
From the 1Institute of Neuroscience and Physiology, Department of Clinical Neuroscience, Rehabilitation Medicine, 2Institute of Medicine, Department of Molecular and Clinical Medicine, Sahlgrenska, Academy, University of Gothenburg, and Region Västra Götaland, Department of Medicine, Geriatrics and Emergency Medicine, 3Region Västra Götaland, Sahlgrenska, Department of Rehabilitation Medicine and 4Region Västra Götaland, Department of Occupational Therapy and Physiotherapy, Sahlgrenska University Hospital, Gothenburg, Sweden
Objective: To determine the incidence of physical inactivity and factors prior to stroke and in acute stroke that are associated with physical inactivity 1 year after stroke
Design: Prospective longitudinal cohort
Patients: A total of 190 consecutively included individuals with acute stroke
Methods: A follow-up questionnaire, relating to physical activity level using the Saltin-Grimby Physical Activity Scale, was sent to participants in the Fall Study of Gothenburg 1 year after stroke. Predictors of physical inactivity at baseline were identified using univariable and multivariable logistic regression analyses.
Results: Physical inactivity 1 year after stroke was reported by 70 (37%) of the 190 patients who answered the questionnaire and was associated with physical inactivity before the stroke, odds ratio (OR) 4.07 (95% confidence interval (95% CI) 1.69–9.80, p = 0.002); stroke severity (assessed by National Institutes of Health Stroke Scale (NIHSS), score 1–4), OR 2.65 (95% CI) 1.04–6.80, p = 0.042) and fear of falling in acute stroke, OR 2.37 (95% CI 1.01–5.60, p = 0.048).
Conclusion: Almost 4 in 10 participants reported physical inactivity 1 year after stroke. Physical inactivity before the stroke, stroke severity and fear of falling in acute stroke are the 3 main factors that predict physical inactivity 1 year after stroke.
Key words: stroke; physical activity; rehabilitation.
Accepted May 31, 2021; Epub ahead of print Jun 14, 2021
J Rehabil Med 2021; 53: jrm00224
Correspondence address: Sara Botö, Department of Clinical Neuroscience, Institute of Neuroscience and Physiology, Rehabilitation Medicine, Sahlgrenska Academy, University of Gothenburg, Per Dubbsgatan 14, 3rd Fl, SE-413 45 Gothenburg, Sweden E-mail: sara.boto93@gmail.com
Doi: 10.2340/16501977-2852
After a stroke, there is a risk of becoming physically inactive, which could affect one’s health. In order to create a rehabilitation plan with individualized preventive actions and interventions against physical inactivity, it is important, early after stroke onset, to identify patients who are at risk of becoming physically inactive. Previous studies of the early prediction of physical inactivity are few in number, with small sample sizes. This research on 190 individuals describes which factors prior to and in acute stroke (which is the first week after stroke) are associated with physical inactivity 1 year after stroke. The results showed that physical inactivity before stroke, stroke severity, and a fear of falling in acute stroke are associated with physical inactivity 1 year after stroke.
Physical activity has been defined by the World Health Organization (WHO) as ”any bodily movement produced by skeletal muscles that requires energy expenditure” (1). In November 2020, the WHO published updated guidelines for physical activity with the key message that we should become more physically active, regardless of age and function. According to these new guidelines, at least 150–300 min of accumulated physical activity of moderate to vigorous intensity every week are recommended for adults. As physical activity affects our bodies and minds, with a beneficial outcome for all ages and variabilities, these guidelines are important (2). However, 25% of adults worldwide have been reported not to be physically active enough (3). As a result, after a stroke, compliance with the guidelines for physical activity can be even more difficult and the risk of becoming physically inactive can be greater compared with those who have not had a stroke (4–10). A review of 26 studies showed that balance (postural control), degree of physical fitness and walking ability are associated with a higher physical activity level after stroke (4). The sample sizes in the review were generally small, with an age range of 65–75 years. In some studies, the inclusion of the participants was not reported or occurred long after stroke onset (4). In a more recent meta-analysis, physical inactivity was associated with higher age, male sex, low physical function, depression, fatigue, low self-efficacy and poor quality of life (11). However, in only 7 of the 21 studies included, the main aim was to study physical activity level (11). In a small study based on 77 individuals, functional dependence, older age and previous low physical activity level were found to be early determinants of physical inactivity 1 year after stroke (12). The primary driver of this study was to target the knowledge gap related to small sample sizes and few studies based on early prediction, to confirm previous analyses, to increase the confidence in estimates, and to reduce the uncertainty. To enable the early identification of individuals at risk of becoming physically inactive post-stroke and to create individualized rehabilitation plans with preventive actions and interventions against physical inactivity, finding the determinants of physical inactivity is of great clinical interest.
