
From the 1Department of Rehabilitation Medicine, Erasmus MC, University Medical Center Rotterdam, 2Rijndam Rehabilitation and 3Department of Neurology, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands
Objective: To examine the association of fatigue with long-term participation in aneurysmal subarachnoid haemorrhage survivors.
Design: Cohort study, 4 years post-onset.
Subjects: A total of 59 patients with aneurysmal subarachnoid haemorrhage.
Methods: Participation performance was assessed with the Sickness Impact Profile-68, participation autonomy and problem experience with the Impact on Participation and Autonomy questionnaire, and community integration with the Community Integration Questionnaire. Fatigue was assessed with the Fatigue Severity Scale and depression with the Center for Epidemiologic Studies-Depression scale. Multivariable linear regression analyses were performed.
Results: Fifty-nine survivors (mean age 53.0 years, standard deviation (SD) 10.8 years) were included, of which 59.3% was fatigued. Fatigued patients had significantly worse participation scores than non-fatigued patients regarding performance (p < 0.001), autonomy indoors (p = 0.001), autonomy outdoors (p = 0.002) and problem experience (p = 0.001), but not regarding community integration. More severe fatigue was related to worse participation in terms of performance (B = 2.79, p < 0.001) and problem experience (B = 0.08, p = 0.003), adjusted for depression and inpatient rehabilitation.
Conclusion: Four years after onset, many survivors of aneurysmal subarachnoid haemorrhage have persistent fatigue, which is independently associated with reduced participation in activities of daily living. Therefore, future studies should investigate whether rehabilitation programs that focus on fatigue are effective in improving long-term participation outcome after aneurysmal subarachnoid haemorrhage.
Key words: subarachnoid haemorrhage; fatigue; social participation; community integration; depression; stroke; rehabilitation.
Accepted Jan 28, 2021; Epub ahead of print Feb 19, 2021
J Rehabil Med 2021; 53: jrm00173
Correspondence address: Elisabeth A. de Vries, Erasmus MC, University Medical Center Rotterdam, Department of Rehabilitation Medicine, PO Box 2040, 3000 CA Rotterdam, The Netherlands. E-mail address: ldvries@rijndam.nl
Doi: 10.2340/16501977-2800
A subarachnoid haemorrhage (SAH) is a subtype of stroke. In most cases subarachnoid haemorrhage is caused by rupture of an aneurysm, termed aneurysmal subarachnoid haemorrhage. Fatigue is one of the most common symptoms after aneurysmal subarachnoid haemorrhage. Fatigue may reduce participation in activities of daily living. If fatigue and participation are related, focusing on fatigue during rehabilitation might improve participation in activities of daily living after aneurysmal subarachnoid haemorrhage. Therefore, this study examined whether fatigue is associated with participation 4 years after aneurysmal subarachnoid haemorrhage. The results showed that fatigued patients participated less in activities of daily living, were less autonomous regarding their participation, and had more problems with their level of participation than non- fatigued patients. In addition, more severe fatigue was related to worse participation in activities of daily living and more problems with the level of participation. This indicates that treating fatigue during rehabilitation might improve participation in the long-term after aneurysmal subarachnoid haemorrhage.
Aneurysmal subarachnoid haemorrhage (a-SAH), caused by rupture of an intracranial aneurysm, accounts for approximately 5% of all strokes (1). The survival rate of patients with a-SAH has increased by 17% over the past 30 years, to approximately 65% (2). SAH survivors are relatively young (mean age 55 years) (1) compared with patients with other types of stroke (mean age 69 years) (3). Although the majority of survivors regain functional independence (4), many experience long-term impairments in cognitive and daily functioning (5). The consequences of SAH may interfere with quality of life (6) and participation in society (7), especially because patients with a-SAH are generally in the middle of their working lives and may have a family to take care of. Therefore, during recovery and rehabilitation after a-SAH, the focus should be not only on functional outcomes, but also on reintegration into normal living, including participation in work and social activities (8).
Participation is a multifaceted concept that can be defined as “involvement in a life situation” (9). It encompasses both a performance aspect (e.g. frequency of activities), and an individual perspective or experience aspect (e.g. satisfaction with level of participation) (10). Previous studies have shown that patients with a-SAH perceive a variety of problems in participation in the long-term; they were dissatisfied with their level of participation (7) and perceived participation restrictions regarding employment (11–14), self-organization and mobility (12) and reintegration into normal life (14) and social and leisure activities (15).
