
From the 1Health Rehabilitation Group, University of Antioquia, Medellín, Colombia and 2Department of Rehabilitation Medicine, Hannover Medical School, Hannover, Germany
Objective: To describe adaptations in the provision of rehabilitation services proposed by scientific and professional rehabilitation organizations to avoid interruptions to patients’ rehabilitation process and delays in starting rehabilitation in patients with COVID-19.
Methods: A narrative review approach was used to identify the recommendations of scientific and professional organizations in the area of rehabilitation. A systematic search was performed in the main databases in 78 international and regional web portals of rehabilitation organizations. A total of 21 publications from these organizations were identified and selected.
Results: The results are presented in 4 categories: adequacy of inpatient services, including acute care services and intensive care unit for patients with and without COVID-19; adequacy of outpatient services, including home-based rehabilitation and tele- rehabilitation; recommendations to prevent the spread of COVID-19; and regulatory standards and positions during the COVID-19 pandemic expressed by organizations for protecting the rights of health workers and patients.
Conclusion: Health systems around the world are rapidly learning from actions aimed at the reorganization of rehabilitation services for patients who are in the process of recovery from acute or chronic conditions, and the rapid response to the rehabilitation of survivors of COVID-19, as well as from efforts in the prevention of contagion of those providing the services.
Key words: rehabilitation service; COVID-19; disability; health professional; rehabilitation organization; health system.
Accepted Jul 23, 2021; Epub ahead of print Aug 24, 2021
J Rehabil Med 2021; 53: jrm00228
Correspondence address: Luz Helena Lugo Agudelo, Antioquia, University of Antioquia, 050010 Medellín, Colombia. E-mail: luzh.lugo@gmail.com, luz.lugo@udea.edu.co
Doi: 10.2340/16501977-2865
In response to the coronavirus disease 2019 (COVID-19) pandemic, which developed very rapidly worldwide, rehabilitation services were forced to modify and adapt the way they provide and deliver services. These measures were proposed and adopted across a wide range of countries, the changes proposed included the following measures: critical patients with SARS-CoV-2 infection should be cared for by a multidisciplinary team providing early mobilization, respiratory, outpatient, and long-term care rehabilitation interventions. Home- based and community rehabilitation can be delivered through different strategies, such as telerehabilitation or direct care. The use of measures to prevent and protect against transmission of COVID-19 are necessary for all patients in rehabilitation care.
The coronavirus disease 2019 (COVID-19) pandemic expanded very rapidly worldwide. Because of its rapid spread, morbidity, and mortality, COVID-19 has had a significant impact on the delivery of healthcare, including rehabilitation services. Globally, rehabilitation services have been forced to modify and adapt the way they provide and deliver services in response to the pandemic, aiming to reduce physical contact between professionals and patients without affecting communication in the rehabilitation process (1). Furthermore, restrictions to contain the spread of COVID-19 have limited patients’ access to many rehabilitation services, causing collateral damage and negative consequences to people with disabilities, increasing functional limitations in chronic conditions, and hampering recovery after acute events (2).
The World Health Organization (WHO) called for action to strengthen rehabilitation planning and implementation, including sanitary emergency preparedness and response to the current COVID-19 pandemic (3).
However, the rehabilitation processes of people experiencing disability as well as of people with disability have been affected by the lack of continuity of care in rehabilitation services. It is estimated that, due to the pandemic at March 31st 2020, an estimate range of 1,3–2,2 million people in Europe have had to interrupt their rehabilitation treatments in all phases of their conditions: acute, post-acute and long-term (4).
Demographic and epidemiological trends suggest that the key indicators of the health of populations will be affected by the pandemic; not only mortality and morbidity, but also functioning. This, in turn, means that the primary focus of healthcare will need to include the scaling up and strengthening of rehabilitation (5).
Furthermore, rehabilitation might benefit any person with rehabilitation needs, patients with any specific health condition(s), persons with any specific impairment, activity limitations and/or participation restrictions, from any cause, at any stage of illness or age. Rehabilitation might be delivered in any location (e.g. rural area, urban area, community, centralized, decentralized); in any mode of service delivery (e.g. inpatient or outpatient settings, day hospital, day services, home and community rehabilitation, telerehabilitation); and there is also consensus that rehabilitation must include habilitation, pre-habilitation, acute, sub-acute post-acute and long-term chronic rehabilitation care (6).
