
From the 1Spinalis Foundation, 2Karolinska Institute, Stockholm, 3Department of Rehabilitation/CHILD Research Centre, School of Health and Welfare, Jönköping University, Jönköping,Sweden, 4Research Therapist, Royal Free Hospital and College of Health, Medicine & Life Sciences, Brunel University London, UK and 5Department of Rehabilitation, Jönköping Academy, Aging Research Network-Jönköping (ARN-J), Jönköping University, School of Health and Welfare, Jönköping, Sweden
Background and objective: Individuals with spina bifida often have cognitive impairments leading to difficulties in education and daily activities. The aims of this study were to explore cognitive impairments in adults with spina bifida and to consider associations between impairments, educational outcome and performance of daily activities, comparing individuals with and without intellectual disability.
Methods: Data were collected on 35 adults with spina bifida via cognitive tests and Assessment of Motor and Process Skills (AMPS). Participants were divided into 3 groups: individuals without intellectual disability who completed compulsory education (NID-C); those without intellectual disability, who failed to successfully pass compulsory education (NID-F); and those with intellectual disability failed to successfully pass compulsory education (ID-F).
Results: All individuals with intellectual disability failed to successfully pass compulsory education (group ID-F) and had poorer scores across almost all measures than group NID-F and significantly poorer scores than group NID-C. All except 6 individuals scored below cut-off levels for effort and safety on both AMPS motor and process scales; more significant associations were seen between the cognitive tests and the motor rather than process scale.
Conclusion: Cognitive impairments, irrespective of intellectual disability, impact on the performance of everyday activities and on educational achievement, and thus need to be considered in assessments and interventions to improve outcomes and promote independence in people with spina bifida.
Key words: disability evaluation; intellectual disability; cognitive function; activities of daily living; spina bifida.
Accepted Aug 14, 2021; Epub ahead of print Aug 26 2021
J Rehabil Med 2021; 53: jrm00225
Correspondence address: Dorothee Riedel, Spinalis Foundation, Stockholm, Frösundaviks allé 4A, 169 70 Solna, Sweden. E-mail: dorothee@spinalis.se
Doi: 10.2340/16501977-2868
Individuals with spina bifida often have cognitive impairments, resulting in difficulties in performing their everyday life activities at home, in education, training and social life. These difficulties are often not recognized, and the individuals do not receive the support they need from society. This study investigated the relationship between cognitive impairments, school achievements and performance of daily life activities of 35 adults with spina bifida. The study examined whether individuals had an intellectual disability, and whether they had completed compulsory education, and compared this with their cognitive function and performance in everyday activities. The results confirm that individuals with cognitive impairments, even those without intellectual disabilities, often have considerable difficulties in school achievements, and performance of daily life activities, reducing their ability to live independently.
Spina bifida (SB) is caused by the incomplete closing of the embryonic neural tube, which can affect brain development, with consequent sensory and motor difficulties (1, 2). Hydrocephalus is present at birth in 80–85% of individuals with SB (3), and by adulthood 63% are estimated to have hydrocephalus (4). Hydrocephalus leads to structural anomalies in the brain (1), which seem to contribute to a cognitive phenotype with relative strengths and weaknesses (5) and differing degrees of cognitive impairments amongst individuals with SB (6). One in 5 individuals with SB and hydrocephalus are reported to have an intellectual disability (ID) (intelligence quotient (IQ) < 70) (7). Furthermore, according to several studies many other individuals with SB show impaired executive functions (EF)1, which become more evident when performing more complex activities (5). Impaired working memory (9), a part of EF (8), and prospective memory (10) are also common, as well as attention disorders (11), impaired processing speed, timing deficits (5), problems with time management (12) and with getting things done (13). Impaired visuospatial function is also common (11). In general, individuals with SB have no limitations in reading, vocabulary, grammar, and sentence structure, but may have difficulties in understanding the underlying meaning of words and in drawing conclusions (5). Reduced reading comprehension and reduced numeracy are also common (5). Learning capacity is often unaffected, but individuals may have difficulties in processing and retrieving information (5). These cognitive impairments can be observed in childhood and become more evident during adolescence and adulthood, when activities of daily living (especially taking care of your own household), education, work and relations put increased demands on the person (14). Several studies found that cognitive impairments in individuals with SB do not decrease with maturity, but persist into adulthood (9, 14). Furthermore, impairments in prospective memory have also been shown to increase for persons over 32 years of age (10). Few studies have examined the effects of ageing on cognitive function in individuals with SB (9).
