
From the 1School of Medicine, University of Manchester, Manchester, 2School of Medicine and Leeds Institute for Data Analytics, University of Leeds, 3Academic Department of Rehabilitation Medicine, University of Leeds and National Demonstration Centre of Rehabilitation Medicine, Leeds Teaching Hospitals NHS trust, 4Department of Infectious Diseases, Leeds Teaching Hospitals NHS Trust, Leeds, 5Department of Rehabilitation Medicine, Hull University Teaching Hospitals NHS Trust, Hull, 6Intensive Care Unit, Leeds Teaching Hospitals NHS Trust, Leeds, UK and 7Division of Neuroscience and Experimental Psychology, University of Manchester, Manchester, UK
*Joint first authors
Objective: To determine long-term clinical outcomes in survivors of severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) coronavirus infections after hospitalization or intensive care unit admission.
Data sources: Ovid MEDLINE, EMBASE, CINAHL Plus, and PsycINFO were searched.
Study selection: Original studies reporting clinical outcomes of adult SARS and MERS survivors 3 months after admission or 2 months after discharge were included.
Data extraction: Studies were graded using the Oxford Centre for Evidence-Based Medicine 2009 Level of Evidence Tool. Meta-analysis was used to derive pooled estimates for prevalence/severity of outcomes up to 6 months after hospital discharge, and beyond 6 months after discharge.
Data synthesis: Of 1,169 identified studies, 28 were included in the analysis. Pooled analysis revealed that common complications up to 6 months after discharge were: impaired diffusing capacity for carbon monoxide (prevalence 27%, 95% confidence interval (CI) 15–45%); and reduced exercise capacity (mean 6-min walking distance 461 m, CI 450–473 m). The prevalences of post-traumatic stress disorder (39%, 95% CI 31–47%), depression (33%, 95% CI 20–50%) and anxiety (30%, 95% CI 10–61) beyond 6 months after discharge were considerable. Low scores on Short-Form 36 were identified beyond 6 months after discharge.
Conclusion: Lung function abnormalities, psychological impairment and reduced exercise capacity were common in SARS and MERS survivors. Clinicians should anticipate and investigate similar long-term outcomes in COVID-19 survivors.
Key words: coronavirus infection; follow-up; follow-up studies; COVID-19; prevalence; lung function; exercise tolerance; post-traumatic stress disorder; depression; anxiety; fatigue; quality of life; SARS; MERS, ARDS.
Accepted May 19, 2020; Epub ahead of print May 25, 2020
J Rehabil Med 2020; 52: jrm00063
Correspondence address: Dr Manoj Sivan MD FRCP Ed, Academic Department of Rehabilitation Medicine, Martin Wing, Leeds General Infirmary, LS1 3EX. E-mail: m.sivan@leeds.ac.uk
Severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome (MERS) are two previous viral infection outbreaks similar to the current COVID-19 pandemic. Studies that have looked at long-term health problems in survivors of these two outbreaks report reduced lung function and reduced ability to exercise in some survivors up to 6 months after discharge from hospital. Mental health problems including stress, an-xiety and depression were observed in up to one-third of survivors at 6 months and beyond. The quality of life was observed to be low even 12 months after discharge from the hospital. Rehabilitation clinicians and services should anticipate similar health problems in survivors of COVID-19, investigate them accordingly and plan suit-able and timely treatments to enable best possible recovery and quality of life for them.
Severe acute respiratory syndrome (SARS), Middle East respiratory syndrome (MERS) and coronavirus disease 2019 (COVID-19) are 3 major coronavirus (CoV) outbreaks that have occurred in the 21st century (1). SARS, caused by SARS-CoV, originated in China in 2002 and MERS, caused by MERS-CoV, originated in Saudi Arabia in 2012 (1). Like COVID-19, caused by SARS-CoV-2 (2), both of these diseases are members of the same virus family and result in viral pneumonia and may lead to acute respiratory distress syndrome (ARDS) (1, 3).
