
From the 1Department of Health Sciences, Lund University, Lund, 2Department of Neurology, Rehabilitation Medicine, Memory Disorders and Geriatrics, Skåne University Hospital, and 3Department of Clinical Sciences, Lund University, Lund, Sweden
Objective: To assess the occurrence of self-reported fatigue among men and women who have returned to work after stroke, and the association between 2 fatigue rating scales.
Design: A cross-sectional study.
Subjects: A total of 91 adults (58 men/33 women, mean age 53 years) with mild to moderate disability.
Methods: Questionnaires were posted to participants approximately one year after stroke. Fatigue was assessed with the Fatigue Severity Scale (FSS) and the Mental Fatigue Scale (MFS).
Results: In total, 58% of the women and 33% of the men reported fatigue on the FSS (total score ≥ 4), and 46% of the women and 28% of the men reported mental fatigue on the MFS (total score ≥ 10.5). Being easily fatigued, decreased motivation, mental fatigability and sensitivity to stress were the most reported problems. FSS and MFS were moderately associated (rho 0.517–0.732).
Conclusion: Fatigue is common among persons who have returned to work after stroke, and interferes with daily life. The long-term consequences of fatigue should be addressed after stroke, especially in women. The FSS and the MFS can be used in combination, as they provide information on different aspects of fatigue.
Key words: cerebral stroke; data correlation; disability evaluation; mental fatigue; return to work; self-assessment; stroke rehabilitation.
Accepted Jul 9, 2021; Epub ahead of print Aug 3, 2021
J Rehabil Med 2021; 53: jrm00227
Correspondence address: Anna Norlander, Skånes universitetssjukhus, Rehabiliteringsmedicin mottagning, 221 85 Lund, Sweden. E-mail: anna.norlander@med.lu.se
Doi: 10.2340/16501977-2863
Fatigue can be a long-lasting and disabling impairment following stroke. There is a need for increased knowledge of how fatigue affects people who have returned to work after stroke, and which fatigue rating scales capture their problems most appropriately. The aim of this study was to assess the occurrence of self-reported fatigue among men and women who have returned to work after stroke, and to determine the association between 2 fatigue rating scales. The study was based on a postal survey and includes 91 participants. Fatigue was found to be common 1 year after stroke, especially in women, and interfered with daily life. The 2 fatigue rating scales could be used in combination, as they provide different information on fatigue. The findings could be used to develop support that enables people with stroke to return to and to stay at work long-term.
Stroke is one of the most common causes of long-lasting disability among adults (1, 2). In Sweden, approximately 26,000 persons have a stroke annually (3). Because of an increasing incidence of stroke among young people (4) many live with its consequences for a significant part of their lives. Common impairments following stroke include reduced sensorimotor and cognitive functions, as well as fatigue (5–7). Due to advances in acute treatments and rehabilitation, more people recover from their initial neurological impairments. Despite this, post-stroke fatigue can be a persisting and severely disabling problem (8).
Fatigue is defined as a subjective lack of physical and/or mental energy that interferes with various activities (9). It is related to reduced quality of life (10, 11), increased dependence in ADL (12) and increased mortality (12, 13). Fatigue can also have a negative impact on social participation, driving, reading, sleeping and return to work (8). Although fatigue is reported by 25–85% of stroke survivors during the first 2 years after stroke, the occurrence of post-stroke fatigue remains unclear due to large heterogeneity between studies (9). Women may experience more fatigue than men (7, 14), although the mechanisms behind this, or in what situations fatigue occurs, are poorly described.
In addition, people with mild stroke (15, 16) who have returned to work (17) may experience fatigue, which could lead to difficulties in maintaining work (18). Our previous study (19) revealed that ”invisible” impairments, including fatigue, contributed to people feeling uncertain about their working capacity after stroke. They also had difficulties expressing what kind of help they needed to deal with their problems. Overall, knowledge regarding the occurrence of fatigue among people who have returned to work and its influence on daily life and work capacity is limited. Such knowledge is important to be able to provide adequate rehabilitation and support that enables people to return to work and stay at work after stroke.