The aim of this study was to determine the incidence of physical inactivity and factors prior to stroke and in acute stroke that are associated with the occurrence of physical inactivity 1 year after stroke. Based on previous research on the early prediction of physical inactivity 6 months after stroke, established in parts of the current population, we hypothesized that a low physical activity level prior to the stroke, stroke severity, the number of drugs and impaired postural control in acute stroke are associated with physical inactivity 1 year post-stroke (13).
This study forms part of the Fall Study of Gothenburg (FallsGOT), with a prospective longitudinal cohort design, which was conducted between October 2014 and June 2016 (14). The main study in FallsGOT aimed to identify variables associated with falls after stroke, and consecutively included 504 patients (14). The inclusion criteria were: 18 years or older, a stroke diagnosis (any of the International Classification of Diseases (ICD) codes I60, I61 and I63), and admission to a stroke unit at Sahlgrenska University Hospital (SU)/Östra in Gothenburg, Sweden. Patients with both first and recurrent strokes were included. The exclusion criteria were those who were unwilling to be part of the project, and patients in a palliative stage. Patients who were being considered for thrombectomy and/or thrombolysis were not admitted to the stroke unit at SU Östra, and were therefore not included in the study.
Ethics approval was obtained from the Swedish Ethical Review Authority in Gothenburg on 25 February 2014 (ref. 004-14) and 9 April 2015 (ref. T301-15, Ad 004-14). Prior to participation in the study, written and oral informed consent was obtained from all participants. FallsGOT was registered at ClinicalTrials.gov (identifier: NCT02264470).
The current study is based on the 190 individuals from FallsGOT who received and answered a postal questionnaire on self-reported physical activity level 1 year after stroke using the Saltin-Grimby Physical Activity Scale (SGPALS) (15, 16). The participants were instructed to select 1 of 4 response options in the SGPALS: 1 = physically inactive, 2 = light physical activity (e.g. walking for at least 3 h a week), 3 = moderate physical activity for at least 3 h a week, and 4 = hard physical activity. The dependent variable, physical inactivity, was defined as SGPALS score 1 and physical activity as SGPALS score 2–4. If the participant did not reply, 1 additional request for study participation was sent by post.
The independent variables (all registered at the stroke unit 12 months earlier) were: age; sex; stroke severity; self-rated physical activity level prior to the stroke; fear of falling; postural control (17); use of a walking aid; number of drugs taken and diabetes mellitus.
To assess fear of falling, the participants were asked the following question: ”Are you afraid of falling? (yes/no)”. Postural control was assessed by a physiotherapist using a 12-item ordinal clinical outcome measurement, the modified version of the Postural Assessment Scale for Stroke Patients (SwePASS) (18–23). In the SwePASS, each item is scored from 0 to 3. A higher score indicates better postural control. The physiotherapist also assessed postural control using tandem standing, 1 item on the Berg Balance Scale (BBS) (17). Tandem standing is scored from 0 to 4. A higher score indicates better postural control. The National Institutes of Health Scale (NIHSS) was used to assess the severity of the stroke and was performed by a trained nurse (24). The NIHSS scores range from 0 to 42, where 0 indicates no stroke symptoms and 42 indicates a severe stroke.
The independent variables were collected within the first 4 days after admission to the stroke unit, with the exception of the number of drugs, which was registered specifically on day 4 or on the day of a fall, if a fall occurred before that. Data relating to the dependent and independent variables were retrieved from the patients’ medical records.
Data analysis
Any association between the dependent variable, physical inactivity at 1 year after stroke, and the independent variables was analysed using univariable and multivariable logistic regression using the Statistical Package for the Social Sciences (SPSS) version 25 (IBM Corp., Armonk, NY, USA). Variables that were significant in the univariable analyses were selected to be included in the final multivariable analysis. In the univariable analysis a value ≤ 0.10 was considered significant, and these values were therefore included in the multivariable analysis. Multicollinearity was assessed in a regression model, to exclude any correlation between the independent variables and the strength of that correlation.