1Executive functions (EF): cognitive processes involved in achieving goal-directed behaviours (8)
Cognitive impairments are associated with quality of life (15) and affect performance of daily activities negatively for adults with SB (16), with potential impact on health and wellbeing (4, 17). Impaired EF may limit young adults in achieving milestones of independence in life, like education, work, relationships and assuming responsibility for their own household (18). Many individuals with SB do not reach secondary education and have difficulties in obtaining a job (19). Further challenges may appear in adulthood with the need to manage contacts with authorities regarding special transportation services, housing, and community-based support services, etc. (20). Moreover, management of personal hygiene and medication due to complex SB-related disabilities put additional demands on EF (20). Consequently, impaired EF increases risks for complications, such as pressure ulcers, urinary infections, incontinence, and constipation (21). However, individuals with SB are often highly verbal, giving the impression of managing everyday life well (22). Thus, healthcare professionals and others not specialized in the field seldom recognize these cognitive limitations (23). The need for support may go unrecognized, and interventions may be insufficient or even fail (24).
In order to provide appropriate support, there is a need for assessments to recognize the range of cognitive impairments in individuals with SB and to consider how these impact on educational outcomes (completion of compulsory education2) and performance of daily activities (especially household activities). The aims of the current study were to explore cognitive impairments in adults with SB and to consider associations between these impairments, educational outcome, and performance of daily activities, comparing individuals with and without intellectual disabilities (ID).
2In Sweden compulsory education certificates are usually obtained at age 16 years after 9 years of school.
A cohort study was performed to examine profiles of performance across clinical tests of cognitive function and daily skills. The study was approved by the Regional Ethical Review Board in Stockholm (registration number 2012/1836-31/2) and fully informed written consent was obtained from participants.
Participants
Participants were recruited from 2 groups. One group were young adults with SB who were invited to participate upon enrolment at the rehabilitation centre (”on enrolment”; OE group), resulting in 15 participants, age range 18–26 years. To increase the overall sample size data were also collected from client records (”client records”; CR group) from 20 individuals from the same rehabilitation centre (age range 22–45 years), who had been assessed using the Assessment of Motor and Process Skills (AMPS) and the cognitive tests chosen for the current study within the previous 5 years. Demographic information was collected at assessment or from records. Individuals would have been diagnosed with an ID by a neuropsychologist following referral and this diagnosis registered in the young person’s records. Educational history was recorded as the highest level of education completion evidenced by certification or self-report.
The participants were divided into 3 groups: individuals without ID who completed compulsory education (NID-C);those without ID who failed to successfully pass compulsory education (NID-F); and those with ID who failed to successfully pass compulsory education (ID-F).