Fatigue is most often assessed using self-reported rating scales. Several scales are available, but no consensus exists regarding which scale should be preferred after stroke. Currently, the Fatigue Severity Scale (FSS) is the most used in stroke research (9). The FSS mainly targets fatigue defined as a sense of physical tiredness and lack of energy (20). However, people with stroke also commonly experience mental fatigue; characterized by difficulties performing mentally strenuous tasks for more than short periods, increased irritability, sensitivity to stress, concentration difficulties and emotional instability (21). The Mental Fatigue Scale (MFS) was constructed to capture the impact of mental fatigue on various life situations (22).
Taken together, there is a need for increased knowledge of how fatigue affects people who have returned to work after stroke, and which fatigue rating scales most appropriately capture their problems. Therefore, the aims of this study were to assess: (i) the occurrence of self-reported fatigue among men and women who have returned to work after stroke; and (ii) the association between FSS and MFS (i.e. whether these measures can replace or complement each other).
Study design
This study is part of a larger project on return to work among people with mild to moderate disability following stroke. It is based on a postal survey targeting personal factors, work ability, working situation and perceived consequences following stroke, including fatigue, one year after stroke. In the current study, only data on fatigue are presented.
Participants
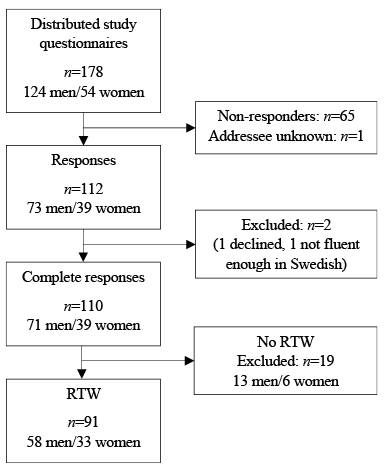
Participants were identified through monthly screening of patients admitted to Skåne University Hospital, which is the third largest hospital in Sweden. The uptake area covers 14 municipalities, consisting of both rural and urban areas. Inclusion criteria were: age 18–64 years; having had a stroke (i.e. cerebral infarction, intracerebral haemorrhage or subarachnoid haemorrhage) 10–14 months previously; referred to the stroke rehabilitation outpatient clinic at Skåne University Hospital within 180 days after stroke onset; and worked at least 25% of full-time employment prior to the stroke. Exclusion criteria were: extensive language deficits, severe cognitive impairment or not being sufficiently fluent in Swedish to answer the questionnaire. Participants were consecutively included in the survey from March 2017 to August 2019. A total of 178 persons were sent the questionnaires, and 110 completed the survey. Of these, 91 persons (83%) had returned to work (RTW) after stroke and were included in the current study (Fig. 1).
Fig. 1. Flow chart showing the inclusion of participants. RTW: return to work.
Data collection
The postal survey comprised an invitation letter including information about the research project, a form of written informed consent, questions on demographics and work situation, a set of questionnaires regarding perceived work ability, fatigue (see below), physical and cognitive disabilities after stroke (according to the Stroke Impact Scale; SIS) (23) and a pre-paid return envelope.
Assessment of post-stroke fatigue
To assess self-reported fatigue, the 9-item Swedish translated version of the Fatigue Severity Scale (FSS) (24) and the Swedish Mental Fatigue Scale (MFS) (22) were used.
The FSS consists of 9 statements concerning the impact of fatigue on daily life, e.g. ”My motivation is lower when I am fatigued”. Items are scored on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). The total score represents the mean of the 9 statements and ranges from 1 to 7, where a greater score indicates more fatigue (20). Most commonly, a cut-off score of ≥ 4 is used to classify post-stroke fatigue (9). The FSS has demonstrated adequate validity and reliability in other diagnoses (24, 25) and satisfactory internal reliability after stroke (26, 27).
The MFS consist of 15 questions targeting different symptoms of mental fatigue, including affective, cognitive and sensory symptoms, duration of sleep and daytime variation in symptom severity (during common activities). Each item has 4 response options: 0 corresponds to normal function, 1 indicates a problem, 2 a pronounced symptom, and 3 a maximal symptom. It is also possible to select a rating between 2 response options (i.e. 1.5, 2.5, etc.). Items 1–14 are used to calculate the total score, whereas item 15 provides additional information on daytime variation of symptoms. A total score ≥ 10.5 indicates fatigue (28). The MFS was constructed to capture mental fatigue irrespective of illness and has demonstrated high internal consistency in neurological conditions including stroke (22). It has shown ability to identify self-perceived fatigue among people with mild stroke compared with healthy subjects (21) irrespective of age, sex and education (28).