For continuous variables, the means and standard deviations (SD) (medians and interquartile ranges (IQRs)) were given, while numbers and percentages were given for categorical data. For ordinal data, medians and IQRs were used. To test the goodness of fit of the multivariable logistic model, the Hosmer–Lemeshow test, Cox and Snell and Nagelkerke pseudo R2 were used (25). The odds ratios (ORs) with 95% confidence intervals (95% CIs) and the area under the receiver operating characteristic (ROC) curve were used. The significance level was set at a p-value < 0.05.
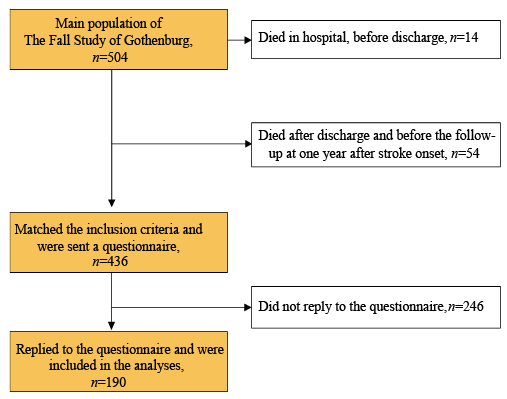
The enrolment process is shown in Fig. 1. A total of 190 participants (90 females; 47%) were included. The baseline characteristics of these participants are shown in Table I. Before stroke onset, 50% of participants reported being physically inactive. After 1 year, the corresponding proportion was 37%. The respondents were older (p = 0.007) and had ischaemic heart disease (p = 0.036) to a greater extent compared with non-respondents. Smoking was more common among the non-respondents (p = 0.022).
Fig. 1. Enrolment process.
Table I. Demographic characteristics at baseline, in the acute phase of stroke, for all participants, those that reported being physically inactive or physically active at 1 year after stroke onset and for non-respondents
The results of the univariable and multivariable logistic regression analyses are shown in Table II. The variables that were statistically significant in the univariable analysis were: age; stroke severity (NIHSS); physical activity level before the stroke; postural control (SwePASS total score and tandem standing); fear of falling; number of drugs; use of walking aid and diabetes mellitus. In the multivariable analysis, the statistically significant variables that were associated with being physically inactive 1 year after stroke were: physical inactivity before the stroke, OR 4.07 (95% CI 1.69–9.80, p = 0.002); stroke severity (NIHSS 1–4), OR 2.65 (95% CI 1.04–6.80, p = 0.042); and fear of falling in acute stroke, OR 2.37 (95% CI 1.01–5.60, p = 0.048).
Table II. Univariable and multivariable logistic regression analysis for prediction of physical inactivity 1 year after stroke
In this sample of 190 individuals, we aimed to determine the incidence of physical inactivity 1 year after stroke, using a single question. Factors prior to the stroke and in the acute setting that were associated with the occurrence of physical inactivity 1 year after stroke onset were also identified. Almost 4 in 10 participants reported being physically inactive 1 year after stroke, and our hypothesis that a low level of physical activity prior to the stroke and stroke severity in acute stroke were associated with physical inactivity 1 year after stroke was confirmed. However, our hypothesis that the number of drugs and impaired postural control in acute stroke were associated with physical inactivity 1 year post-stroke was rejected. Instead, physical inactivity was also associated with a fear of falling in acute stroke.
The knowledge acquired from this study is of clinical importance at the stroke unit to enable the early identification of patients at risk of becoming physically inactive, to improve the planning of individualized rehabilitation, and to prevent a further stroke. In addition, it is also important for professionals in purely preventive healthcare. The area under the ROC curve for the final model in the multivariable analysis indicates that the model is excellent as a diagnostic test (25). The Cox & Snell R2 and Nagelkerke R2 values for the final logistic regression model indicate that the final model constitutes a significant explanation of physical inactivity.
Compared with adults worldwide, where, according to the WHO, 25% report not being physically active enough (3), the proportion of physically inactive adults in the current study population was twice as high prior to stroke. Nevertheless, it is worth noting that the proportion of physically inactive participants decreased from 50% prior to stroke to 37% 1 year after stroke. Despite having a stroke, the fact that 24 individuals reported an increased level of physical activity is positive, although an even higher figure would have been desirable. The fact that the physical activity level increased from prior to the stroke to 1 year after the stroke is in line with previous research (26). The stroke event might have led to a lifestyle change towards a healthier life, such as more training and/or through new support from a physiotherapist, possibly with physical activity on prescription as a supplement. None of these interventions was registered in this current study and, thus, we are unable to relate or comment on their impact. For future research, however, it would be of value and interesting to address this issue.