The underlying mechanism that accounts for problems in participation after a-SAH is not well understood. Age, comorbidity, and unmet needs were found to be inversely associated with community integration after a-SAH (16), mood disturbances with participation restrictions (11), and anxiety and cognitive complaints with participation restrictions and satisfaction with participation (7). In addition, fatigue was associated with reduced self-organization and socializing after a-SAH (12, 15), and depression, physical disability, and a-SAH severity were inversely associated with return to work and normal life activities (14). Fatigue is of particular interest, because, with a prevalence of up to 90%, it is one of the most commonly reported sequelae after a-SAH (17, 18). However, fatigue after a-SAH may interact with depression; patients with depressive symptoms experience more severe fatigue (19) and both were found to be associated with participation. Interestingly, independent of depression, fatigue was found to contribute to problems in resumption of leisure and social activities 4 years after a-SAH (15). These results suggest that fatigue plays an essential role in participation outcome in the long-term after a-SAH. However, participation not only includes performance in leisure and social activities, but also the perceived level of participation and autonomy and community integration, in which the role of fatigue has not yet been investigated. In addition, the assessment of fatigue in previous studies was not based on validated questionnaires, but on 1 or 2 questions related to fatigue (12, 15). Therefore, the aim of this study was to explore the role of fatigue in participation outcomes 4 years post-a-SAH. It was hypothesized that fatigued patients with a-SAH have worse participation than non-fatigued patients and that fatigue severity is independently associated with participation outcomes.
Participants and procedures
Consecutive patients diagnosed with a-SAH, who were hospitalized between 2006 and 2009 at the neurology or neurosurgery departments of Erasmus MC and fulfilled the inclusion and exclusion criteria, were asked to participate in a prospective cohort study with measurements in the first year and after 4 years’ follow-up (16, 20). In the current study, a cross-sectional secondary analysis of the 4-year follow-up data was conducted. Inclusion criteria were survival of SAH and aged at least 18 years. Exclusion criteria were serious (neurological) comorbidity resulting in a life expectancy less than one year and insufficient mastery of the Dutch language. A-SAH was diagnosed by computed tomography (CT) and, if negative, by lumbar puncture and CT angiography and/or digital subtraction angiography to detect the aneurysm. Before inclusion all patients signed an informed consent form. The medical ethics committee of Erasmus MC approved the study (MEC 2004–255).
Data collection
The staff of the neurology and neurosurgery departments of Erasmus MC collected baseline sociodemographic data and clinical characteristics, including SAH severity (according to the World Federation of Neurosurgical Societies classification), location of the aneurysm (anterior or posterior circulation), treatment procedure (surgical clipping or endovascular coiling), and discharge to inpatient rehabilitation (rehabilitation centre/nursing home) or home. Four years post-a-SAH onset, patients were visited at home by a trained research psychologist to collect data on fatigue, multiple participation outcomes, and depression, with validated self-report questionnaires (16, 20).
Measurement instruments
Severity of fatigue was assessed with the Fatigue Severity Scale (FSS). Patients rate their agreement with 9 statements about fatigue (e.g. “Fatigue interferes with my physical functioning”) on a 7-point Likert-scale, ranging from 1 (strongly disagree) to 7 (strongly agree). A mean score (range 1–7) was calculated, where higher scores indicate more severe fatigue. If the mean score is 4 or higher, patients are considered fatigued (21).
Three participation instruments were used. Participation in terms of functional performance in activities of daily living was assessed with the Sickness Impact Profile-68 (SIP-68) (22). It contains 68 items, divided over 6 subscales, which are categorized in a physical domain (somatic autonomy, mobility control, and mobility range) and a psychosocial domain (psychological autonomy and communication, social behaviour, emotional stability). Examples of items in the physical domain are “I walk more slowly” and “I do not maintain balance” and examples of items in the psychosocial domain are “I am doing fewer community activities” and “I do not finish things I start”. Patients mark those items that apply to their current health status, where a marked item indicates 1 point. All marked items are summed and this number reflects the total score (range 0–68). The physical domain consists of 39 items (score range 0–39) and the psychosocial domain consists of 29 items (score range 0–29). Higher scores indicate more health-related restrictions in daily functioning (22).