The objectives that a rehabilitation service plans and aims to achieve include: recovery; improvement of health status; optimizing functioning, such as improving self-care; returning to normal life; returning home; returning to work; improving quality of life services; increasing hospital discharge rates; and decreasing complications and hospital readmissions (6). As a consequence of the current pandemic, there is a need to identify barriers and facilitators to providing rehabilitation services, and to develop new sets of skills to meet the varied needs in these different settings (7).
Even during a pandemic, rehabilitation is one of the 5 key health strategies (5). Rehabilitation is an essential part of the continuum of care, prevention, promotion, treatment, and palliation, and should therefore be considered an essential component of integrated health services (8). Rehabilitation is part of universal health coverage, which ensures all people in need, including people with disabilities, reach and maintain an optimal functioning level in interaction with the environment (9).
The main aim of this study is to describe the adaptations to rehabilitation services proposed by scientific and professional rehabilitation organizations for the rehabilitation care of patients with and without COVID-19 in both inpatient and outpatient settings. The secondary objectives are to describe preventive measures to reduce the spread of COVID-19, and regulatory measures for protecting health workers and patients’ rights.
A narrative review, based on information published on websites, was performed to identify scientific and professional rehabilitation organizations’ recommendations concerning the adaptation of rehabilitation services for people with rehabilitation needs during the COVID-19 pandemic.
Research question
What do scientific and professional rehabilitation organizations recommend regarding the adaptation of rehabilitation services for people with rehabilitation needs during the COVID-19 pandemic and for preventing the spread of COVID-19 in different rehabilitation settings?
Search
Based on the research question, a medical librarian conducted a systematic web search to identify national and international rehabilitation organizations. The International Society for Physical Medicine and Rehabilitation (ISPRM) publishes the most complete list of organizations, from which the websites of 78 organizations were searched to identify specific reports, guidelines and documents. The searches were conducted in April 2020 and updated in February 2021. Based on these searches, publications of 21 organizations (listed in Appendix S11) were selected for inclusion in the study.
Selection and extraction of information
A total of 78 international and regional web portals of rehabilitation organizations and associations were identified. Then, associations that answered the objective of this synthesis through reports, guidelines and specific related documents were selected. A total of 21 associations, that issued adaptations regarding the provision of rehabilitation services in order to avoid interruption of, or delay in starting, the rehabilitation process in patients with or without COVID-19, were included in the study. Information from these 21 associations was updated until February 2021.Four researchers with expertise in rehabilitation services screened the search results and selected 21 publications from the following physical medicine and rehabilitation organizations and other related professions. (See Appendix S1).
Data extraction was conducted by 6 researchers (MAS, KMC, AP, JCV, LM,RD) using a pre-defined form to record information regarding proposed adaptations in the provision of rehabilitation services according to the following categories: individual coronavirus prevention for health rehabilitation professionals; outpatient rehabilitation services; inpatient rehabilitation services; patient education (COVID-19 webinar series); telerehabilitation; professional education (COVID-19 webinar series); research-related to COVID-19; community support; institutional settings or homecare; legislation for skilled health workers; support for professionals; and financial resources for rehabilitation.
Data synthesis was performed by 4 researchers (LHL, RD, CMV, DFP) with expertise in systematic reviews and rehabilitation services. In the synthesis stage, the information about adaptations was discussed among the 4 researchers and was reorganized into 4 categories:
Adequacy of inpatient services
The adequacy of inpatient rehabilitation services during the COVID-19 pandemic: acute, intensive care unit (ICU), and general wards for patients with and without COVID-19, was reviewed.
Acute and intensive care unit rehabilitation.
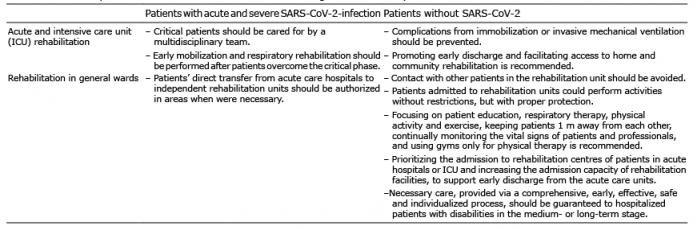
Patients with acute and severe COVID-19. Scientific and professional rehabilitation organizations recommended ensuring rehabilitation for patients recovering from COVID-19, in order to prevent complications of acute conditions and comorbidities throughout the entire pandemic period. The transfer of patients with disabilities to acute care hospitals and ICUs if the health situation or a COVID-19 infection requires it was also stated as a priority (10). Different associations, such as World Confederation for Physical Therapy (WCPT), Association of Chartered Physiotherapists in Respiratory Care (ACPRC), Canadian Physiotherapy Association (CPA), Chartered Society of Physiotherapy (CSP) and others, published manuals, protocols, and recommendations for the care of patients with COVID-19 infection. They suggested that critical patients should be cared for by a multidisciplinary team, which includes different rehabilitation professionals. They also offered recommendations for early mobilization and respiratory rehabilitation to promote spontaneous breathing and functional recovery after patients had overcome the critical phase (11). One guideline from the CSP focused on the acute pulmonary rehabilitation of patients with COVID-19 in ICUs (12). Prevention interventions, therapeutic strategies and recommendations were proposed for patients with COVID-19 in the acute pulmonary rehabilitation phase, and CSP have committed to developing guidelines to describe the rehabilitation of patients with COVID-19, from the ICU to the community setting (12).
The guideline “Physiotherapy management for COVID-19 in the acute hospital setting” included recommendations for physiotherapy workforce planning management for COVID-19 in the acute hospital setting, and a screening tool for determining the requirement for physiotherapy (11). The Chinese Society of Rehabilitation Medicine (CSRM) recommended assessing patients from admission to ICU, identifying severe manifestations, and allowing immediate implementation of supportive treatments (13). The safety criteria for early mobilization and the prescription of activities in patients with COVID-19 in the ICU and physiotherapeutic interventions for patients with suspected or confirmed diagnosis of COVID-19 in the ICU were presented (14).
The article “Early Rehabilitation in COVID-19, best practice recommendations for the early rehabilitation of COVID-19 patients” included conceptual suggestions for early rehabilitation of patients with COVID-19, such as a checklist of logistical and organizational preparations, aspects of infectivity and personal protective equipment (PPE), adjustments to the patients’ surroundings, interprofessional teamwork and co-therapy, respiratory therapy, mobilization, activating care, training in activities of daily living (ADL), training intensity, and psychosocial management (15).
Patients without COVID-19. Patients without COVID- 19 infection who required ICU should be treated according to the protocols that each centre had developed for ICU rehabilitation. Italian Society of Physical Medicine and Rehabilitation (SIMFER) recommended preventing complications from immobilization or invasive mechanical ventilation. Clinical stability must be achieved, and rehabilitation interventions planned. Promoting early discharge and facilitating access to home and community rehabilitation is recommended whenever possible, especially for patients with adequate functionality (16).
Rehabilitation in general wards.
Patients with COVID-19. Latin American Medical Association of Rehabilitation (AMLAR) stated that rehabilitation centres converted their inpatient rehabilitation units into dedicated COVID-19 recovery units and explicitly authorized direct transfer of patients from acute care hospitals to independent rehabilitation units in areas when were necessary (17).
Patients without COVID-19. One of the main recommendations of American Academy of Physical Medicine and Rehabilitation (AAPMR) was for patients without COVID-19 to avoid contact with other users in the rehabilitation unit (17). Some associations stated that patients without COVID-19 infection who were admitted to rehabilitation units could perform activities without restrictions, but with protection, such as using a surgical mask or face covering from home, with patients performing supervised handwashing at the entrance and exit, safe distancing, and temperature checks at the entrance of the rehabilitation unit. They recommended focusing on patient education, respiratory therapy, physical activity and exercise, maintaining 1-m social distancing between patients, continually monitoring the vital signs of patients and professionals, and using gyms only for physical therapy (18).
SIMFER also recommended prioritizing the admission to rehabilitation centres of patients in acute hospitals or ICU, and increasing the admission capacity of rehabilitation facilities, to support early discharge from the acute care units (16). Other organizations planned the relevance of admitting patients with rehabilitation needs to rehabilitation units and hospitals, and reconsidered intensive therapies lasting 3–4 h during the public health emergency (10).
CPA willingly offered the availability of therapists to support respiratory therapy, preparation for discharge and early rehabilitation of people with neurological conditions and post-traumatic injuries. Other organizations proposed resources and measures regarding physiotherapists in hospital settings to continue to work with proper protection measures (19).