In this study, participants were included regardless of stroke severity or using a wheelchair. This might lead to a risk of bias. It is highly reasonable that greater stroke severity results in more neurological symptoms; for example, paresis, which could lead to more difficulty mobilizing, with a subsequent risk of becoming physically inactive. On the other hand, individuals who are more immobile than others are likely to have the same ambition to be more active. However, the ORs for being physically inactive 1 year after stroke increased more than 2.6 times for the NIHSS group 1–4 points, compared with the reference group, an NIHSS score of 0 points. The finding that physical inactivity before stroke is associated with stroke severity NIHSS score 1–4, is in line with previous research (27). However, with greater stroke severity (an NIHSS score of 5 or more), there was no statistically significant association with physical inactivity 1 year after stroke.
The fact that a low level of physical activity before stroke is associated with physical inactivity 1 year after stroke is in line with previous findings (12, 28) and with a recently published paper in which physical activity levels were said to be influenced by pre-stroke identity related to physical activity by stroke survivors (29). As physical inactivity prior to a stroke constitutes a risk factor for physical inactivity after a stroke, in parallel with other benefits of physical activity (30), great attention should be paid to physical activity as an intervention with high potential.
Fear of falling in acute stroke was associated with physical inactivity 1 year after stroke. This is in line with a recent publication (31), in which fear of falling was considered to be a barrier to aerobic exercise in individuals with chronic stroke in a developing country (31). Previous studies have shown a difference between women and men with regard to fear of falling, and how fear of falling associates with the risk of falling (14, 32, 33). Women seem to report fear of falling more often than men (14, 32, 33), while falling after stroke is more common among men compared with women (32, 33).
In the present study, postural control (SwePASS) was not associated with low physical activity in the multivariable analysis. Thus, the current study contrasts with the results of FallsGOT at 6 months post-stroke, which showed that impaired postural control in the acute phase was the strongest determinant of low physical inactivity after stroke (13). It can be speculated that these diverging results might be explained by the fact that postural control continues to improve during the first year after stroke (34), while this might not be the case for fear of falling. The result also contrasts with previous research, based on 55 women with a mean age of 74 years, which showed that balance was associated with self-reported physical activity level in a multivariable analysis at 1–3 years after stroke (35). In a previous meta-analysis, male sex was associated with physical inactivity after stroke (11). No such association was found in the current study. The reason is unclear and cannot be explained by skew, as the proportion of men and women is almost the same. Nor were any associations found between age and physical inactivity after stroke, which is also in contrast to previous research showing the association between high age and physical inactivity after stroke (12, 28).
Some limitations should be taken into consideration in the interpretation of the current results. For more than half of the potential participants we have no information on self-reported physical activity level 1 year after stroke, since they did not reply to the SGPALS. Thus, there is a risk that the proportion of participants being physically inactive after stroke could be biased by the low response rate at the follow-up. As already mentioned, there are statistically significant differences between the respondents and the non-respondents in terms of age and in the proportions with ischaemic heart disease and current smokers.
The fact that patients who needed treatment with thrombolysis or thrombectomy were not included in the study constitutes a risk of selection bias. A further limitation is that the SGPALS has not been validated specifically for stroke patients. However, the SGPALS has been validated previously on many elderly patients, where it shows good psychometric characteristics (36–38). The SGPALS, which is a self-report questionnaire, involves only 1 question (36), is inexpensive to use, and saves time for information on physical activity level compared with direct observations or the use of devices such as accelerometers. By using self-reported data instead of a direct measurement to estimate the physical activity level, there is a risk of recall and misclassification bias. Previous research has shown that studies using a self-reported activity level may overestimate the activity level compared with direct measurements (39). If this were the case in the current study, the proportion of physical inactivity would be even higher and it would be even more important to highlight the problem of physical inactivity after stroke. In addition, variables other than those examined, such as support, social activities and self-efficacy, could be of interest, and might be associated with physical inactivity after stroke. The strengths of the current study are the consecutive inclusion, the prospective design, the recommended and well-defined follow-up point (40) and the fairly large population size.
In conclusion, 37% of participants in this study reported being physically inactive 1 year after stroke, compared with 50% prior to stroke. Physical inactivity 1 year after a stroke was associated with physical inactivity before the stroke, stroke severity (NIHSS score 1–4) and fear of falling in acute stroke. Although this study has a larger sample size than previous studies of the early prediction of physical inactivity, a further study with an even larger sample size and with direct measurements of physical activity level would be of interest. It would also be of interest in future studies to change the focus to identifying factors that predict a good level of physical activity after stroke.