Alongside acute challenges, the SARS and MERS outbreaks resulted in significant long-term clinical problems for survivors, with implications for rehabilitation services and healthcare utilization (4, 5). Whilst there are currently no long-term follow-up studies investigating COVID-19, these long-term outcomes have been documented in survivors of SARS and MERS. Lessons should be learned from these previous outbreaks and used to predict potential long-term (> 3 months) complications of COVID-19 in survivors.
The aim of this review is to determine the long-term clinical complications for survivors of SARS and MERS after hospitalization and intensive care unit (ICU) admission. The findings of this review will inform rehabilitation clinicians in anticipating similar problems in COVID-19 survivors and planning interventions and services for timely input and restoration of function in these individuals.
The protocol for this systematic review and meta-analysis has been published on PROSPERO (ID: CRD42020179002).
Data sources and search strategy
A search of current literature was carried out in 4 databases: MEDLINE (1946 to March week 3 2020), EMBASE (1974 to 31 March 2020), CINAHL Plus (1937 to March week 3 2020), and PsycINFO (1806 to March week 3 2020). The search strategy was: (Coronavirus OR Coronavirus Infections OR SARS virus OR Severe acute respiratory syndrome OR MERS OR Middle east respiratory syndrome OR COVID) AND (Follow-up OR Follow-up studies OR Prevalence). Terms were entered as MeSH terms, where available, for each database, otherwise these were searched as keywords in the title, abstract, and subject headings.
Inclusion and exclusion criteria
Population. Clinical studies involving adults with a confirmed diagnosis of SARS or MERS were included.
Exposure. Studies reporting patients with SARS or MERS were included.
Study Studies had to follow up patients for a minimum of 3 months post-admission or 2 months post-discharge to be included in this review. Only primary research studies were included. Reviews, case-reports, and editorial reports were excluded.
Outcomes. Studies were required to monitor changes in clinical symptoms at follow-up in order to be included. Studies that only monitored changes in serological or immunological results without any assessment of clinical status of the patient were excluded. Likewise, studies reporting only radiological appearance of lung disease or osteonecrosis without any mention of any clinical outcomes were excluded.
Selection process
All studies were first screened using the title and abstract. At this stage abstracts with any mention of follow-up were included to avoid exclusion of abstracts that did not report the length of follow-up. Similarly, abstracts that reported follow-up for any outcome were accepted in order to allow inclusion of studies in which clinical findings were not significant and therefore not reported in the abstract. Full texts of selected abstracts were then screened to ensure that all of the above selection criteria were met.
The final included studies were then critically appraised and graded. Screening and grading were undertaken by 4 independent reviewers (KP, HA, MS, and SH). Author DG was involved in cases of disagreement
Data extraction
Data were extracted into standardized tables for each medical system. The following data were extracted: study, year, country, type of coronavirus outbreak, sample size, follow-up rate, age, sex, settings (hospital/ICU admission), follow-up period, prevalence of key outcomes, and mean score for assessment of each outcome. Where estimates were only provided separately for 2 or more subgroups, the weighted average across those subgroups was taken as the estimate for the overall population. Extraction was performed by at least 2 independent authors and further cross-checked by 2 other authors.
Quality assessment
Studies were graded using the Oxford Centre for Evidence-Based Medicine (OCEBM) 2009 Level of Evidence Tool (Table SI) (6). The initial level of evidence was assigned depending on the type of study. Prospective cohort studies were then downgraded if the follow-up rate was < 80%.
Data analysis
Binary data for prevalence of outcomes were pooled using meta-analysis by mixed-effects logistic regression, directly modelling the number of subjects with impaired function using a binomial distribution. Mean scores for different outcomes were pooled in a meta-analysis using random effects models (7). Forest plots were stratified by duration of follow-up (up to 6 months and over 6 months). Where a study presented more than one result within a subgroup, the value closest to 6 months (for up to 6 months) or to closest to 12 months (for over 6 months) was selected. Between-study heterogeneity was assessed as the range of study estimates and the proportion of total variability attributable to between-study heterogeneity (8). There were too few studies to formally explore the sources of heterogeneity through meta-regression (e.g. by mean age, disease, % male, or level of evidence) or to examine potential small-study effects, such as publication bias through funnel plots. All statistical analyses were conducted using Stata version 15 (9).
Role of the funding source
There was no funding source for this study.
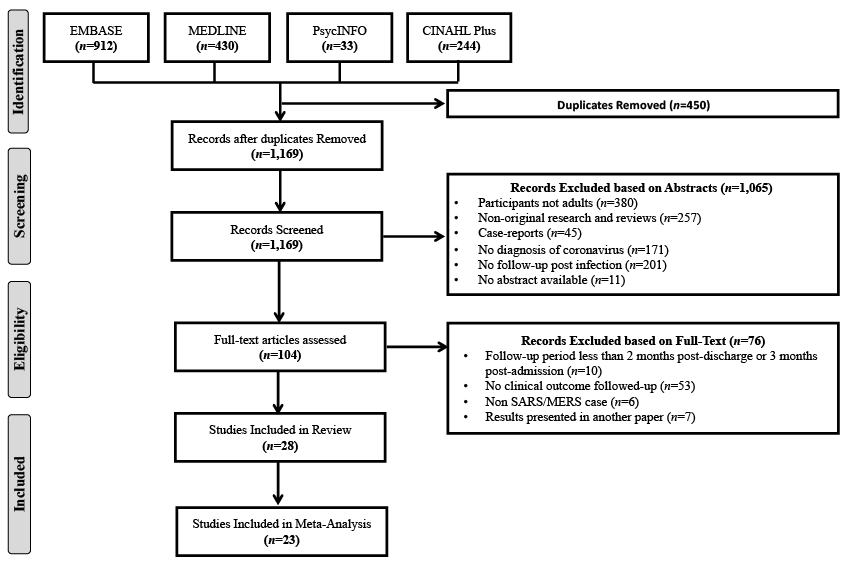
A total of 1,169 studies were identified from the databases. Of these, 104 abstracts were selected for full-text screening and a final total of 28 studies were included in the systematic review and 23 included in the meta-analysis. The reasons for exclusion are reported in Fig. 1.
Fig. 1. PRISMA Flowchart for the Literature Search.
Out of the 28 studies included in this review, 26 reported findings from the SARS outbreak and 2 reported findings from the MERS outbreak. The cohorts studied were from Beijing (11 studies), Hong Kong (9 studies), Guangzhou (1 study), Singapore (2 studies), Taiwan (2 studies), Korea (2 studies), and Canada (1 study), which were the regions that were severely affected by the previous outbreaks. The sample size ranged from a case series of 4 patients to a cohort study of 406 patients. Based on OCEBM grading, 15 studies were graded Level 1b, 8 Level 2b, 2 Level 3b, and 3 Level 4.
The 28 studies in the review reported outcomes involving multiple organ systems.The studies mainly addressed one or more of 5 key outcomes of interest: lung function (18 studies), mental health (6 studies), exercise tolerance (5 studies), health-related quality of life (HRQoL) (5 studies), ocular outcomes (1 study), and neuromuscular outcomes (1 study). The study characterstics and results for each key outcome of interest are presented in Tables I–V. Additional data for lung function, mental health, and quality of life are shown in Tables SII–SIV.
