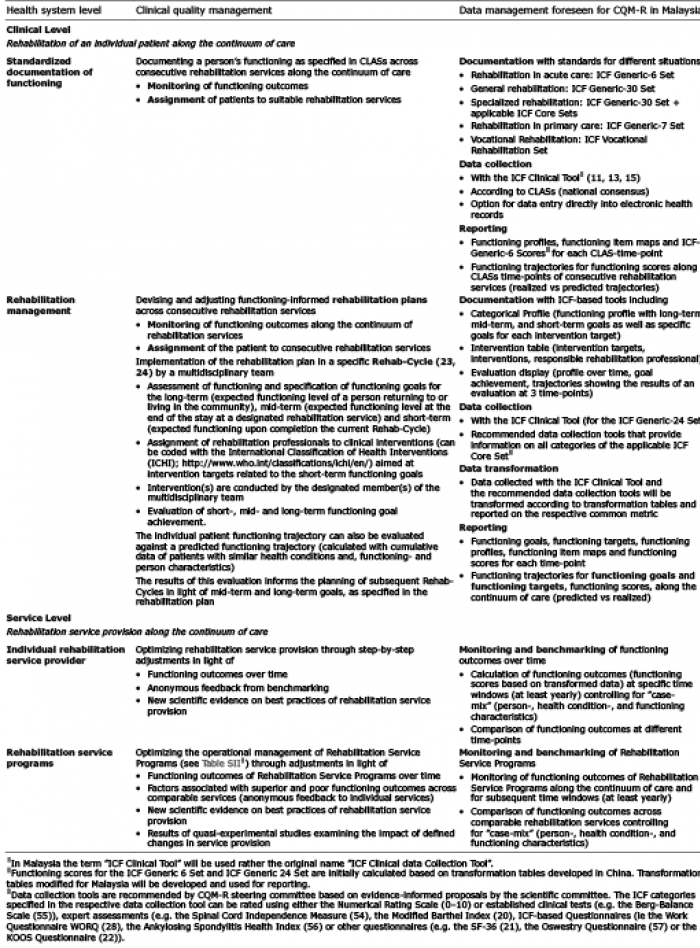 Click to show fullsize
Click to show fullsize