Perceived participation and autonomy were assessed with the Impact on Participation and Autonomy (IPA) questionnaire. The IPA consists of 32 questions divided over 5 domains; autonomy indoors, family role, autonomy outdoors, social relations, and work and education. The questions are focused on the possibility to participate in daily life when and the way the patient wants to (e.g. “My chances of visiting relatives and friends when I want to are…”; “My chances of spending leisure time the way I want to are…”. The items are rated on a 5-point scale, ranging from 0 (very good) to 4 (very poor). Domain scores are calculated by averaging the items per domain (score range 0–4). Higher domain scores reflect more perceived restrictions in participation and autonomy. In addition, patients indicate whether they experience their level of participation as problematic by scoring 9 items (e.g. “With regard to your leisure time, to what extent does your health or disability cause problems?”) on a 3-point scale, ranging from 0 (no problems) to 2 (severe problems). A mean problem score (IPA problem experience, range 0–2) was calculated, where a higher score indicates more perceived problems with the level of participation (23).
Participation in terms of community integration was measured with the Community Integration Questionnaire (CIQ) (24). The revisited CIQ was used, consisting of 13 items divided over 3 subscales; home competency, social integration, and productive activity (25). The home competency scale consists of 5 items about who usually does household-related activities (e.g. “Who usually prepares meals in your household?”). Patients rate the items on a 3-point scale, ranging from 0 (someone else) to 2 (yourself alone). The social integration scale consists of 5 items about participating in activities outside the own home (e.g. “How often do you travel outside the home?”). Items are scored on a 3-point scale, ranging from 0 to 2, where 0 indicates either a low frequency of participating in these activities or performing activities alone and 2 indicates either a higher frequency of participating in these activities or performing activities with family and/or friends. Sum scores are calculated for both the home competency scale and the social integration scale separately, resulting in subscale scores ranging from 0 to 10. The productive activity scale consists of 3 questions about current work situation, current school or training programme situation, and about the frequency of engaging in volunteer activities. A combined score ranging from 0 (not working, not going to school, no volunteer activities) to 5 (working full-time and attending school) is given. A total sum score (range 0–25) is calculated by adding the scores of the 3 subscales. Higher scores on all 3 subscales and a higher total score indicate a higher level of community integration (25).
Depressive symptoms were assessed with the Center for Epidemiologic Studies Depression scale (CES-D). Patients rate 20 items about their perceived mood during the past week (e.g. “ During the past week… I felt sad”) on a 4-point scale ranging from 0 (rarely or none of the time, less than one day) to 3 (most or all of the time, 5–7 days). The total sum score ranges between 0 and 60. Higher scores reflect more depressive symptoms, where a score of 16 or higher is indicative for the presence of depression (26). An overview of the questionnaires is shown in Table SI.
Statistical analyses
Statistical analyses were performed using IBM SPSS Statistics version 23 (SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to present the characteristics of the total study population and the subgroups of fatigued and non-fatigued patients. Normality of the data was checked. Independent t-tests and χ2 tests were carried out to check for differences in patient characteristics and participation scores between fatigued and non-fatigued patients. Univariable regression analyses were performed to examine relationships of fatigue and potential confounders (sociodemographic and clinical characteristics, discharge to inpatient rehabilitation, and depression) with the participation outcomes (SIP total score, IPA problem experience score and CIQ total score). Subsequently, multivariable regression analyses were conducted with forward selection of the variables that were significant (p < 0.05) in univariable regression analyses, for each of the 3 participation outcomes separately (entry p-value 0.05, removal p-value 0.10). Variables were checked for multicollinearity by examining the correlation between the variables, the variance inflation factor (VIF) and tolerance (1/VIF) and by examining whether the variance proportions were distributed across different dimensions (eigenvalues) for each predictor. Based on these 3 criteria no multicollinearity was found between the variables in the regression analyses. A significance level of p < 0.05 was used and a Bonferroni correction was applied to correct for multiplicity.