The authors thank all the participants in the FallsGOT and stroke unit 354 at Sahlgrenska University Hospital. The study was financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF agreement (881811).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize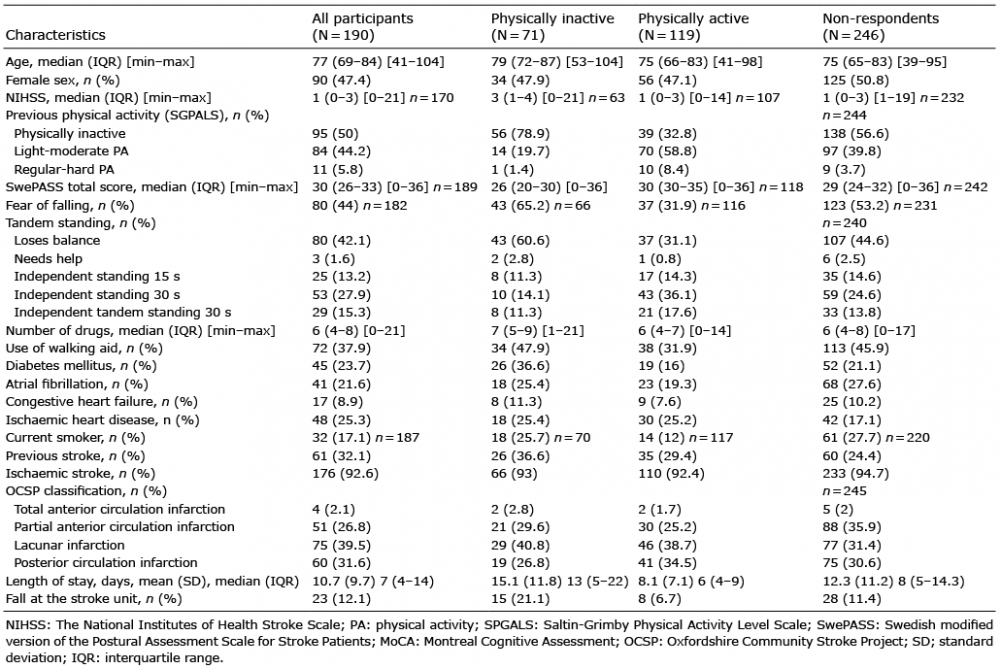 Click to show fullsize
Click to show fullsize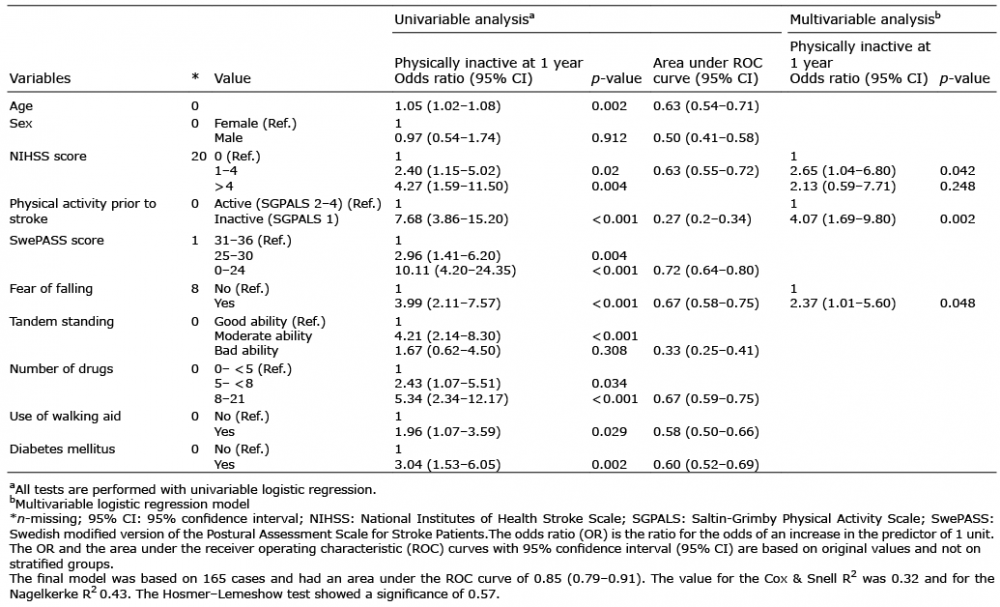 Click to show fullsize
Click to show fullsize