Data analysis
Descriptive statistics were used to characterize the participants’ demographics and clinical characteristics. Relative frequencies, medians and quartiles were used to describe occurrence of self-reported fatigue among men and women, as assessed by the FSS and MFS. To promote meaningful interpretation of the data, the item scores were categorized into 2 and 3 severity levels, respectively. For the FSS, an item score between 1 and 3 was considered disagreement (i.e. no or minor problem) and ≥ 4 as agreement (i.e. moderate to severe problem). For the MFS, item scores 0–0.5 were categorized as normal function, 1–1.5 as a problem, and 2–3 as pronounced to maximal symptoms. The proportion of participants with fatigue was determined using the recommended cut-off levels for the FSS total score (≥ 4) (9) and for the MFS total score (≥10.5) (28).
To test for differences in reported fatigue among men and women, the Mann–Whitney U test was used for individual items and total scores. Associations between the 2 fatigue scales were calculated using Spearman’s rank correlation coefficient. The strength of the correlations was interpreted as: rho < 0.3 negligible; 0.3 to < 0.5 low; 0.5 to < 0.7 moderate; 0.7 to < 0.9 high; and ≥ 0.9 very high (29). p-values < 0.05 were considered significant in all analyses. All statistical analyses were performed using IBM SPSS Statistics for Windows (Version 26.0. Released 2019. Armonk, NY: IBM Corp).
Ethics considerations
The study was approved by the Regional Ethical Review Board in Lund, Sweden (Dnr 2016/1064). Written informed consent was obtained from all participants before inclusion, and the principles of the Declaration of Helsinki were followed. All data were handled confidentially and securely stored separate from any personal contact information.
Participants
As shown in Table I, 58 (64%) men and 33 (36%) women, age range 29–65 years (mean 53 years, SD 8), were included. The majority had had a stroke due to a cerebral infarction and perceived themselves to be fairly well recovered from their stroke. Most participants reported no or minor problems with memory, cognition, strength and mobility, but approximately one-quarter perceived some limitations regarding work and leisure activities, as assessed by the SIS. All participants had returned to work after stroke, and all but 3 were still working at the time of answering the survey. Sixty-eight percent of the participants worked at least 75% of full-time employment, and 19% of the men and 30% of the women had a lower degree of employment compared with before stroke.
Table I. Participants’ characteristics approximately 1 year after stroke (n = 91)
Occurrence of self-reported fatigue
Fatigue Severity Scale. As can be seen in Table II, both men and women reported problems with fatigue on the FSS. Among the men, 57% agreed (i.e. item score ≥ 4) that they were easily fatigued and 47% that fatigue was 1 of their 3 most disabling symptoms. Sixty-nine percent of the men agreed that their motivation was lower when fatigued, and 47% that fatigue interfered with their physical functioning. Approximately one-third of the men reported that their fatigue caused frequent problems, prevented sustained physical functioning, interfered with duties and responsibilities and interfered with work, family or social life. Only 10% of the men agreed that exercise brought on their fatigue. Median item scores ranged from 2 to 5, with the highest scores (i.e. highest agreement) for the statement ”My motivation is lower when I am fatigued” (median 5, IQR 6–3) and the lowest for ”Exercise brings on my fatigue” (median 2, IQR 2–1). The men’s total FSS scores ranged from 1 to 6 (out of a maximum of 7) with a median of 3. In total, 33% of the men scored above the established cut-off level for fatigue (i.e. total score ≥ 4).
Table II. Score distribution (%) and median scores for individual items and total score of the Fatigue Severity Scale (FSS) among the 58 men and 33 women
Among the women, 76% agreed that they were easily fatigued and 64% that fatigue was one of their 3 most disabling symptoms. Seventy-nine percent of the women agreed that their motivation was lower when fatigued. Approximately two-thirds of the women reported that fatigue interfered with carrying out certain duties and responsibilities, with their physical functioning and with work, family, or social life. Approximately half of the women agreed that fatigue caused them frequent problems and that it prevented sustained physical functioning. One-third of the women agreed that exercise brought on their fatigue. Median item scores ranged from 3 to 6, with the highest scores for ”My motivation is lower when I am fatigued” (median 6, IQR 6–4) and the lowest for ”Exercise brings on my fatigue” (median 3, IQR 4–1). The women’s FSS total scores ranged from 1 to 6, with a median of 5. In total, 58% of the women scored above the cut-off level for fatigue.