Study population
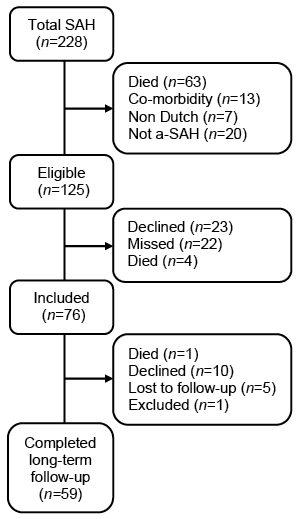
A total of 125 out of 228 patients with a-SAH were eligible to participate in the study. Of these, 76 patients agreed to participate, of whom 59 patients participated in the 4 years follow-up measurement (Fig. 1). The measurement were conducted at a mean of 3.9 years (SD 0.8 years) post-SAH onset. Characteristics of the total group and the fatigued and non-fatigued subgroups are shown in Table I. Mean age at SAH-onset was 53.0 years (SD 10.8 years) and 35.6% were men. The majority of patients were fatigued (59.3%), with a mean overall fatigue score of 4.2 (SD 1.7). A proportion of 28.8% was discharged to inpatient rehabilitation (rehabilitation centre or nursing home) and 27.1% had symptoms of depression. In the fatigued group, both the depression score and the proportion of depression were significantly higher than in the non-fatigued group. Sociodemographic and clinical characteristics did not differ significantly between the groups (Table I).
Fig. 1. Flow diagram. SAH: subarachnoid haemorrhage; a-SAH: aneurysmal subarachnoid haemorrhage.
Table I. Patient characteristics and outcome 4 years post-a-SAH onset
Participation outcomes
Four years post-a-SAH onset, patients reported a mean of 9.8 (SD 10.5) restrictions in functional performance, as measured with the SIP-68, mainly in the psychosocial domain (mean 6.7; SD 7.0) (Table II). IPA subdomain scores varied between 0.6 (SD 0.7) and 1.2 (SD 0.9), indicating some perceived restrictions in participation and autonomy. Patients did not experience many problems with their level of participation, given the mean IPA problem experience score of 0.4 (SD 0.4) over the 5 domains. The mean community integration score was 15.0 (SD 4.3), indicating a reduced level of community integration, in particular in the productive activity domain (mean 1.8; SD 1.8).
Differences in participation between fatigued and non-fatigued patients
All participation outcomes were significantly (p < 0.05) worse in the fatigued group than in the non-fatigued group, except for the IPA Work and Education and CIQ Home Competency and Social Integration subscales (Table II). After Bonferroni correction, the difference between the groups remained significant (p < 0.004) for the SIP-68 total score, for both the Physical domain and Psychosocial domain, the IPA Autonomy Indoors domain and IPA Autonomy Outdoors domain, and the overall Problem Experience score.
Table II. Participation outcomes for the total group, fatigued group and non-fatigued group
Associations of fatigue severity with participation outcomes
Fatigue, depression, and discharge to inpatient rehabilitation were significantly associated with all 3 participation outcomes in univariable regression analyses (Table III). In addition, age was associated with community integration. The Spearman’s rank correlation between fatigue (FSS) and depression (CES-D) was 0.473 (p < 0.001), between fatigue and discharge destination 0.125 (p = 0.344) and between depression and discharge destination 0.088 (p=0.507), indicating no multicollinearity between the predictors. Adjusting for depression and inpatient rehabilitation, fatigue severity was independently associated with participation, as assessed with the SIP-68 total and overall IPA problem experience score. For both outcomes, more severe fatigue was independently related to more restrictions in functional performance and more perceived problems in participation (Tables III and IV). Regarding community integration, fatigue did not contribute significantly to the model containing age and depression. Older age and higher depression score were independently related to worse community integration (Tables III and IV).
Table III. Variables associated with participation in univariable and multivariable regression analyses
Table IV. Model selection and performance
Four years post-a-SAH onset, fatigued patients had more health-related restrictions in functional performance, they experienced more restrictions in participation and autonomy in the autonomy indoors and outdoors domains, and they perceived more problems with their level of participation than non-fatigued patients. Moreover, fatigue severity was independently related to worse long-term participation in terms of functional performance and perceived problems with the level of participation, adjusted for depression and discharge to inpatient rehabilitation.
The multifaceted nature of participation is reflected in its definition, namely “involvement in a life situation” (9). Due to this broad definition, a variety of questionnaires is used to assess participation outcome after stroke (27). This makes the results of studies difficult to compare, but allows the extensive examination of participation (28). In the current study different questionnaires were used to assess participation in terms of functional performance (SIP-68), perceived participation and autonomy (IPA) and community integration (CIQ) after a-SAH, thereby covering both the performance and experience aspects of participation (10).