Assessment instruments
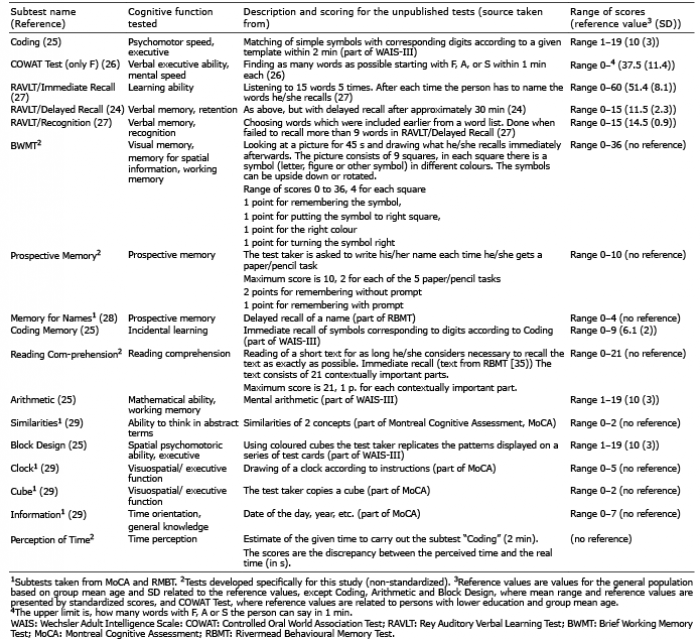
The 17 subtests used for the purpose of this study are outlined in Table I. Subtests were selected that, according to the literature, assess cognitive impairments common in individuals with SB (5, 6). Eight of the subtests were taken from standardized assessments: Coding, Coding Memory, Arithmetic and Block Design from the Wechsler Adult Intelligent Test (WAIS-III) (25), the Controlled Oral World Association Test (COWAT), and the 3 parts of the Rey Auditory Verbal Learning Test (RAVLT). These subtests have been tested for reliability and validity with normative values available (considered here as reference group values) (26, 27). Four subtests were taken from the Montreal Cognitive Assessment (MoCA) (Similarities, Clock, Cube, and Information) and 1 subtest was taken from the Rivermead Behavioural Memory Test (RBMT). The MoCA and the RBMT have been tested for reliability and, validity as a whole (28, 29), but no separate normative values are available for parts of the tests. No suitable existing tests were found for visuospatial working memory, prospective memory, reading comprehension and time perception. As more clinical information was required about these functions, 4 further tests were developed by the second author: the Brief Working Memory Test (BWMT) (currently under development and used clinically in a specialist clinical setting), Prospective Memory, Reading Comprehension, and Perception of Time (developed for this study). These tests do not have reference values for the general population and have not been tested for reliability and validity. It took approximately 1 h to perform the battery of cognitive tests.
Table I. Description of the used cognitive tests and scoring of the unpublished tests
The AMPS was chosen as a standardized assessment of daily life performance of an individual regarding effort, efficiciency, saftey and independence. AMPS is a client-centred observation-based performance assessment used by occupational therapists. The AMPS measures the quality of performance of ADL tasks on 2 scales (motor and process) without testing for any underlying cognitive impairments (30). Cognitive function can partly explain the performance of daily activities measured with the AMPS in individuals with stroke (31), Alzheimer’s disease (32), and dementia (33). The AMPS is designed to be performed at home or in a clinical setting, has established intra- and inter-rater reliability (34) and is validated for use in Sweden (35). The client chooses and performs 2 or more ADL tasks that are relevant and familiar to him/her (30). During these activities, an occupational therapist, trained and certified in AMPS, observes and evaluates the quality of performance of 16 motor skills (e.g. paces, positions, walks, coordinates, transports) and 20 process skills (e.g. attends, chooses, initiates, organizes), using a 4-point ordinal scale (30). AMPS software using Rasch analysis converts the raw data into a logit scaled score on 2 univariate measures of individual performance: ADL motor ability (i.e. degree of physical effort) and ADL process ability (i.e. degree of efficiency). Their respective cut-off levels (2.0 for motor ability, 1.00 for process ability) indicate whether an individual may need assistance to function in the community. The Rasch weighting allows for generalization of results across different ADL-tasks of similar challenge (30). No studies have examined relationships between cognitive function and performance of daily activities measured by the AMPS among adults with SB.