The women had significantly higher FSS scores than the men in 6 out of 9 items, and a significantly higher total score (p = 0.006).
Mental Fatigue Scale. As can be seen in Table III, both men and women reported symptoms of mental fatigue according to the MFS. Among the men, 59% reported at least some degree of problem (i.e. item score ≥1) with mental fatigability and 53% with sensitivity to stress. Between 33% and 38% reported problems with memory, fatigue in general, lack of initiative, concentration difficulties and slowness of thinking. The other symptoms were reported as problematic by over 20% of the men. Pronounced or maximal symptoms (i.e. item score ≥ 2) were most common for sensitivity to stress, mental fatigability and concentration difficulties (reported by 9–19% of the men). For the remaining items, the proportion with pronounced symptoms was less than 5%. Median item scores varied between 0 and 1 (out of 3), with the highest scores (i.e. most symptoms) for mental fatigability and sensitivity to stress (median 1.0, IQR 1.5–0.0) and the lowest for mental recovery and decreased/increased sleep (median 0.0, IQR 0.5–0.0). The men’s total MFS scores ranged from 0 to 22 (out of a maximum of 42) with a median of 7.5. In total, 28% of the men scored above the cut-off level for fatigue (total score ≥ 10.5).
Table III. Score distribution (%) and median scores for individual items and total score of the Mental Fatigue Scale (MFS) among the 58 men and 33 women
Among the women, as many as 85% reported some degree of problem with mental fatigability. Between 61% and 67% experienced problems with fatigue in general, sensitivity to stress and concentration difficulties. More than half, 54–58%, reported problems with lack of initiative, emotional instability, sensitivity to noise, irritability and slowness of thinking. Forty-six percent reported problems with memory and 30–39% with mental recovery, sensitivity to light and decreased/increased sleep. Pronounced or maximal symptoms were most common for mental fatigability, sensitivity to stress, mental recovery and sensitivity to noise (reported by 12–39% of the women). For the remaining items, the proportion with pronounced symptoms was less than 10%. Median item scores varied between 0 to 1.5, with the highest score for mental fatigability (median 1.5, IQR 2.0–1.0) and the lowest for sensitivity to light and decreased sleep (median 0.0, IQR 1.0–0.0). The women’s total MFS scores ranged from 1 to 22, with a median of 9.5. In total, 46% of the women scored above the cut-off level for fatigue.
The women had significantly higher MFS scores than the men in 8 out of 14 items, and also a significantly higher total score (p = 0.013) (see Fig. 2).
Fig. 2. Bar chart demonstrating the proportion of men (n = 58) and women (n = 33) with fatigue according to established cut-off levels for the Fatigue Severity Scale (FSS) and the Mental Fatigue Scale (MFS).
Association between the 2 rating scales
As shown in Table IV, the FSS and the MFS were significantly correlated, both regarding the total scores (rho 0.732, p < 0.001) and with respect to the occurrence of fatigue according to the cut-off levels (rho 0.517, p < 0.001). The association for the total scores was slightly stronger among men (rho 0.697) than among women (rho 0.667), whereas the association for occurrence of fatigue according to the cut-off levels was slightly stronger among the women.
As shown in Fig. 2, a larger proportion of participants with fatigue were identified with the FSS compared with the MFS among both men and women. The results also show that, although the ratings on the 2 scales were associated, there were some discrepancies (Table V). Among those who scored above the FSS cut-off for fatigue, 42% of the men and 32% of the women were below the cut-off for the MFS. Conversely, among those with fatigue according to the MFS, 31% of the men and 13% of the women did not reach the cut-off for the FSS. This means that 19% of the men and 40% of the women had fatigue according to both scales, and an additional 23% of the men and 24% of the women according to only one of the scales.
Table IV. Association (rho) between the Fatigue Severity Scale and the Mental Fatigue Scale regarding total scores and occurrence of fatigue according to cut-off levels
Table V. Cross table showing the proportion of men and women (% men/women) with self-reported fatigue, as assessed by the Fatigue Severity Scale and the Mental Fatigue Scale (total score above cut-off), n = 58 mena/33 women
This study shows that self-reported fatigue is relatively common among persons who have returned to work approximately one year after stroke, and that it interferes with functioning and everyday life in different ways. Two-thirds of the women and almost half of the men reported fatigue (i.e. total score ≥ cut-off) on at least 1 of the 2 rating scales FSS and MFS. Being easily fatigued, decreased motivation, mental fatigability and sensitivity to stress were among the most commonly reported problems. The 2 fatigue rating scales were moderately associated, indicating that they capture somewhat different aspects of self-reported fatigue.
The results of the current study confirm previous qualitative studies showing that fatigue is a common and disabling problem among people with mild stroke (30, 31) and among those who have returned to work (18). The occurrence of fatigue in the current study sample ranged between 34% and 42% depending on the rating scale used. This is in agreement with previous studies that show a prevalence of fatigue between 23% and 40% in people with mild stroke or transient ischaemic attack (TIA) (32). Although studies that have investigated fatigue after return to work are few, the current results are in agreement with the study by Andersen et al. (17), who found that 46% of the participants who were employed 2 years after stroke still experienced fatigue.
Our findings of higher reported prevalence of fatigue in women compared with men is consistent with other studies (7, 14), even though the underlying mechanisms are unclear. One contributing factor might be sex-related differences in daily life responsibilities, where women more often take responsibility for the household, children and caring for older relatives in addition to working life. In the current study, the most significant difference between men and women was found for the FSS item ”Fatigue interferes with carrying out certain duties and responsibilities”, where the proportion of women who agreed was twice that of men.
When analysing data at the item level we found that the FSS item with the lowest scores (i.e. low agreement) was item 2: ”Exercise brings on my fatigue”, which indicates that exercise does not commonly worsen fatigue. This adds important knowledge, as there is limited research regarding the impact of exercise on post-stroke fatigue. Physical activity and exercise are key components of secondary prevention after stroke (33). It is therefore of importance to point out that exercise does not necessarily worsen fatigue, which, in itself, is often perceived as a barrier to exercise (34) and has been linked to a higher mortality rate because of its association with a sedentary lifestyle (12). In addition, the MFS ratings show that specific symptoms of mental fatigue are especially common, such as increased mental fatigability and sensitivity to stress, which were reported by the majority of both men and women, whereas sensitivity to light and sleep disturbances were not particularly common in this group.
A larger proportion of participants with fatigue (according to the cut-off levels) were identified using the FSS compared with the MFS. This may be due to the scales capturing different aspects of fatigue. Whereas the MFS targets a number of predefined symptoms of mental fatigue and asks the respondent to rate his or her situation in comparison with how it was before stroke, the FSS focuses on how fatigue affects everyday life in general, including work, social and physical activities. As the scales provide different types of information, direct comparison regarding their sensitivity in detecting fatigue is difficult. However, our findings indicate that using both scales in combination increases the possibility of detecting persons who experience problems with fatigue. In fact, fatigue was identified among 42% of the men and 64% of the women for at least one of the rating scales when used in combination, which is more than if only one of the scales is used. As indicated by the moderate correlation between the MFS and the FSS, not all those who experience problems with fatigue in daily life (i.e. above the cut-off on the FSS) have mental fatigue (i.e. above the cut-off on the MFS). However, most of those who had fatigue according to only one of the rating scales scored fairly close to the cut-off levels on both. High ratings on individual items should be considered even if a person does not score above the established total score cut-off levels.
Methodological considerations
Regarding the fatigue rating scales used in the current study, the MFS has been developed specifically to assess fatigue after stroke, but is not yet widely used internationally. This makes direct comparison with other studies difficult. The symptoms of mental fatigue in the MFS can also be related to depression and cognitive impairments (21, 28). However, mental fatigue has been determined a separate construct that should not be confused with depression (21, 35). Further evaluation of the psychometric properties of the MFS is needed in future research. Regarding the FSS, the fact that it rests on the patient’s own definition of fatigue can be considered both a strength and a limitation. The validity of the FSS after stroke has been questioned, as the respondents may not be able to distinguish their fatigue from their neurological deficit (36). A 7-item version of the FSS (item 1 and 2 removed) has been suggested to be more valid in stroke populations (37), but the validity needs to be further studied among people with mild to moderate stroke and among those who have returned to work. Moreover, not all who report problems with fatigue during an interview score above the cut-off for the FSS (7). In a qualitative study, based on semi-structured interviews, fatigue was identified in as much as 72% of the participants one year after mild stroke (15). Taken together, this indicates a need to further develop how post-stroke fatigue is defined and assessed.
Clinical implications
The findings of the current study highlight the need to address fatigue among people who have returned to work after stroke, and to use rating scales that capture various fatigue-related problems. Recovering from a stroke and adapting to a life with impairments takes time. Problems with fatigue may enhance as demands increase; for example, when one resumes work and other responsibilities, but few persons, on work resumption, have any ongoing rehabilitation (38). Difficulties in understanding and expressing ones problems and needs, and the fact that few seem to talk about problems related to fatigue with their doctor (7) may lead to long-term restrictions in participation (39). Fatigue does not appear to resolve spontaneously, but may even increase over time (16). Increased problems with fatigue during the first year after stroke has been associated with a reduction in professional activity (40). Thus, fatigue might be a contributing factor to why several participants in the current study reported limitations in work and leisure activities despite relatively mild impairments.
To enable people with stroke to return to and stay at work, there is a need for increased awareness about post-stroke fatigue in healthcare, as well as among persons with stroke, their families and employers. Supporting people to develop efficient fatigue management strategies could potentially improve their long-term health and well-being. The findings of the current study indicate that fatigue management interventions should target all areas of life, including work, family, social life and physical activity. Specific symptoms, as well as the patient’s health and life situation as a whole, need to be considered. In the assessment of fatigue, it is important to be aware that different fatigue rating scales provide different types of information. Moreover, all fatigue-related information should be considered, not merely if the total score is above or below a cut-off (i.e. fatigue/not fatigue). Distinguishing between different types of fatigue (e.g. physical and mental fatigue) and how these are exacerbated by activities and environments is necessary when advising on self-management strategies (41). Currently, there is limited consensus regarding the definition of post-stroke fatigue or its underlying mechanisms, which underscores the importance of further research. More research is also needed regarding factors influencing self-reported fatigue among people who have returned to work after stroke, including sex, stroke characteristics and working situation.
Strengths and limitations
A strength of this study is that 2 different fatigue rating scales, which provide complementary information, were used for the data collection. By analysing the data at the item level, and with special attention to differences between men and women, we could provide more detailed and clinically relevant results. A limitation is that more men than women were included in the study. However, this corresponds to the sex distribution among those who have a stroke before the age of 65 years in Sweden (3). As the study included participants with mostly mild to moderate disabilities who had returned to work, the findings cannot be generalized to stroke survivors with more severe disabilities. Since the assessments were based on self-reports administered by a postal survey, people with severe language or cognitive deficits were excluded. The relatively low response rate (63%) of the survey is also a limitation. The fact that this study targeted people in mid-life who had returned to work after stroke might have contributed to several people not responding.
Conclusion
The results of this study indicate that fatigue is a common problem among persons who have returned to work after stroke. Consequences of fatigue should be addressed long term after stroke, especially in women, as they report more fatigue-related problems. The 2 fatigue rating scales, FSS and MFS, can be used in combination, as they provide information on different aspects of fatigue.
Funding. The study was supported by grants from NEURO Sweden and ”Stiftelsen för bistånd åt rörelsehindrade i Skåne”.
The authors thank all persons who participated in the study and Michael Miller RTP, PhD, for language editing.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize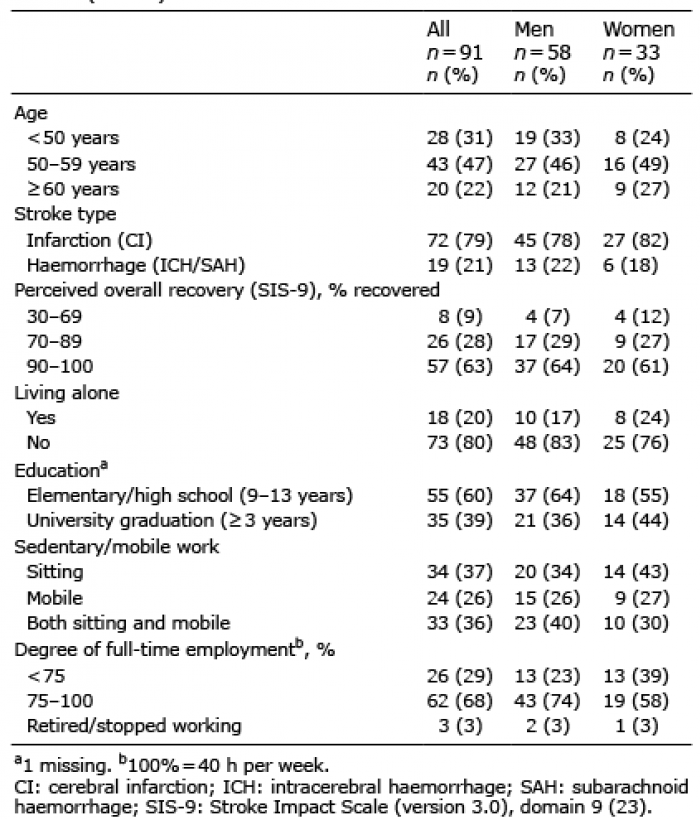 Click to show fullsize
Click to show fullsize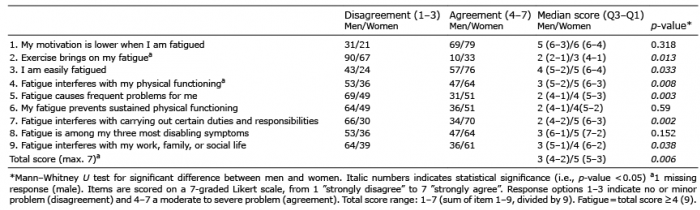 Click to show fullsize
Click to show fullsize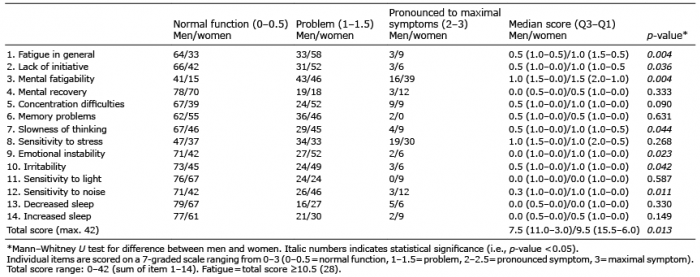 Click to show fullsize
Click to show fullsize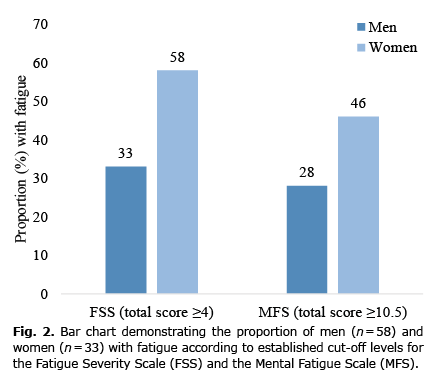 Click to show fullsize
Click to show fullsize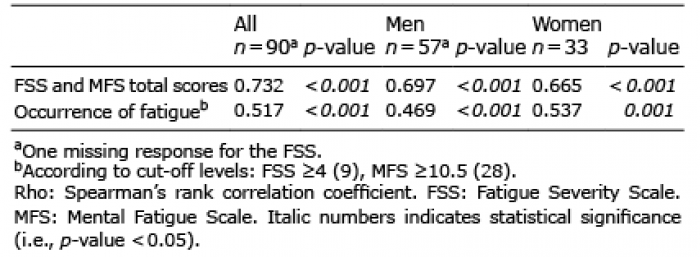 Click to show fullsize
Click to show fullsize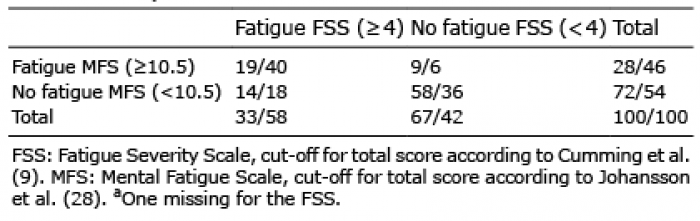 Click to show fullsize
Click to show fullsize