Regarding participation in terms of functional performance in activities of daily living, patients with a-SAH in the chronic phase had a higher level of participation than patients within the first year after other types of stroke (29, 30). Fatigued patients reported significantly more restrictions in functional performance than non-fatigued patients, primarily in the psychosocial domain. The lower overall SIP-68 score in patients with a-SAH may be attributed to the longer time post-onset and the often more favourable (functional) outcome of patients with a-SAH than patients with other types of stroke; for example, regarding hemiparesis or aphasia (1, 4, 5, 8). In the current study, the proportion of patients with depression was higher in the fatigued group than in the non-fatigued group. Patients with depressive symptoms tend to score lower on self-report questionnaires as the SIP (31), which may partly explain the lower scores in the fatigued group. However, interestingly, fatigue severity was found to be related to overall functional performance, independent of depression and discharge to inpatient rehabilitation. These results add to findings from a previous study, which show that fatigue is associated with return to social and leisure activities after a-SAH, independent of depression (15). The independent effect of fatigue on functional performance is interesting, since fatigue is one of the most commonly reported sequelae after a-SAH (18). Even 4 years post-onset, patients with a-SAH, in particular those who are fatigued, still experience a substantial number of health-related restrictions, primarily in the psychosocial domain, despite the fact that almost one-third had received inpatient rehabilitation. The current study shows the potential of improving participation, in terms of functional performance, especially in activities related to cognitive functioning, mood and socializing, by focusing more on fatigue in rehabilitation after a-SAH. This could be accomplished by, for example, incorporating psycho-education sessions in a rehabilitation programme, where the patient can be guided by an occupational therapist in coping with fatigue and planning activities of daily living. In addition, motivating patients to be physically active seems an important aspect in rehabilitation after a-SAH, because more severe fatigue was found to be related to decreased physical fitness in patients with a-SAH (32).
The outcomes of the IPA reflect the perceived autonomy, the experienced restrictions in participation and problems with the level of participation (23). Overall, the scores on the IPA subdomains were similar to scores found in a previous study, in patients 5 years post-stroke (63% very mild stroke) (33), indicating that patients with a-SAH perceive the same level of restrictions and autonomy in participation and equal problems with the level of participation as patients after stroke. Fatigued patients with a-SAH experienced more restrictions in participation and autonomy than non-fatigued patients, especially in the autonomy indoor and outdoor domains. Apparently, fatigue is primarily associated with restrictions in participation and autonomy regarding self-care and leisure activities and less with activities related to social relations, family role and work and education. Regarding problems with the level of participation, it was found that fatigued patients experienced more problems than non-fatigued patients. In addition, fatigue severity was independently related to perceived problems with the level of participation, adjusted for depression and inpatient rehabilitation as discharge destination. Hence, in addition to the independent role of fatigue in functional performance, fatigue severity is also independently related to the experience aspect of participation in patients with a-SAH. This is of added value for rehabilitation purposes, since it stresses the need to look beyond the (functional) performance aspect of participation, by taking into account the experience aspect (10), especially in fatigued patients with a-SAH.
Finally, in the current study the role of fatigue in community integration in 3 domains was analysed: home competency, social integration, and productive activity (25). The level of community integration, in terms of frequency and support needs, of patients 4 years post-a-SAH is comparable to community integration of patients only 1 year after traumatic brain injury (25), but slightly higher than community integration of brain injury patients, including patients with stroke (34). No differences were found between fatigued and non-fatigued patients with a-SAH on the total scale and the 3 domains of community integration. In addition, fatigue severity was not associated with community integration. This seems to contrast with previous findings that fatigue after a-SAH is inversely related to independence in self-organization and frequency of socializing (12). However, fatigue in this study was not assessed with a validated questionnaire, but with only 1 question about fatigue (12). By assessing fatigue with 1 question instead of a questionnaire, a different aspect of fatigue might be assessed, which may be differently related to participation outcome (35).
Study strengths and limitations
A strength of the current study is that fatigue was assessed with a validated questionnaire and multiple participation outcomes were assessed. This allowed the role of fatigue in various domains of participation to be studied. Another strength is that in the current study depression was also assessed, since depression is found to be related to participation and fatigue after a-SAH (14, 19), and discharge to inpatient rehabilitation treatment was taken into account. Consequently, it was possible to examine the independent role of fatigue in participation outcomes.