Table I. Lung function outcomes in coronavirus survivors
Table II. Exercise tolerance outcomes in coronavirus survivors
Table III. Mental health outcomes in coronavirus survivors
Table IV. Quality of life outcomes in coronavirus survivors
Table V. Miscellaneous outcomes in coronavirus survivors
A total of 18 studies (9 Level 1b, 4 Level 2b, 3 Level 3b, and 2 Level 4 studies) reported lung function outcomes in CoV survivors, of which 16 were included in the meta-analysis. Chen et al. (11) only reported changes in symptoms without any report of lung function parameters which could be included in this meta-analysis. Zheng-Yu et al. (14) did not report standard deviations, hence the data could not be used in the meta-analysis. All studies defined an abnormality in each lung function parameter as a value of < 80% of the predicted value. Studies reporting prevalence of abnormality in diffusing capacity of the lung for carbon monoxide (DLCO) (10 studies), forced expiratory volume in 1 s (FEV1) (6 studies), forced vital capacity (FVC) (5 studies), and total lung capacity (TLC) (4 studies) were used to obtain pooled prevalence of each abnormality (Fig. 2 and Fig. S11). At 6 months post-discharge, abnormalities in DLCO, FVC, and TLC were more prevalent than abnormalities in FEV1. Most of these abnormalities improved after 6 months after discharge; however, the prevalence of DLCO impairment remained considerably high even 6 months beyond discharge, with a pooled estimate of 24.35 (95% confidence interval (95% CI) 11.05–45.46). Studies reporting mean values for DLCO (10 studies), FEV1 (10 studies), FVC (10 studies), FEV1/FVC (6 studies), vital capacity (VC) (4 studies), diffusing capacity of the lung for carbon monoxide: alveolar ventilation (DLCO:Va) (3 studies), and TLC (8 studies) were used to pool mean values for each abnormality up to and beyond 6 months after discharge (Fig. S21). None of the pooled estimates for the mean values of these parameters were <80% of predicted.
Fig. 2. Summary Forest plot showing pooled estimate of prevalence of different lung function abnormalities in CoV survivors up to 6 months (top) and over 6 months (bottom).
Five studies (4 Level 1b studies and one Level 2b study) reported exercise tolerance outcomes in CoV survivors, of which 4 were included in this meta-analysis (Fig. S31). Results from Ong et al.’s study (27) were not included because they only reported outcomes from cardiopulmonary exercise testing (CPET) and did not conduct 6-min walking distance (6MWD) tests. The pooled estimate of 6MWD for 3 studies reporting outcomes up to 6 months was 461.18 (95% CI 449.66–472.71). The 6MWD increased substantially after 6 months, with pooled estimate of 533.00 (95% CI 449.66–472.71). Since ~30 m is considered to be the minimal clinically important difference in 6MWD (37), patients seem to improve significantly over time. Unfortunately, data were not available regarding the 6MWD for participants before CoV infection, and therefore there is no report of the number of patients with exercise tolerance lower than baseline.
Six studies (5 Level 1b and one Level 2b study) reported psychological comorbidities in CoV survivors, of which all 6 were included in the meta-analysis. All studies that reported prevalence of these psychological conditions had follow-up periods longer than 6 months. As a result, meta-analysis was conducted for prevalence beyond 6 months post-discharge only. The prevalence of different psychological conditions was substantially high, with pooled estimates of 38.80% (95% CI 30.93–47.31) for post-traumatic stress disorder (PTSD), 33.20% (95% CI 19.80–50.05) for depression, and 30.04% (95% CI 10.44–61.26) for anxiety (Fig. 3 and Fig. S41). It was not possible to perform meta-analysis on the mean scores for different psychological comorbidities because different scales were used to report these in different studies.
Fig. 3. Summary Forest plot showing pooled estimate of prevalence of different psychological conditions in CoV survivors over 6 months
Five studies (4 Level 1b studies and one Level 2b study) reported quality of life outcomes in CoV survivors. Of these, only 3 studies, which reported both mean and SD, were included in the meta-analysis of Short Form 36 health survey (SF-36) (Fig. S51) and St George’s Respiratory Questionnaire (SGRQ) (Fig. S61) each. Pooled analysis showed that the mean score for all of the 8 domains of the SF-36 were substantially lower in CoV survivors than normative values for people who are healthy, as well as for people with chronic diseases derived from existing validated literature (38) (Fig. 4). Domains that scored particularly lower than healthy individuals and those chronic conditions were role limitations due to physical and emotional health. There seems to be some improvement in these domains beyond 6 months, but the scores were still lower than healthy and chronic disease patients (38).
Other outcomes that have been followed-up in SARS patients are reported in Table V. A 2004 study by Yuen et al. (35) found no eye pathologies in this cohort. A 2004 case series study by Tsai et al. (36) followed up patients who developed limb weakness related to critical illness neuropathy (CIN) and myopathy (CIM) and sensory deficits following infection. All these patients had partial or full recovery of muscle power 3 months after admission.
Fig. 4. Radar plot showing pooled estimate of mean scores for different domains of SF-36 in coronavirus survivors up to 6 months (green) and over 6 months (orange) compared to healthy individuals (blue) and subjects with chronic conditions (red).
This systematic review collates the long-term (> 3 month) complications following SARS and MERS in patients who required hospitalization or ICU stay. HRQoL, measured using SF-36, was considerably reduced in survivors at 6 months post-infection, and showed only slight improvement beyond 6 months. HRQoL of survivors remained below that of the normal population and of those with chronic conditions (Fig. 4). Since these SF-36 scores reflect impairment in physical, mental, and social functioning of well-being, it is not surprising that the key areas of impairments identified in our systematic review were pulmonary dysfunction, reduced exercise tolerance, and psychological problems.
Respiratory compromise is one of the key physical issues in survivors of SARS and MERS. The impairment is mainly restrictive in nature, with predominance of abnormalities in DLCO, VC, and TLC, compared with FEV1, thereby supporting the aetiopathology of ARDS with parenchymal infiltration caused by the infection. Even though lung function improves over time, the results of the current meta-analysis showed that reduction in DLCO may still be present in 11–45% of CoV survivors at 12 months. This is consistent with CT findings from other studies, which have reported that pulmonary fibrosis can persist for up to 7 years (26). Considering that pulmonary rehabilitation has shown positive results in patients with fibrosis, such intervention, if employed at an early stage, has the potential to improve outcomes long-term (39).
SARS survivors had reduced aerobic capacity, with peak oxygen uptake (VO2max) testing showing impairments in 41% of patients at 3 months (27). This could be due to circulatory limitation, muscle weakness, critical illness neuropathy and myopathy (CINM), and deconditioning (27). The 6MWD is also reduced in SARS and MERS survivors at 3 months and slowly improves by 12 months (13, 16). Such chronic weakness may be present in patients even 5 years after ICU admission; therefore, the rehabilitation needs of these patients can be prolonged (40). Early rehabilitation combining mobilization with strengthening exercises may improve exercise tolerance in these patient groups, as there is substantial evidence for improvement in weakness and functional independence in CINM (41).
The current meta-analysis showed that approximately one-third of SARS and MERS survivors may have psychological conditions, such as PTSD, depression, and anxiety beyond 6 months. These estimates are much higher than the prevalence of these conditions reported as part of post-ICU syndrome in medical and surgical patients (42). This indicates that the long-lasting mental health impact is not from serious illness alone, but also from factors such as fear (43), stigma (34) and difficulties and compliance with quarantine (44), and the psychological impact of the quarantine experience.
SF-36 scores for role limitations in SARS survivors were particularly low compared with healthy individuals. A 2007 study by Tansey et al. (12) reported that 17% of SARS survivors had not returned to their previous level of working even at one year post-infection. Many of the symptoms experienced by SARS survivors could be responsible for such reduced social functioning. Fatigue was reported in at least one-third of the patients in 2 studies, with a follow-up period of 18 months (33) and 40 months (34), respectively. Pain disorders were followed up in one study, which reported that these were present in approximately one-third of patients around 3.5 years after SARS infection (34).
Differences in outcomes between ICU and non-ICU patients remain unclear. Whilst one study identified that lung function parameters, such as FVC and DLCO, were comparatively lower in the ICU group (13), another reported no significant difference between the 2 groups (27). It is known that muscle weakness developed during ICU admission has been associated with substantial impairments in physical function and quality of life following acute lung injury (45), and therefore it could be hypothesised that SARS and MERS ICU survivors may have suffered worse outcomes.
The main strength of this study is that it highlights multiple long-term biopsychosocial impairments which may hinder return to pre-infection functional status. This is the first systematic review and meta-analysis on this topic as far as we are aware. Unlike a previous review from 2003 (4), we investigated long-term outcomes from major SARS and MERS outbreaks this century. We have tried to capture the various aspects of well-being and health-related quality of life in CoV survivors.
A weakness of our review was the large between study heterogeneity of studies included - almost all I-squared estimates >50%. and a wide range of results observed across studies. Pooled estimates must therefore be interpreted cautiously, particularly when comparing the data up to 6 months with the results over 6 months. We were unable to formally explore sources of this heterogeneity because of the small numbers, but these could include study-level differences in mean ages, gender, differences between SARS and MERS outbreaks, referral pathways between regions, and study design.
At this stage it is not possible to conclude whether the long-term outcomes identified in SARS and MERS patients will also occur in COVID-19 survivors. However, as SARS and MERS belong to the same family of virus as COVID-19, and the clinical features are similar (1, 3), as well as providing a critical assessment of the risk factors and actionable items for stopping their spread, based on the lessons learned from the first 2 deadly coronavirus outbreaks, as well as results from initial reports on the current COVID-19 coronavirus pandemic, clinicians should anticipate a similar range of long-term outcomes in survivors of COVID-19 following hospitalization and ICU admission. Further studies should therefore be performed in these patients in order to follow up lung function abnormalities, reduced exercise capacity, psychological impairments, and reduced quality of life, as identified in SARS and MERS patients. Practical approaches are recommended early in the COVID-19 outbreak to mitigate against the potential long-term outcomes identified in the current review. Acute multidisciplinary rehabilitation during hospital stay, post-acute rehabilitation in step-down rehabilitation or respiratory units and long-term rehabilitation interventions are recommended to optimize physical, psychological and functional recovery in these individuals. In summary, it is clear from the SARS and MERS epidemics that clinicians should monitor the survivors of COVID-19 for the range of physical and mental health impairments identified in this review, in order to manage them appropriately.
The authors thank Huifeng Zhang (University of Leeds), Zuyao Yang (Chinese University of Hong Kong), Shuting Wang (Chinese University of Hong Kong), Yu-Kang Tu (The National Taiwan University), and Queenie Chan (Imperial College) for their help with tracing and translating some of the full text articles.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize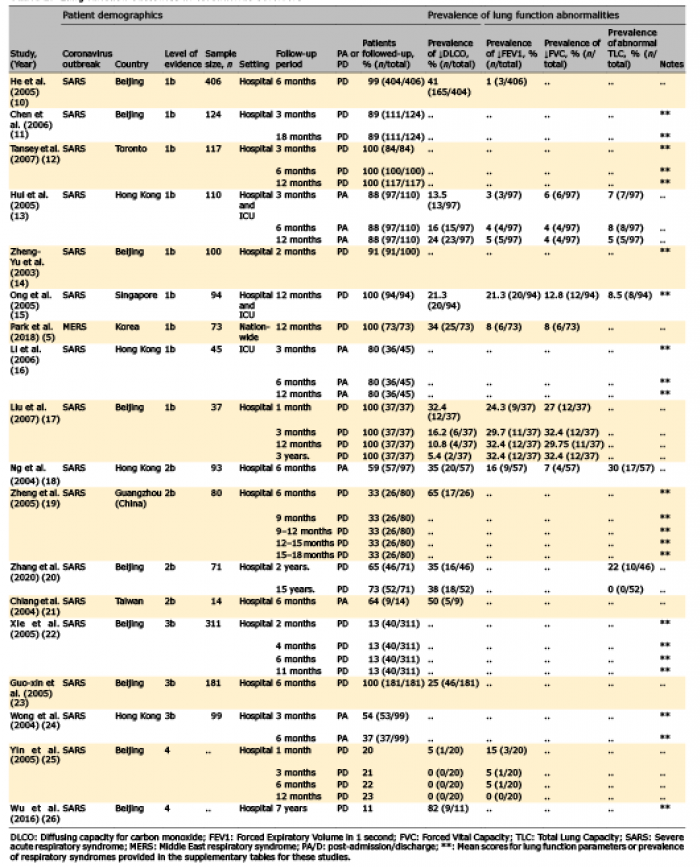 Click to show fullsize
Click to show fullsize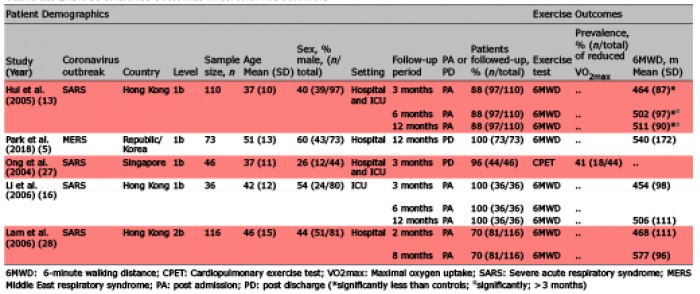 Click to show fullsize
Click to show fullsize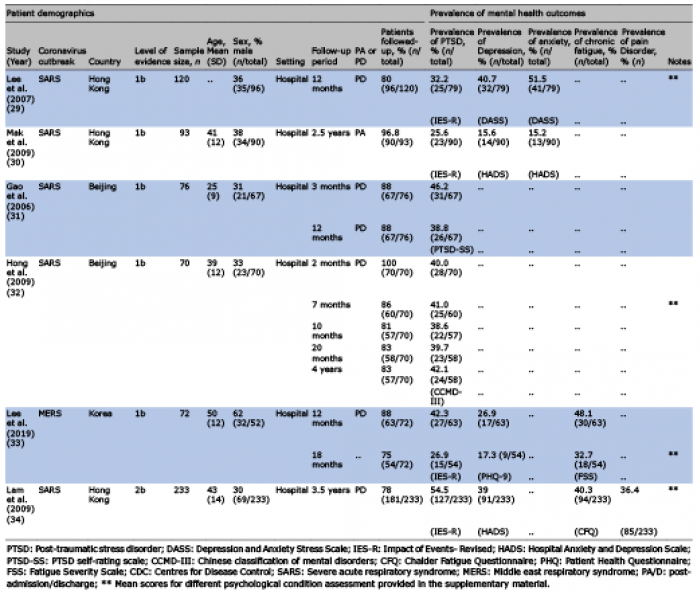 Click to show fullsize
Click to show fullsize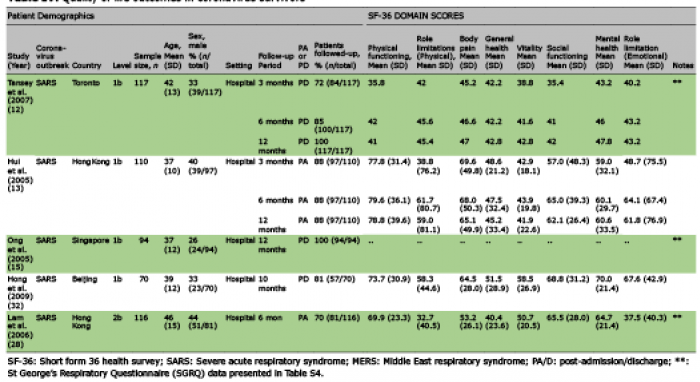 Click to show fullsize
Click to show fullsize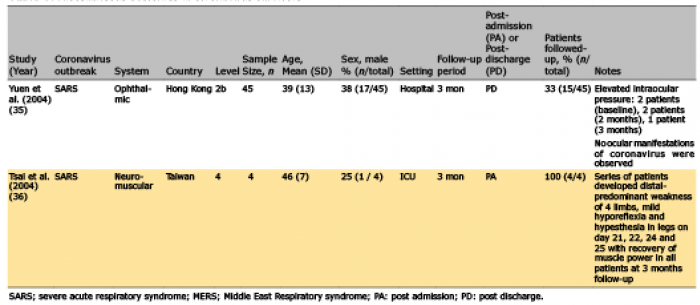 Click to show fullsize
Click to show fullsize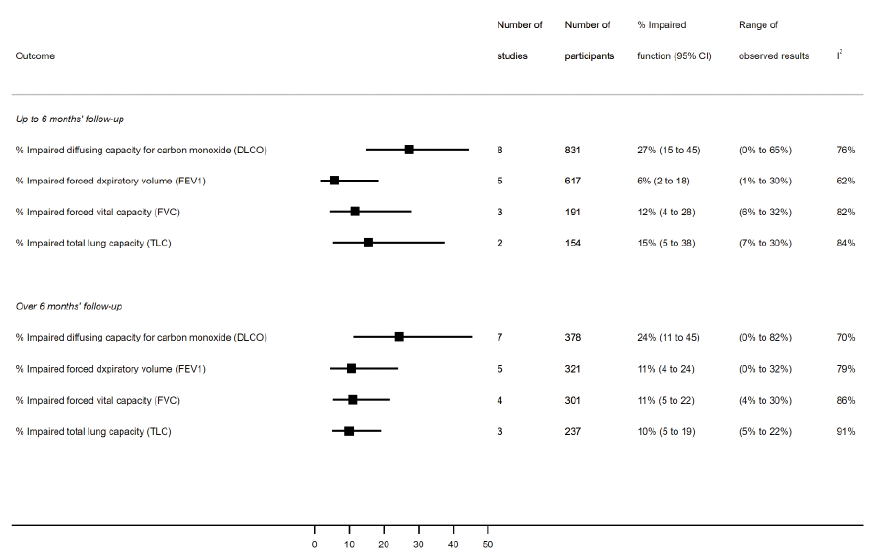 Click to show fullsize
Click to show fullsize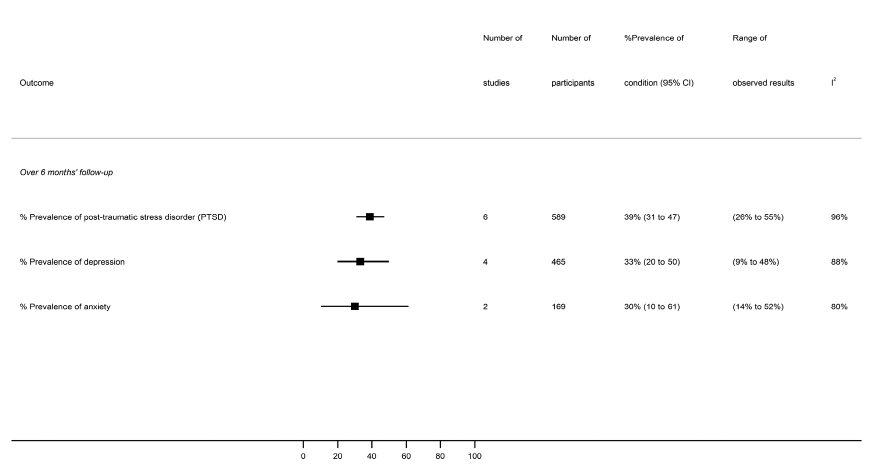 Click to show fullsize
Click to show fullsize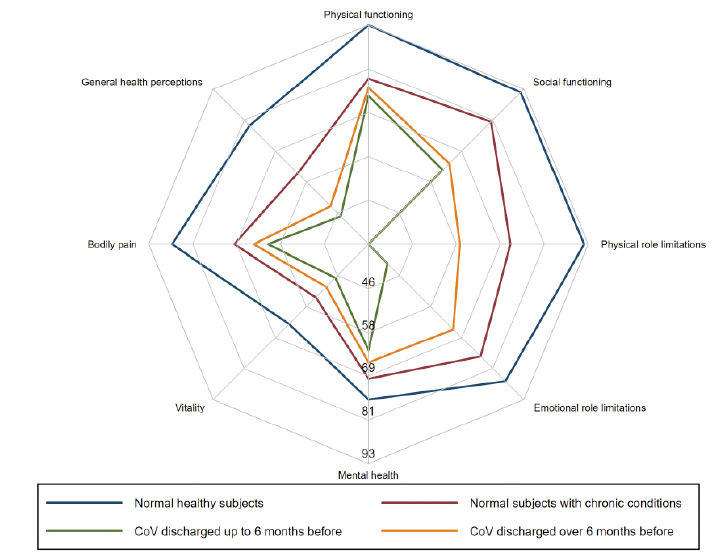 Click to show fullsize
Click to show fullsize