Moreover, AAPMR exposed that necessary care, through provision of a comprehensive, early, effective, safe and individualized process, should be guaranteed to hospitalized patients with disabilities in the medium- or long-term stage. Furthermore, assessment, treatment and telematic support from rehabilitation services are suggested (17). Table I shows the main adaptations in ICU rehabilitation services during the COVID-19 pandemic.
Adequacy of outpatient services
Recommendations regarding the adequacy of outpatient services: post-acute services and long-term community rehabilitation services for patients with and without COVID-19, were reviewed.
Post-acute services. AAPMR recommended restricting face-to-face care for high-risk users. All outpatient procedures were suspended for those patients with respiratory symptoms, immunocompromised patients, older patients, or those in contact with children or older people, those who had recently travelled outside their countries or had been in contact with a person who had travelled abroad (20). For patients receiving outpatient care or who did not have an urgent medical condition, SIMFER recommended immediate transition to virtual medical appointments through remote consultation or telerehabilitation was recommended (16).
Spanish Society of Rehabilitation and Physical Medicine (SERMEF) recommended that first-time outpatient consultations and patients with complex pathologies should be prioritized. Regarding rehabilitation in day hospitals, there were no specific recommendations. Furthermore, SERMEF recommended assessing the risk–benefit individually and postponing treatment in patients over 65 years of age, and those with comorbidities, immunosuppression or cardiorespiratory disease. However, assistance for patients with pathologies such as acute neurological damage, rehabilitation after recent surgery, acute musculoskeletal rehabilitation with a high risk of sequelae or any pathology derived from COVID-19 infection, was considered urgent (21).
In maintaining outpatient services for some patients with face-to-face rehabilitation needs, Colombian Association of Physiotherapy (ASCOFI) recommended patients attend rehabilitation institutions together with only one companion. They must remain in the waiting rooms according to established protocols. Furthermore, hospitals must schedule agendas to limit patient encounters, have staff cleaning contact surfaces regularly, not admit patients without prior appointment, and not allow companions in therapies except for patients who are minors or with significant dependence (22). Some guidelines and webinars, especially those from SERMEF, offered information about the reopening of outpatient services along with modifications in the physical structure, protective barriers, use of PPE in the outpatient setting, such as using a surgical or face covering from home, supervising the patient’s handwashing at the entrance and exit, disinfecting footwear, safety distancing, and temperature checks at the entrance to the rehabilitation unit, reorganization of waiting rooms and recommendations about how to handle the COVID-19 crisis in the outpatient rehabilitation setting, including hydrotherapy services (21, 23).
Table I. Main adaptations to ICU rehabilitation services during the COVID-19 pandemic
Long-term and community services.
Outpatient and home rehabilitation services should ensure the care of people in need of interventions to minimize functional deficits and prevent long-term disability (17).
Home-based and community-based rehabilitation can be delivered through different strategies, such as telerehabilitation or direct care. Rehabilitation at home or in the community is recommended by Ghana Physiotherapy Association (GPA) in priority cases, assessing the patient’s environment regarding the health conditions of family members and establishing strict protocols for patients with or without COVID-19 (24).
Telerehabilitation services are an innovative strategy that have been widely recommended and supported by several scientific associations. Most associations supported and encouraged the modification of service provision to this modality, whenever possible. For example, patients should not be offered telerehabilitation consultations in some cases, such as: if they are in hospital and require physiotherapy; if there is a risk of serious deterioration from underlying pathology; if they have urgent rehabilitation needs, such as acute neurological damage, rehabilitation after recent surgery, acute musculoskeletal rehabilitation with high risk of sequelae, or any pathology derived from COVID-19 infection that is considered urgent (21, 25).
Teleconsultation must be provided by rehabilitation professionals. It should be prioritized, facilitate communication, and provide information and advice to people with disabilities of different origins and their families or caregivers (26). Associations resolved frequent questions regarding telerehabilitation on their websites (27).
Some therapy associations, such as the CSP, stated that virtually informed consent, patient safety, and consultation privacy are necessary for the telerehabilitation process through videos, telephone, email, and mobile messaging (28). When the pandemic is over, some associations will probably continue using telerehabilitation programmes. Furthermore, there are some training courses and guidelines about the benefits of the use of digital tools to deliver telerehabilitation (26).
A survey, carried out in Colombia, revealed that 90% of patients and medical staff considered that virtual physiotherapy should be included in physiotherapy’s practical training and should be part of primary care. Moreover, virtual physiotherapy allows the development of competencies for counselling-consulting-orientation of caregivers and patients and will enable patients’ follow-up after discharge from hospital care (29).
Rehabilitation care for patients with COVID-19. Different associations recommended home-based rehabilitation programmes to avoid deconditioning, offering information about pulmonary rehabilitation at home for people with COVID-19 (30). CSP stated that community rehabilitation teams must be resourced and staffed sufficiently to meet the existing demand, as well as the additional need of people recovering from COVID-19 who are returning home or to a care home. It is estimated that 45% of people admitted to hospital with COVID-19 need some form of ongoing health and care services on discharge, which includes rehabilitation. These services already face significant disruption due to the redistribution of the workforce, social distancing and shielding requirements (25).
American Physical Therapy Association (APTA) also stated that patients with COVID-19 who are discharged from hospitals should transfer their care to community rehabilitation teams. Some people with COVID-19 were not admitted to hospital, but required physiotherapy support through community services. Furthermore, some associations stated that community rehabilitation teams must have sufficient resources and meet the additional needs of people recovering from COVID-19 when returning home. Thus, web conferences were delivered focused on helping therapy staff to promote community rehabilitation in recovery from COVID-19 (30).
It is recommended that outpatients with COVID-19 should be followed up by a rehabilitation team (17). In case of a suspected or confirmed case of COVID-19, hospital therapies must be suspended, primary care personnel must report the situation, and they (the patient and personnel who attended the patient) should complete 14 days of isolation at home (31).
Finally, associations warned about the consequences of COVID-19 and recommended learning about outpatient rehabilitation interventions in patients with COVID-19 and post-intensive care syndrome (PICS) (30). Table II shows the main adaptations in outpatient and long-term rehabilitation services during the COVID-19 pandemic.
Recommendations to prevent the spread of COVID-19 in rehabilitation care
ACMFR recommended that, in order to avoid crowds in the institutions, all group meetings should be suspended, and only 1 person should use cafeteria spaces at a time. They recommended that all people entering the hospitals undergo rapid assessment to detect COVID-19 symptoms and, in the event of positive findings, the case is reported. The rapid assessment consists of enquiring if the patient has respiratory symptoms or fever, if the patient travelled abroad in the last 20 days, or if they had had contact with suspected or confirmed cases of COVID-19 infection. Furthermore, cleaning and disinfection every 2 h were recommended, and that a protocol for waste management and disposal should be set out (22). During the COVID-19 pandemic, the rehabilitation care system will be responsible for assessing and managing individuals with suspected or confirmed COVID-19, while continuing to provide services for urgent non-COVID-19 healthcare needs. Hence, comprehensive infection prevention and control programmes are essential in every setting where healthcare is provided. They will help ensure that effective processes and activities are in place to prevent or minimize the transmission of COVID-19 within the organization (30).
Table II. Main adaptations to outpatient and long-term rehabilitation services during the COVID-19 pandemic
Associations therefore developed biosecurity protocols for rehabilitation professionals and patients and highlighted prevention measures to mitigate COVID-19, through guidelines and educational resources (25, 31). The most general recommendation was to use PPE for patients, caregivers and personnel who provide healthcare in COVID-19 and not-COVID-19 settings. Associations offered training and guidelines to ensure education on the use, application, and removal of PPE. In addition, associations promoted appropriate hand hygiene with soap and water for at least 20 s, especially after contact with the ill person and after removing gloves, masks and eye protection and drying the hands with disposable paper towels, or cleaning the hands with a wet wipe and then using an alcohol-based hand sanitizer (11). Table III shows the main strategies to ensure the correct use and availability of PPE during the COVID-19 pandemic.
Table III. Main strategies to ensure the correct use and availability of personal protective equipment (PPE) during the COVID-19 pandemic
Furthermore, CSP highlighted other measures to reduce the spread of COVID-19, such as providing individual care, assessing COVID-19 symptoms to determine the possibility of infection, adopting specific actions to perform therapies, social and physical distancing measures, cleaning equipment and devices between each patient interaction, taking the temperature of patients, and recommending taking precautions when collecting patient samples (32). Also, they stated that people at higher risk from COVID-19, such as older adults and populations with chronic medical conditions, immunocompromised patients or those with obesity should be protected through measures such as: keeping away from people who are sick; leaving home only for medically necessary appointments; avoiding contact with people who have travelled or been exposed to the virus; cleaning hands frequently; avoiding touching the mouth, nose, and eyes and/or food with hands; avoiding touching high-touch surfaces; avoiding crowds and large gatherings; and, if they develop symptoms, staying at home and calling a healthcare provider or local public health unit (25).
ASCOFI developed infection prevention and control guidance and strategies to prevent or limit COVID-19 transmission in healthcare settings, including acute care, long-term care, homecare and outpatient and ambulatory care (21).
For all confirmed or suspected cases of COVID-19, droplet precautions should be implemented, at a minimum it is recommended that staff must wear a surgical mask, fluid-resistant long-sleeved gown, goggles or face shield, and gloves. Furthermore, recommended PPE for staff caring for COVID-19-infected patients includes added precautions for patients with significant respiratory illness, when aerosol-generating procedures and/or prolonged or very close contact with the patient are likely. In these cases, it is recommended to take precautions against airborne spread, such as wearing a N95/P2 mask, fluid-resistant long-sleeved gown, goggles or face shield, and gloves. The patients will also be placed in isolation. Hospitals were often able to contain patients with a risk of droplet or airborne spread within dedicated isolation rooms.
They stated that the use of equipment should be carefully considered and discussed with local infection monitoring and prevention service staff before use with patients with COVID-19, to ensure that it can be properly decontaminated. In the case of equipment, it could be used for a single patient, ensuring that machines can be decontaminated after use. Larger equipment (e.g. mobility aids, ergometers, chairs, tilt tables) must be easily decontaminated (11).
In addition, Australian Physiotherapy Association (APA) showed an overview of telehealth and telerehabilitation through web seminars, and highlighted the role of telemedicine in flattening the COVID-19 curve. Therefore, they suggested reducing the barriers to access to teleconsultation (26).
Regulatory standards and positions during the COVID-19 pandemic for protecting health workers and patients’ rights.
Scientific and professional rehabilitation organizations raised concerns related to the breaching of health professionals and patient’s rights. Therefore, they called on the authorities to establish and implement measures to address the needs of rehabilitation professionals and patients.
The American Medical Rehabilitation Providers Association (AMRPA) and the AAPMR associations urged the authorities to guarantee the safety of professionals and patients, to secure equitable availability of COVID-19 testing, increase hospital capacity and other necessary services, ensure access to essential medicines, expand telerehabilitation coverage, reserve funding to pay for COVID-19 treatments for those patients who are not covered by the health system (24, 33).
Finally, rehabilitation associations called for additional regulatory measures by the authorities to help rehabilitation hospitals and centres overcome financial risks. Therefore, they requested increased financial aid for rehabilitation hospitals/centres. Moreover, support was requested for professionals, through tax deductions, interest-free loans, direct payments, and virtual visits (34).
This study describes the timely innovative proposals of scientific associations and rehabilitation professionals, focusing on delivering rehabilitation services, protection and prevention measures, physical distancing, isolation, hand washing, and disinfection measures, based on the recommendations of supranational organizations, such as the WHO.
During the COVID-19 pandemic, rehabilitation services have been downgraded to priority interventions. The COVID-19 emergency is having a huge impact on the rehabilitation of people experiencing disability, which may lead to future cumulative effects due to reduced functional outcomes and, consequently, increased burden of care (35). A devastating consequence of the impact of the pandemic on the delivery of rehabilitation services would be the decreased participation of persons with disabilities in society (8). There will also be an additional group of patients with rehabilitation needs due to the consequences of COVID-19 on respiratory, cardiovascular, neurological and mental functions. Thus, there is concern about reconstituting rehabilitation services appropriately when the pandemic ends (8).
These findings suggest that some care of patients with rehabilitation needs has been postponed in hospital settings, due to prioritizing people with moderate and severe COVID-19. A survey, carried out in 35 countries, including 99% of the European population, found that hospital admissions were stopped and 48% of inpatients with rehabilitation needs were discharged early. Outpatient services were stopped completely in 83% of countries, comprising 87% of the European population (4).
Scientific and professional rehabilitation organizations published timely recommendations regarding continuity of care of patients with or without COVID-19 in different settings, such as acute care, ICUs, and general wards. Moreover, it was recommended that institutional outpatient care be individualized in each case, assessing patients’ risk-benefit and postponing interventions for people with high-risk factors. Some organizations proposed already established strategies, such as home-based rehabilitation and community-based rehabilitation. Furthermore, other methods were developed and maximized, such as teleconsultation through videos, telephone, email, and mobile messaging. Telerehabilitation was implemented to offer synchronous therapeutic interventions, strengthen educational programmes, and preserve adherence to rehabilitation programmes. The safety and efficacy of telehealth has been demonstrated clearly across a wide range of clinical areas, including cardiac rehabilitation, neurological rehabilitation (brain injury, multiple sclerosis, traumatic brain injury), persistent pain, chronic obstructive pulmonary disease (COPD), hip and knee arthroplasty, tendinopathy, and pelvic floor muscle training (26).
Rehabilitation services must be equipped with PPE and follow strict hygiene measures. In particular, rehabilitation must be accessible to vulnerable populations. Hence, rehabilitation services, which range from acute or subacute phases to long-term phases, must remain a health priority during the COVID-19 pandemic and be financed adequately (8, 36).
The implemented strategies have not yet been proven, and it is necessary to evaluate their effectiveness and acceptance by users. Rehabilitation interventions were established for patients with COVID-19, and it is expected that a range of studies will provide information about the safest and most effective rehabilitation strategies.
Different countries, such as Germany, Italy and Spain, state that we must assume that the COVID-19 pandemic raises new challenges in acute care rehabilitation care, outpatient and long-term care. Acute care rehabilitation needs to be provided for patients with COVID-19, combining the existing acute care rehabilitation experience for patients with respiratory infections with currently available sources and experience (15).
The Global Rehabilitation Alliance stated that rehabilitation is an integral part of managing COVID-19-related health problems. Rehabilitation should be provided, from acute to long-term rehabilitation care, during and after COVID-19 infection, and for people experiencing disabilities. Rehabilitation care should involve vulnerable populations, such as older people, those with disabilities, and people living in poverty. It is necessary to improve access to rehabilitation for people with disabilities and other vulnerable populations with COVID-19 who live in low- and middle-income countries (8).
Study limitations
This review has several limitations. First, the heterogeneous indexation of information in the rehabilitation organizations web portals made the task of searching and identifying key documents difficult. Therefore, it is possible that relevant information issued by some scientific and professional rehabilitation organizations has not been included. Secondly, there is a scant evidence base regarding the impact of adaptations of rehabilitation services, because no studies on long-term outcomes are yet available. Thirdly, at the time this review was performed, the organizations did not focus on access to COVID-19 vaccination for professionals and patients. Finally, it is necessary to collect data about the care of people with disabilities in low- and middle-income countries, where there is a lack of adequate information systems about people with disabilities.
Critical patients with SARS-CoV-2 infection should be cared for by a multidisciplinary team and provide early mobilization, respiratory, outpatient rehabilitation intervention and long-term care. For patients with and without SARS-CoV-2, home- and community-based rehabilitation can be delivered through different strategies, such as telerehabilitation or in-person care. The use of measures to prevent and protect against transmission of COVID-19 are necessary for all patients in rehabilitation care.


 Click to show fullsize
Click to show fullsize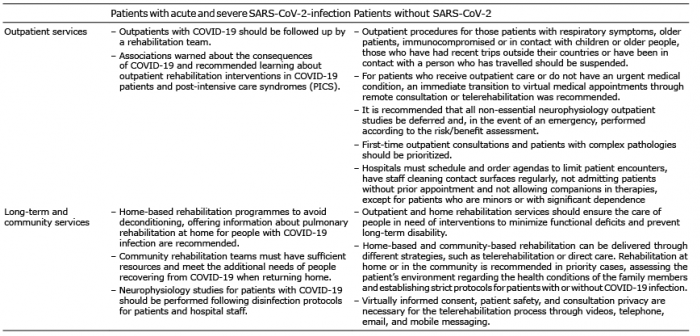 Click to show fullsize
Click to show fullsize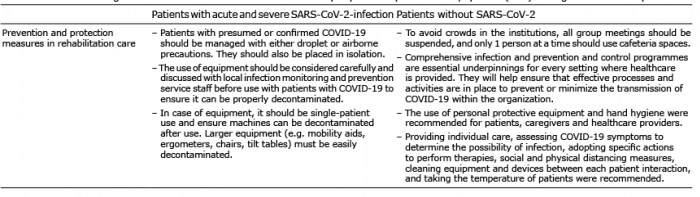 Click to show fullsize
Click to show fullsize