The current study has some limitations. Due to the relatively small sample size, a limited number of variables could be included in the regression analyses. In addition, given the cross-sectional analysis of long-term outcome, this study could not assess causal relationships. A possible longitudinal relationship between fatigue and participation should be further investigated in long-term follow-up studies, using multiple instruments to assess fatigue and taking into account depression.
To summarize, 4 years after a-SAH fatigue severity was independently related to multiple aspects of participation, adjusted for depression and discharge to inpatient rehabilitation. This outcome may encourage clinicians in triaging patients with a-SAH who experience fatigue for rehabilitation services, where the focus could be on coping with fatigue and guidance in resumption of activities, to improve participation performance and experience.
The authors have no conflict of interest to declare.


 Click to show fullsize
Click to show fullsize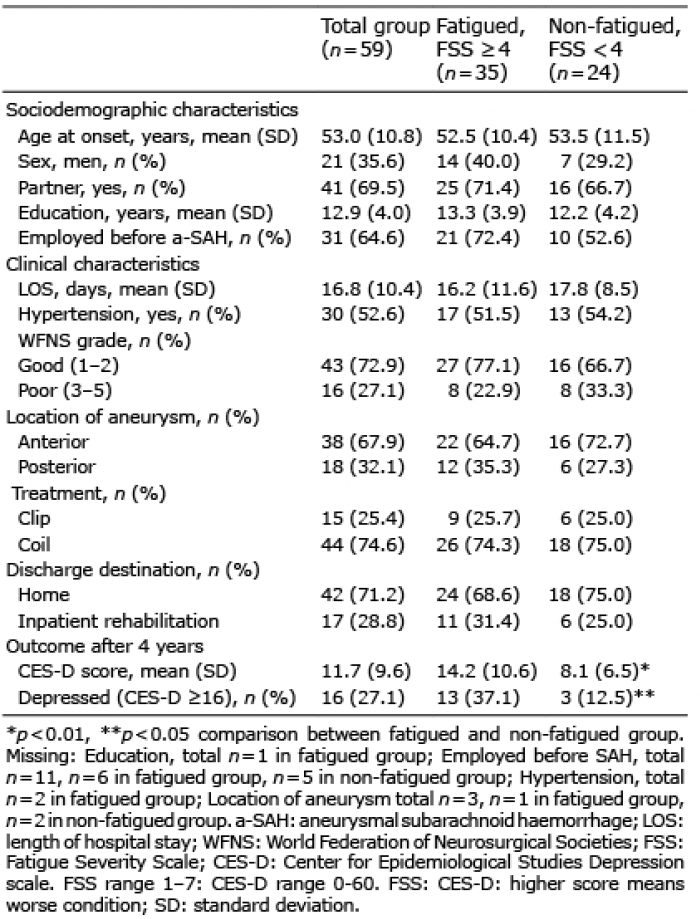 Click to show fullsize
Click to show fullsize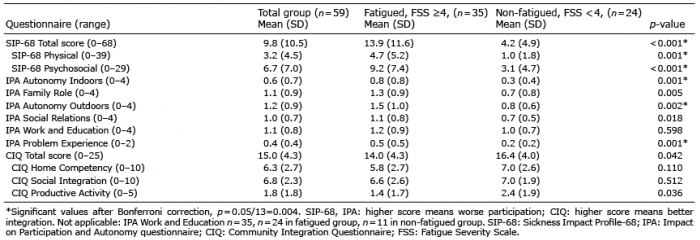 Click to show fullsize
Click to show fullsize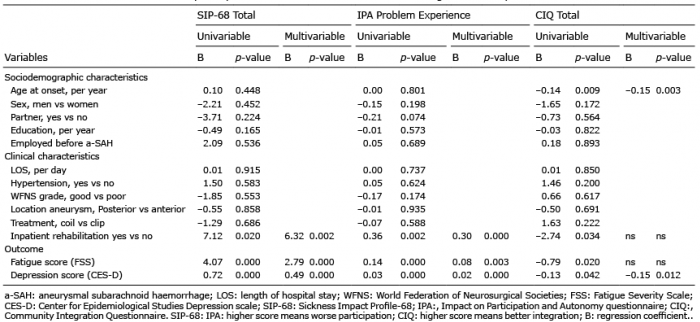 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize