
From the 1Department of Rehabilitation Medicine, Hannover Medical School, Germany, 2Department of Physical and Rehabilitation Medicine, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java/Hasan Sadikin Hospital, Bandung, West Java, Indonesia, 3Department of Rehabilitation Medicine, M. Djamil Hospital, Padang, West Sumatra, 4Faculty of Medicine, Universitas Andalas, Padang, West Sumatra, 5Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Hasanuddin University, Makassar, South Sulawesi, and 6Faculty of Medicine, Maranatha Christian University, Bandung, West Java, Indonesia
Objective: Describing rehabilitation services in a standardized way is a challenge. The International Classification of Service Organizations in Rehabilitation (ICSO-R) 2.0 was published for this purpose. The ICSO-R was criticized for being tested mainly in high-income countries, and because the testing in lower-income countries did not include community-based rehabilitation services. Therefore, this study was performed to describe community-based rehabilitation services by using ICSO-R 2.0.
Methods: The ICSO-R 2.0 was used to describe 8 community-based rehabilitation services located in 3 cities in 3 different provinces in Indonesia: 6 community-based rehabilitation services in Bandung, West Java; 1 in Tanah Datar, West Sumatra; and 1 in Gowa, South Sulawesi.
Results: All the community-based rehabilitation services were owned by the government, as a public body, and in the context of the community. The 6 community-based rehabilitation services in Bandung, West Java, are under the government city of Bandung, while the other 2, from Tanah Datar and Gowa, are integrated within primary healthcare centres. Social welfare supports all 6 community-based rehabilitation services in Bandung. The other 2 community- based rehabilitation services are supported by their respective primary healthcare centres.
Conclusion: The ICSO-R 2.0 is a feasible tool to describe rehabilitation services, including community- based rehabilitation.
Key words: International Classification of Service Organizations in Rehabilitation; ICSO-R; classification; community-based rehabilitation; rehabilitation; health service organization.
Accepted Jan 28, 2021; Epub ahead of print Feb 24, 2021
J Rehabil Med 2021; 53: jrm00166
Correspondence address: Boya Nugraha, Department of Rehabilitation Medicine. Hannover Medical School, Carl-Neuberg-Straße 1, D-30625 Hannover, Germany. E-mail: boya.nugraha@gmail.com
Doi: 10.2340/16501977-2804
The International Classification of Service Organizations in Rehabilitation (ICSO-R) 2.0 was published as a framework to support describing rehabilitation service organizations. The process of development of the ICSO-R did not include Community-Based Rehabilitation Services. Therefore, to rectify this, ICSO-R 2.0 was used for this study. Eight community-based rehabilitation services were surveyed, located in 3 cities in Indonesia; namely Bandung, Tanah Datar, and Gowa. This study found that ICSO-R 2.0 can be used to describe rehabilitation services not only in hospitals, but also in the community.
Strengthening rehabilitation in health systems has become a worldwide agenda. It was accelerated after the launched of the United Nations Convention on the Rights of People with Disabilities (UN-CRPD; (1)), particularly article 26, which mentions habilitation and rehabilitation. Later, the adoption of the Global Disability Action Plan of WHO in 2014 (2), Rehabilitation 2030: A Call for Action (3), and Recommendations for Rehabilitation in the Health System (4) clearly stated the need to strengthen rehabilitation services. In addition, rehabilitation services are also mentioned in the World Report on Disability (1–3, 5).
Rehabilitation services have 2 definitions. The first definition is “a set of measures that assist individuals who experience, or are likely to experience, disability to achieve and maintain optimal functioning in interaction with their environments” (5). This definition describes rehabilitation programmes for health conditions (rehabilitation at the micro-level). Another defines rehabilitation services based on how the rehabilitation service is organized (6, 7). The latter definition is related to rehabilitation at the meso-level of the health system (8). Responding to the latter definition, which was not clearly defined, the International Society of Physical and Rehabilitation Medicine – World Health Organization Liaison Committee (ISPRM-WHO LC)working group published its first proposal, which is called the International Classification of Service Organizations in Rehabilitation (ICSO-R) (6). Following testing and review by international experts, the second version was published recently (ICSO-R 2.0) (7). ICSO-R 2.0 consists of 2 dimensions; service providers and service delivery. These dimensions consist of 9 and 14 categories, respectively.
According to the Rehabilitation Recommendations of WHO (4), rehabilitation services should be integrated into the health system, including availability both in hospitals and the community. In Indonesia, rehabilitation services should be integrated into tertiary and secondary hospitals (9). In addition, rehabilitation services are also available at rehabilitation medicine practices, organized by physical and rehabilitation medicine (PRM) physicians, physiotherapists (PTs), occupational therapists (OTs), and speech and language therapists (SLT). In Indonesia, at the community level, rehabilitation services are delivered at community-based rehabilitation (CBR) services, particularly in areas where rehabilitation services at the hospital are unavailable or lacking.
CBR is one type of rehabilitation service that is mostly provided in the community (10). It was originally established to give access to people with disability where there was no access to rehabilitation services in hospital. Many studies have reported on rehabilitation programmes for different health conditions, provided at CBRs, such as schizophrenia (11), stroke (12), spinal cord injury (13), and post knee arthroplasty patients (14).
Structurally, CBRs can be categorized as one type of rehabilitation service organization. However, to the best of our knowledge, there has been no study describing CBRs as an organization delivering services, or describing how CBRs are organized systematically. Before publishing the ICSO-R 2.0, the testing of the first version of the ICSO-R was performed mostly at tertiary or academic level hospitals. Therefore, this study aimed to review the feasibility of using the ICSO-R 2.0 to describe CBR services.
The ICSO-R 2.0 was used as a framework to collect data on CBR services. The ICSO-R 2.0 consists of 2 dimensions: provider and service delivery (7). In the dimension of provider, there are 9 categories: context; ownership; location of provider; governance/leadership; quality assurance and management; human resources; technical resources; funding of provider; and other categories of provider. The dimension of service delivery consists of health strategies; service goals; target groups; modes of referral; location of service delivery; facility; setting; integration of care; patient-centeredness; aspect of time and intensity; rehabilitation team; reporting and documentation; funding of service delivery; and other categories of service delivery. Some of categories of both provider and service delivery have subcategories. All dimensions, categories, and subcategories have definitions, inclusions, and exclusions.
CBR services were surveyed using the ICSO-R 2.0 in 3 cities of Indonesia; namely Bandung, West Java province; Padang, West Sumatra Province; and Makassar, South Sulawesi. The number of CBR services surveyed was 6, 1, and 1, respectively. Convenience sampling methods were used to select these 8 CBR services.
The data were collected by interviewing the CBR cadres (voluntary workers in the village where the CBR services are located) of every CBR service. The interviews were completed by PRM physicians, and the residents in the PRM programme of the respective university hospitals. The coordinators in each location received training on how to use the ICSO-R 2.0 by one of the developer/author (BN).
The study was conducted at 8 CBR services in 3 cities; namely Tanah Datar, West Sumatra; Bandung, West Java; and Gowa, South Sulawesi, Indonesia (Fig. 1). Batipuh II is one district in the city of Tanah Datar, West Sumatra. The location of the CBR service is in a rural area of Tanah Datar. Tanah Datar is located approximately 86 km and 1,200 km from Padang, the capital of West Sumatra Province, and Jakarta, the capital of Indonesia, respectively. Tanah Datar has population of 356,085 (15). Bandung is the capital of West Java province, and is located approximately 150 km from Jakarta, the capital of Indonesia. The population of Bandung is approximately 2.5 million (16). The location of the other 6 CBR services is urban areas of Bandung. Gowa is a city located approximately 10 km from Makassar, the capital of South Sulawesi province, and 1,600 km from Jakarta. The population of Gowa is 721,623, according to data from 2015 (17). The location of CBR services was in urban areas of Gowa.
Fig. 1. Map of Indonesia and location of community-based rehabilitation (CBR) services surveyed: Tanah Datar, West Sumatra; Bandung, West Java; and Gowa, and South Sulawesi.
Rehabilitation services in Indonesia are available both in hospitals and in the community. In the community, CBR plays an important role in providing rehabilitation services, as it is closer to the living situation of patients with rehabilitation needs. The CBR services are described below, based on the ICSO-R 2.0 framework.
Community-based rehabilitation services at the provider level
In Bandung, West Java, 6 CBR services were described at different governmental levels: 2 at the district level, and 4 at the sub-district level. In Tanah Datar, West Sumatra, and in Gowa, South Sulawesi, the CBR services were at the district and city level, respectively. The description of each CBR service at the provider level is given in Table I.
Table I. CBR provider profile in different cities in Indonesia.
Context (1.1), Ownership (1.2), and Location (1.3). All CBR services that were surveyed are in the context (1.1) of the community, and are owned (1.2) by the government (public body). Interestingly, in Bandung, West Java, the CBR are under the Bandung city government, meanwhile in Tanah Datar and Gowa, the CBR are under Health Services, specifically under Primary Healthcare Services (PHC: Pusat Kesehatan Masyarakat/Puskesmas). Only the CBR service in Tanah Datar is located (1.3) in a rural area. The others are in city/urban areas.
Mission (1.41), Vision (1.4.2), and Involvement in governance (1.4.3).The missions and visions of all CBR services in Bandung are the same as they are under one organizational structure, which is the city government of Bandung. The CBRs at the sub-district and district level are subordinated to the CBRs at the city level. The mission and vision in Tanah Datar, West Sumatra and Gowa are slightly different, but they have similarities; utilizing society, including family, to empower and improve the health of society and persons with disability (PWD) in their area. In Gowa, the vision is related to upholding the rights of PWD in the community, one of which is healthcare.
In Bandung, the heads of the CBRs at the district and sub-district levels are the spouses of the respective districts and sub-districts. In difficult cases, the head of the district will become involved in solving the problem. It is also possible to arrange a meeting with the section head of Social Welfare Services of the District.
As the CBR services in Tanah Datar, West Sumatra, and Gowa, South Sulawesi, are under PHC, the head of the CBRs at these 2 places are the medical leaders of the PHCs. However, in all CBR services, users and user groups are involved in the governance of the CBR.
Quality assurance and management (1.5). CBR services in Bandung undergo both an internal and external audit. The internal audit is performed by the cadres and the head of the CBR cadres at least once a year. The external audit is performed by the head of the district and their team. Both of these audit programmes lack certification. In Tanah Datar, an internal audit (without certification) is performed every 6 months, involving the programme manager, head of the PHC, and the district midwife. The external audit for the CBR at Tanah Datar is performed in conjunction with the audit of the PHC. It is performed by an accreditation team appointed by the Ministry of Health. In Gowa, the CBR is audited only by an internal auditor (without certification).
Human resources (1.6). CBR cadres are the main overseers of every CBR service in Indonesia. CBR cadres are voluntary workers in the village where CBR services are located. They do not have formal education to be CBR cadres. However, they collaborate with health professionals, particularly with general practitioners (GPs) at PHCs. PRMs and PTs are also involved in providing advice and education around basic rehabilitation (activities of daily living; ADL) to CBR cadres.
Technical resources (1.7). All CBR services provide diagnostic and therapeutic services in collaboration with health professionals at PHCs. Almost all CBR services, except at Tanah Datar, provide assistive devices, such as wheelchairs, crutches, and audiometry. In Gowa, hand-made simple assistive devices are also available. Communication mainly is facilitated using cellphones and Whatsapp®. These communication tools are also used not only among the CBR teams, but also with patients and families. Reporting and documentation is done electronically, and/or is paper-based.
Source of money (1.8.1) and Criteria for spending (1.8.2). All CBR services are funded by the government. All CBR services in Bandung and Gowa are funded by Social Services. CBR services in Tanah Datar are funded by the budget fund, with health operational support from the PHCs of Batipuh II, Tanah Datar, West Sumatra. In addition, CBR services in Bandung also receive additional charity funding from public foundations (e.g. Siti Hajar Amali Foundation) and societies. In Bandung, the budget is funded specifically after each CBR service makes a proposal to the government. The budget is mainly used for technical resources, consumables, and goods. In some cases (e.g. special events, such as International Disability Day), other institutions, such as banks, will also provide support. All cadres in all CBR services in Indonesia work voluntarily (without any payment).
Community-based rehabilitation services at the service delivery level
The descriptions of each CBR service are provided in Table II.
Table II. Community-Based Rehabilitation (CBR) service delivery profile in different cities in Indonesia
Health strategies (2.1). Interestingly, all 8 CBR services that were assessed implement multi-health strategies, namely promotion, prevention, and maintenance.
Service goals (2.2). All CBRs have goals around recovery, improvement of health status, and optimizing functioning, particularly improvement of self-care.
Target groups (2.3), Health condition groups (2.3.1), Functioning groups (2.3.2), and Other target groups (2.3.3). Most of the patients have neurological problems (stroke, spinal cord injury), limb amputations, diabetes, cerebral palsy, polio, Down syndrome, mental health problems, and dementia. Functioning issues include gait, mobility, and vocational problems. CBR services in Bandung and Gowa provide services to both adults and children, as well as elderly people and workers. In Tanah Datar, services are delivered only to children. Two CBR services in Bandung (Batu Nunggal and Bandung Wetan) deliver services to ex-athletes who currently work as coaches.
Modes of referral (2.4). Most patients come to CBR services by self-referral. However, cadres and physiotherapists can recommend patients to the PHC and hospitals. Other health professionals, such as GPs and PRM physicians, can also refer patients to the PHC and hospitals. In the case of CBRs at Tanah Datar, midwives can also refer patients to the primary care centre.
Location of service delivery (2.5), Location characteristics (2.5.1), and Catchment area (2.5.2). The assessed CBRs in Bandung and Gowa are located in the city/urban areas. The CBR of Batipuh II, Tanah Datar, is located in a rural area. The catchment of the CBR is based on the location of the CBR services. It can be at the city level, district level, or sub-district level. All CBR services are delivered in the community and/or at homes of users.
Facility (2.6). All CBR services have their own building. However, the buildings are not used to deliver services; they are used for administration-related issues. The buildings in Tanah Datar and Gowa belong to the PHCs. In all CBRs in Bandung, an ambulance car can be provided through collaboration with the PHC at the district level.
Setting (2.7), Levels of care (2.7.1), Mode of service delivery (2.7.2), and Phase of healthcare (2.7.3). A CBR is part of a primary care service that is delivered either through CBR services, the community, PHCs, or home users. In some cases, CBR services in Bandung can also refer patients to a non-profit foundation (e.g. Yayasan Penyandang Anak Cacat (YPAC; Foundation for Children with Disabilities)). Most patients in CBRs are in need of post-acute and long-term rehabilitation care services.
The cadres of the CBR at Tanah Datar collect data from society (including early detection data), and teach families how to carry out basic rehabilitation related to ADL for children with disabilities, based on a guidance book provided by the government.
Integration of care (2.8). In Bandung and Gowa, CBR services are part of a continuum of care in collaboration with health professionals, including general practitioners at PHC centres. CBR cadres also act as counsellors, accompanying patients to prosthetics and orthotics technician, physiotherapist, and primary care appointments, and support when other higher referral systems are needed. In Bandung, children with light to moderate disabilities can be referred to the YPAC by cadres.
In Tanah Datar, cadres evaluate patients once a month at the Integrated Service Post (Pos Pelayanan Terpadu (Posyandu)), and follow-up evaluations are usually performed every 6 months using a standardized evaluation form. Children who need further rehabilitation will be referred by midwives to the PHC and evaluated by the general practitioner, before being referred to a secondary or tertiary hospital.
Patient-centredness (2.9). In all CBR services in this study, patients, family and caregivers are involved in the rehabilitation plan and shared decision-making process. Education and empowerment are also given to patients and the family, with involvement of patients as prosumers.
Aspect of time and intensity (2.10). In Bandung and Gowa, there is no specific time-point to access services, however a visit to the home of the user is always carried out at least once a month, including empowerment of the family. In the case of severe disability, the visits could be more frequent, and the entire CBR cadre team can come at any time upon request.
In Tanah Datar, no rehabilitation treatment is available to children with disabilities, however as mentioned above, the services include early detection, collecting data, and teaching families. These are carried out once a month and evaluated every 6 months.
Rehabilitation team (2.11), Professions, competencies (2.11.1), Interaction approaches (2.11.2). In Bandung, CBR cadres in many cases collaborate with other health professionals (physicians, physiotherapists, nurses) as a multi-professional and interdisciplinary team. In Gowa, CBR cadres collaborate only with physicians. Patients are also part of the rehabilitation team. PRM physicians are involved in giving counselling in all CBRs. In Bandung, PRMs are available on request.
In Tanah Datar, the cadres do not directly treat children with disabilities, therefore the rehabilitation team interaction approaches mostly only occur between CBR cadres and patients as prosumers. In some cases, the GP at the PHC can be involved. In Tanah Datar, the PRM is invited by the PHC to give specific education and counselling once a year.
Reporting and documentation (2.12). Treatment parameters and paper documentation are used as the basis for reporting and documentation systems in all CBR services, although the format could be different among CBR services.
Funding of service delivery (2.13). In all CBR services, the services delivered related to CBR are free. However, payment for service delivery related to the treatment in PHCs or hospitals is mostly through the state insurance system. In some cases, charity organizations will support prosthetics and orthotists. In other cases, the cadres also support the patients financially (e.g. for transportation). The services and/or support from cadres itself is free.
CBR services were initiated by the WHO following the Declaration of Alma-Ata in 1978, in an effort to enhance the quality of life for people with disabilities and their families, meet their basic needs, and ensure their inclusion and participation (18). The important of rehabilitative care in PHCs is also re-affirmed in the Astana Declaration of PHC (19). One strategy to achieve this is by implementing CBR or integrating rehabilitative services into PHCs. While initially a strategy to increase access to rehabilitation services in resource-constrained settings, CBR is now a multisectoral approach working to improve the equalization of opportunities and social inclusion of PWD, while combating the perpetual cycle of poverty and disability. CBR is implemented through the combined efforts of people with disabilities, their families and communities, and relevant government and non-government health, education, vocational, social, and other services. CBR has been implemented worldwide, not only in developing countries, such as Indonesia (11), China (20), Vietnam (21), Uganda (22), and India (23), but also in developed countries, such as Israel (24) and Singapore (13).
Community-based rehabilitation in Indonesia
In Indonesia, healthcare services are delivered by both the government and private health providers. The Indonesian government implements a decentralization approach for the healthcare system, which means the government of every city and provincial governments manage and provide their own resources. The central or capital city of the country manages and provides its own resources. In addition, the Ministry of Health (MOH) is responsible for tertiary and specialized hospitals, such as the National Cardiac Hospital and National Cancer Hospital. The city government (both Kabupaten and Kotamadya) is responsible for hospitals at the city level and Primary Healthcare (PHC) centres at the district level. Meanwhile, rehabilitation services should be integrated into tertiary and secondary hospitals.
Indonesia signed the United Nations Convention on the Rights for Persons with Disabilities (UN-CRPD) in 2007, and ratified it by the Law No 19/2011 (25). The Law No 8/2016 replaces the previous law ensuring the implementation of UN-CRPD (26). This law supports the implementation of rehabilitation services including for PWD, particularly in the community.
Rehabilitation services in Indonesia have become part of healthcare system (27). According to the Regulation of Ministry of Health of Indonesia, rehabilitation services are provided both in hospitals and in the community (28). Therefore, CBR is also an integrated part of the health-related rehabilitation system of Indonesia (29). CBR in Indonesia is available mainly in districts at the governmental level. In some cases, CBR services are also available at the sub-district level. The main role of CBR is to provide support and assistance to PWD and their families in administrative areas where CBR services are located. Activities of CBR are not only referring and assisting PWD and family, but also early detection.
CBR should have multi-sectoral support, including from the social sector, health sector, educational sector, and employment and labour sector, from non-governmental organizations (NGOs), from the media, and from the community (30). In Indonesia, some CBR services are organized under the city government or are part of PHCs. Most collaborate closely with Social Services. In addition, NGOs and the community, such as YPAC and other foundations (e.g. Siti Hajar Amali Fundation), support CBR, particularly in Bandung.
CBR services can be organized in 2 ways (10). They can be part of the PHC system, as in Tanah Datar, West Sumatra, and Gowa, South Sulawesi. They can alternatively be independent organizations, as in Bandung, although they are under the city government. In Bandung, the CBR services are available at the city, district, and sub-district levels. In this study, only CBR services at the district and sub-district levels were surveyed.
Rehabilitation care can be divided into 5 levels of care: level 1 consists of families and peers; level 2 primary care physicians, physiotherapists (PTs), occupational therapists (OTs), and nurses; level 3 PRMs and specialized PTs, OTs, and nurses; level 4 multi-professional rehabilitation services; and level 5 highly specialized rehabilitation services (10, 31). CBR cadres are at level 1, and the frontline of services for CBR. In Indonesia, CBR cadres are voluntarily workers. They receive training in basic rehabilitation (ADL) by GPs at PHCs, physiotherapists, nurses, or PRM physicians. This also shows that health professionals play a role in educating CBR cadres (10, 31).
CBR cadres are voluntary workers from the village where CBR services are located. They support the government in identifying PWD in the community who might need healthcare support, and recommend and accompany PWD to PHC and/or other healthcare providers. In many cases, they even provide outreach activities, such as ensuring PWD are compliant with treatment and attending to their needs by communicating with PHCs or facilitating further appropriate referrals. Interestingly, in many places in Indonesia, midwives play an important role in society, particularly where physicians or other health professionals and healthcare centres are lacking. Therefore, in Tanah Datar, West Sumatra, midwives are involved in referring patients, particularly children with disabilities. This model works quite well, as midwives have specific knowledge with regards to the health conditions of children.
Rehabilitation services for PWD at CBRs in Indonesia are free. The PWD will only need to pay with state health insurance if they are treated at a PHC or other hospitals. Therefore, concerning the ICSO-R framework, the criteria of spending on service delivery (ICSO-R subcategories 2.13.2) is not relevant for CBR services in Indonesia. This is also the case for the criteria of spending for human resources (ICSO-R subcategories 1.8.2), particularly cadres, as they work voluntarily (without any payment). However, due to the nature of voluntary work (without any payment), another issue arises in the regeneration of the cadres. To solve this problem, the government should propose a strategy in order to attract people to become cadres, particularly with regards to work compensation for CBR cadres.
Patients with severe and chronic health conditions in Indonesia keep increasing (27). Therefore, rehabilitation services are an important health strategy that should be optimally implemented. Considering the lack of rehabilitation provisions in Indonesia, CBR could facilitate rehabilitation services, although it is far from optimum. The CBR cadres should be trained further to give basic rehabilitation treatments (ADL) for people in need, although in many places this type of programme has already been implemented, such as in Bandung. The CBR cadres play a role not only in providing basic rehabilitation services to people in need, but also as frontline workers in collection of data on the early detection of PWD, and mediating referral systems.
The existence of CBR in Indonesia is, without doubt, very important and relevant, particularly in areas where there is no or lacking rehabilitation provisions. The original idea of CBR was as a strategy within community development for rehabilitation, equalization of opportunities, and social inclusion of all people with disabilities. However, considering the importance and relevance of CBR, it should be developed further to reach all people in need.
In the current situation of the COVID-19 pandemic, rehabilitation must be included as part of a national strategy to manage COVID-19 (32). Rehabilitation must be included from the acute phase through to long-term care for this group of patients, as rehabilitation services play a major role in accelerating the recovery of patients with COVID-19 (33). In order to complement healthcare programmes discharging COVID-19 patients who still have lingering effects, CBR services should be developed further to support patients with post-COVID syndrome (33, 34). They can also make up for a lack of rehabilitation services in hospitals during a pandemic. One of the strategies to address this issue is to train CBR cadres in basic rehabilitation skills and knowledge to treat patients with post-COVID syndrome. This can be done by collaborating with health professionals, particularly PRM physicians, GPs, PTs, and OTs. Furthermore, the ICSO-R 2.0 could be used as a framework to develop CBR services from an organizational perspective.
Community-based rehabilitation and ICSO-R
According to the ICSO-R 2.0, providers are defined as “organizational units with the primary goal to provide rehabilitation services. This includes rehabilitation departments of larger hospitals, units within larger multi-purpose departments, stand-alone rehabilitation units (rehabilitation clinics and centres, single practices), and rehabilitation services provided in the community. It excludes hospitals or other organizational units that do not provide rehabilitation services as a primary goal” (7). Therefore, CBRs with a primary goal to deliver rehabilitation services can also be categorized as rehabilitation service organizations. As rehabilitation services, CBRs could also be organized in different ways depending on the local needs and situation. Therefore, to describe CBR in a systematic way could also be a challenge.
The ICSO-R was developed to describe rehabilitation service organizations in a systematic way. During its development to the ICSO-R 2.0, testing was performed and international expert opinions were collected. However, the testing was mainly undertaken in rehabilitation centres and rehabilitation units within hospitals (35). There was a discussion as to whether the ICSO-R can be used to describe CBR. Based on this study, the ICSO-R 2.0 is able to describe not only an independent rehabilitation centre and rehabilitation unit within a larger organization, but can also describe CBR. The use of the ICSO-R 2.0 in different CBR services can, at the same time, compare the CBR services. It can also be used for other purposes, such as improving CBR.
Study limitations
This study has several limitations. The CBR services in this study did not represent all CBR services in Indonesia. Different provinces or cities have different policies or structures for managing CBR services. The lack of value sets for the dimensions, categories, and/or subcategories (e.g. quantitative scores) lead to incomprehensively collected data. In this study, the authors collected some quantitative data with regards to the number of CBR cadres. This was the authors’ initiative, in order to find the number of CBR cadres in each CBR service. The ICSO-R is a framework tool to describe rehabilitation service organizations, which is not commonly used by physicians and other health professionals. Therefore, special training to use and implement the ICSO-R should be performed in advance, in order for reliable data collection to be performed.
Structurally, CBR services are an organization that provides rehabilitation services in the community. Therefore, the ICSO-R 2.0 can also be used to describe CBR. This study shows that the ICSO-R 2.0 is adequately able to describe CBR.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize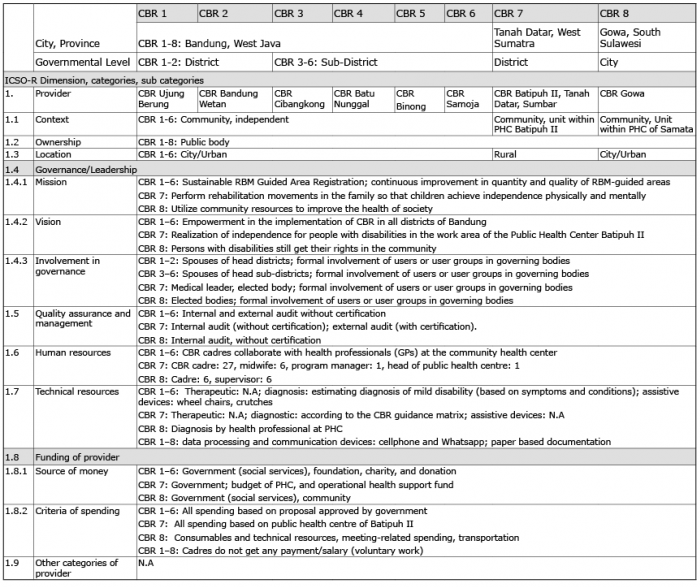 Click to show fullsize
Click to show fullsize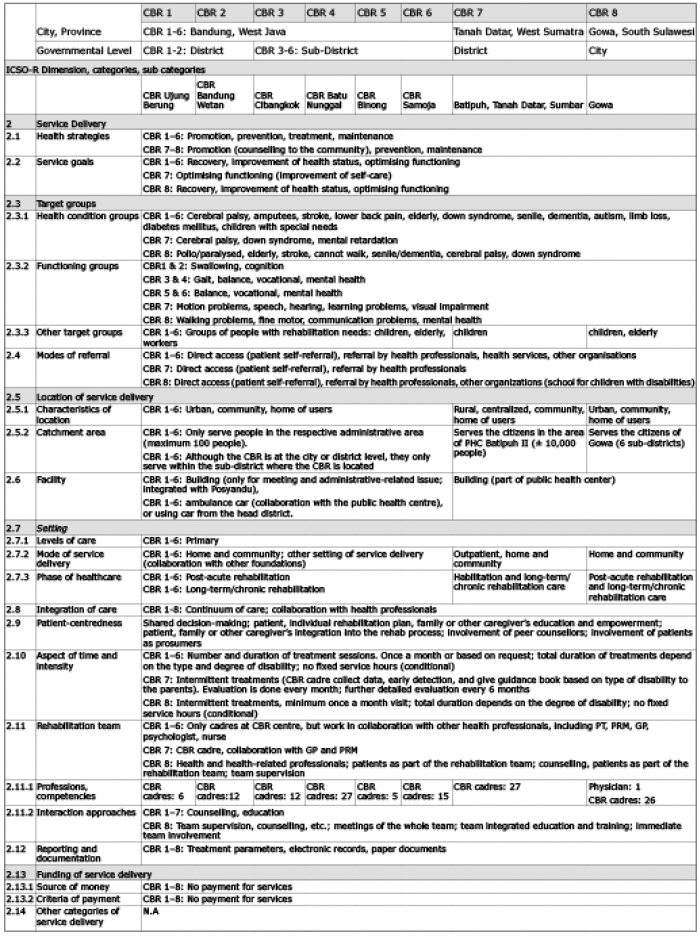 Click to show fullsize
Click to show fullsize