Data collection
Data were collected on 2 different occasions for each participant. Nineteen participants were first assessed with the cognitive tests, and 16 participants were first assessed using the AMPS. The cognitive tests and 5 AMPS assessments were performed at the rehabilitation centre; the remaining 30 AMPS assessments were conducted in participants’ homes. The time difference between the 2 assessment occasions varied; 19 individuals performed both assessments within 1 year, the remaining individuals within 3–5 years (see data analysis section below). In the rehabilitation centre, the AMPS is used clinically for an ADL ability assessment, which individuals require when applying for personal assistance or home help services. In the CR group the cognitive tests were carried out as part of a larger multidisciplinary study, the OE group was tested on enrolment at the rehabilitation centre.
Data analysis
SPSS version 25 (2017) was used for analysis. Three groups of participants were identified based on information on ID and level of school achievement. Descriptive statistics described independent living abilities and explored the results of all the subtests for the whole group and groupwise for the 3 identified groups. Inferential statistics were run on the items from standardized tests with reference values and for the subtests taken from MoCA and RBMT. To identify any differences in performance between OE and CR groups and between the group with a short vs long time gap between the assessments, t-tests were performed for parametric data and Mann–Whitney U for non-parametric data. There were no differences in mean scores on any scale between methods of recruitment or time gaps in testing, nor between younger and older participants; thus, all the data were combined for comparisons. The normality of distributions was checked with Shapiro–Wilks test. Analysis of variance (ANOVA) was used to contrast performance on parametric data, and Kruskal–Wallis analysis of variance was used to contrast performance on the remainder of the cognitive tests and the AMPS. Where age was found to have a significant effect, age-adjusted scores are reported. Post hoc comparisons of between-group differences using Hochberg (for small samples, equal variance) or pairwise comparisons of mean differences were performed for parametric and non-parametric analyses, respectively. False discovery rate (FDR) (36) was used to correct for multiple comparisons to minimize risk of type I error (false-positive findings) for the comparisons of cognitive tests included in inferential data analyses. FDR was considered appropriate in order to localize error rates between tests and rank both parametric and non-parametric results. Alpha was set at 0.05. Correlations between the standardized cognitive tests and the AMPS were calculated with Pearson’s partial correlations controlling for time between testing, in days3.
3No differences were found between Pearson’s and Spearman’s correlation for non-parametric data; therefore, Pearson’s partial correlations are reported for all comparisons.
None of the 9 individuals with identified ID completed compulsory education (ID-F), a further 11 individuals without identified ID also failed to successfully pass compulsory education (NID-F). The remaining 15 individuals had no identified ID and completed compulsory education (NID-C). The results of the 3 groups were compared to consider the impact of potential cognitive deficits, as distinct from more pervasive learning difficulties associated with ID.
The 3 groups did not differ in age (F (2,32)=0.750, p = 0.181) or sex distribution. Most individuals from group ID-F lived with their parents (5/9) or in a sheltered home (2/9). Approximately half of the individuals in group NID-F (6/11) and group NID-C (6/15) lived in their own households by themselves. Only 4 participants, all from group NID-C, managed their everyday life without support. All other individuals received help for their personal care and/or household work. Twenty participants (57%) also needed help with reminders to perform their personal care (8/9 in group ID-F, 4/11 in group NID-F and 5/15 in group NID-C). Almost all individuals in group ID-F (8/9) and approximately half of the individuals in group NID-F (5/11) needed help with their personal finances. The majority of group NID-C (12/15) managed their finances independently. More than one-third of the individuals who required help in any of the above-mentioned activities (11/31) received assistance, mainly from their parents. Very few individuals were employed: none from group ID-F, only 2 in group NID-F, and 4 in group NID-C.
Cognitive performance
Participants as a group had generally poor results across most cognitive tests compared with the general population (Table II); group ID-F differed most and group NID-C the least.
Table II. Participants’ (n = 35)c results across cognitive tests as whole group and by 3 learning ability subgroups
There were significant differences between the 3 groups for Coding (χ2 (2, n = 35) 15.41, p = 0.010), RAVLT Immediate Recall (F (2,32)= 5.68, p = 0.008), RAVLT Delayed Recall (F(2,32)= 4.02, p = 0.028), and Coding Memory (χ2 (2, n = 35) 15.41, p = 0.010), Arithmetic (χ2 (2, n = 35) 9.49, p = 0.009) and Block Design (χ2 (2, n = 35) 12.493, p = 0.002), with Coding, Arithmetic and Block Design remaining significant after FDR control. RAVLT Immediate and Delayed recall were just above threshold after FDR control. Post hoc comparisons showed the differences to be significant between group ID-F and group NID-C for Coding (mean difference –15.09 (95% CI –25.52 to –4.66), p = 0.003) and for Arithmetic (mean difference –3.38 (95% CI –1.27 to –6.49), p = 0.03). For Block Design significant differences were evident, both between group ID-F and group NID-F (mean difference –11.66 (95% CI –21.45 to –1.86), p = 0.016) and group ID-F and group NID-C (mean difference –10.91 (95% CI –20.10 to –1.73), p = 0.016). In the subtest RAVLT Recognition all 3 groups performed within reference values and there was no difference between the groups. The results of subtest COWAT showed that group NID-F and group NID-C performed within reference values (group NID-F slightly better than group NID-C): Group ID-F was only slightly below the reference value.
Among the subtests from MoCA and RBMT there was a significant difference between groups for the Cube (χ2 (2, n = 35) 8,37, p = 0.015), which remained significant after control for FDR. Post hoc analyses showed significant differences between group ID-F and group NID-C (mean difference –1.00 (95% CI –1.88 to –0.12, p = 0.023). There were no significant group differences for Clock, Memory for Names, Information and Similarities.
Activities of daily living
All participants had significantly poorer results on both AMPS motor and process scales than the general population of corresponding age (Table III). Significant differences were found between the 3 groups on both the motor (F(2,32) = 8.54, p = –0.001) and process scales (F(2,32) = 8.57, p = –0.001). Post hoc analyses showed significant differences between group ID-F and NID-C for AMPS motor scale (mean difference –0.69 (95% CI –1.1 to –0.3) p = 0.001); for AMPS process scale significant differences were evident between group ID-F and group NID-C (mean difference –0.60 (95% CI –1.0 to –0.2), p = 0.002) and group NID-F and group NID-C (mean difference –0.44 (95% CI –0.8 to –0.1), p = 0.016). All participants performed below the established AMPS motor scale cut-off of 2.0, with only 6 individuals (17%) above the process scale cut-off of 1.0 (5 from group NID-C and 1 from group NID-F).
Table III. Participants’ results for the Assessment of Motor and Process Skills (AMPS) motor and process scales as whole group and by 3 learning ability subgroups with reference values
Correlation between the cognitive tests and the Assessment of Motor and Process Skills
Both the AMPS motor and process ability correlated positively with the test for psychomotor speed Coding and with Block Design. In addition, the AMPS motor ability correlated positively with the test for mental speed COWAT Test, and the memory tests RAVLT/Immediate Recall and RAVLT/Delayed Recall (Table IV).
Table IV. Correlations between Assessment of Motor and Process Skills (AMPS) and Cognitive tests
The study aimed to explore cognitive impairments in adults with SB and considered associations between these impairments, educational outcome, and performance of daily activities. By distinguishing between individuals with and without known ID who had or had not completed compulsory education, the relationship between cognitive impairments and daily performance was explored in detail. Group NID-C performed best in both the cognitive tests and AMPS, as expected, followed by group NID-F and group ID-F; the latter differing most from reference values. Notably, even individuals who did not have a known ID and had completed compulsory education (group NID-C) performance within reference values low reference values in most of the cognitive tests, and even demonstrably poorer in activities of daily living. Since all the participants performed below the cut-off on the AMPS motor scale, and the majority (29/35) of the individuals performed below the cut-off in AMPS process scale, increased physical effort, inefficiencies, safety risks and need for assistance when performing ADL tasks are to be expected. In line with these findings, almost all individuals had considerable support from relatives and/or community-based support services to manage everyday life.
The results across the cognitive tests are consistent with previous studies showing problems in EF (6), working memory (9), processing speed (5), and visuospatial functions (11). The results of the included subtests developed by the second author also seemed to confirm known difficulties in working memory and visuospatial function prospective memory (8), time management (11), and reading comprehension (5). The same pattern of group differences as in the standardized tests appeared. The results also confirm previous findings (5), that individuals often have relatively unaffected learning capacity (within reference values in RAVLT Recognition), but difficulties in retrieving information (difficulties in RAVLT Delayed Recall). Surprisingly, almost all participants performed in line with reference values in COWAT Test for verbal EF and mental speed. Psychomotor components of processing speed, evident in tests involving written or motor responses, may be more affected than the mental functions, reflecting the relative verbal strengths seen in this group (5).
Overall, cognitive functioning, in particular EF, was associated with functional performance according to AMPS, irrespective of known ID. In a complex disability such as SB, taking care of one’s body is one of the factors putting high demands on EF (20). Thus, the high prevalence of medical complications, such as urinary tract infections, incontinence, and pressure sores, in adults with SB (16) could be explained by compromised EF. Understanding of the relationship between cognitive factors and performance of daily activities will be important in efforts to mitigate broader health impacts by, for example, community-based support services.
The performance of time-restricted subtests (Coding and Block Design) indicated that many participants could solve the task, but not under time constraint. Therefore, reduced psychomotor speed may exacerbate other cognitive functions and thereby also day to day performance. This was evidenced in the performance on the AMPS, as participants worked slowly and had problems with time management.
Processing speed and numeracy as well as reading comprehension were poorer in individuals who failed to successfully pass compulsory education. This may explain the failure of many individuals without ID to successfully pass compulsory education. The poor performance of the cognitive tests of individuals with ID who did not pass compulsory education may be attributed to known ID. Yet, performance below or within low reference values of many other items were also found in the 2 groups without known ID, suggesting prevalence of specific impairments in EF. Surprisingly, there were few differences in cognitive testing and daily performance (AMPS) between individuals without ID who had completed compulsory education and those who had not. This may, in part, be due to the small sample size and lack of power.
When comparing reference values from the general population with test results of the participants, AMPS motor ability differed considerably, possibly due to physical disabilities resulting from SB. It is also possible that the AMPS motor abilities, particularly places (objects), coordinates, calibrates and paces (own movements), are dependent on EF. Yet, the limited associations with the AMPS process scale are surprising and difficult to interpret. Habituated daily activities may put fewer demands on process skills, such as those of temporal processing (initiating, sequencing, continuing, and terminating tasks and activities). Consistent with previous studies (12), the AMPS indicated impaired initiative or difficulties in getting things done, through low scores in AMPS abilities, such as accommodates, notices/responds and initiates. On the other hand, it was difficult to assess initiative with the included subtests, since the participants had to follow instructions and did not have to take initiative of their own.
Some cognitive impairments identified by the cognitive tests, particularly abstract thinking, numeracy and working memory, did not show any correlation with occupational performance as measured by the AMPS. These skills are important for other activities than those assessed by the AMPS, such as working, studying, and managing personal finances (5). Impaired working memory becomes more evident in complex activities (6), such as education and work life, than in more habituated everyday activities, such as making a sandwich. Notably, almost half of the participants in the current study also had difficulties managing education, employment, and personal finances, which suggests a link between cognitive function and management of daily life in education and work.
The level of lesion appears to be of limited relevance in explaining the difficulties in managing personal care, since individuals with an acquired spinal cord injury at the same level as the study group require no assistance in their activities of daily living (37).
Taken together, the described cognitive difficulties seemed to be the reason, why most of the participants, including individuals without ID, needed reminders and considerable support in managing their personal care, education, household, and personal finances. They often remained dependent on parents, even those who had community-based support services. Therefore, early recognition of cognitive difficulties in individuals with SB, irrespective of ID, is important for interventions and adequate support in education and activities of daily living, in order to mitigate problems with health and wellbeing, promote independence, and thereby reduce the individual’s dependency on their parents. Here a cognitive screening instrument tailored for adults with SB could have an important function. Cognitive assessments need to be supplemented with, among other things, interviews, and observations (38) to obtain a comprehensive picture of the complex interaction between the person, the environment, and the activity (39).
Study limitations
Since the number of participants in this study was limited to 35, generalization of the results to all individuals with SB is not possible. In particular, the prevalence of hydrocephalus was higher among participants than in the adult SB-population in general, in which 63% have hydrocephalus (16) compared with 97% in the current study. Thus, the cognitive abilities in the study group might have been lower than in the adult SB-population in general. Furthermore, as the AMPS in the CR group was undertaken to obtain a certificate of need, it is possible that some responses may have been influenced by need to ”obtain” a higher level of support. As all participants in the current study, including those without ID, performed below the means of a reference group on almost all standardized tests, including the AMPS, similar problems may be present in a broader population of adults with SB. Another limitation is the lack of a specific subtest on attention, a known difficulty in the SB-population according to previous research (10). Furthermore, conclusions from the non-standardized subtests should be drawn with caution.
Furthermore, since the data were collected over a period of up to 5 years, these findings should be interpreted with caution. To control for this large observation period, the results at the item level for 2 groups were compared (small vs large time gap between assessments, and group OE vs group CR), but no significant differences were found. In addition, partial correlations were run between the cognitive tests and AMPS to control for gaps in time that did not change results. While evidence suggests that cognitive functions of children with SB persist into adulthood (13), larger studies are warranted to explore cognitive and occupational performance over time. The limited number of participants over the age of 32 years (n = 2) precluded further analyses, particularly with respect to prospective memory (9), warranting more research into ageing in SB.
Conclusion
These findings point to a wide range of cognitive impairments prevalent to a varying extent among adults with SB. The study highlights the impact of ID and cognitive function on educational achievement and performance of daily life activities in this group. Notably, even individuals without ID can have considerably reduced cognitive functions and may fail to complete compulsory education. The selected cognitive tests, to a large extent, describe cognitive impairments in this group and their associations with difficulties in performing everyday activities, albeit the small sample warrants caution in interpretation. More research is needed to identify the cognitive profiles of individuals with SB, taking into account ID as well as other cognitive deficits, for the purpose of developing individualized interventions to address limitations in school performance and activities of daily living.
The authors thank all the participants who contributed to this study; the Carolina Montgomery Foundation and the Spinalis Foundation for part funding the study; and the Spinalis Clinic at Rehab Station Stockholm (the rehabilitation centre where the study was performed) for supporting the study. The sponsors had no role in any aspect of the study or preparation of the manuscript and the decision to submit the article for publication.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize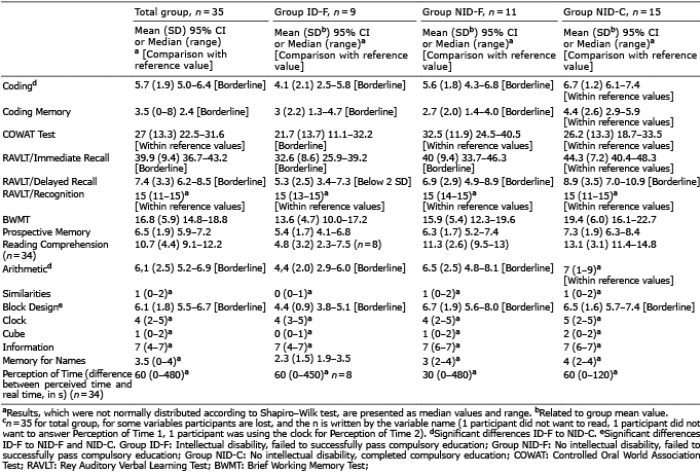 Click to show fullsize
Click to show fullsize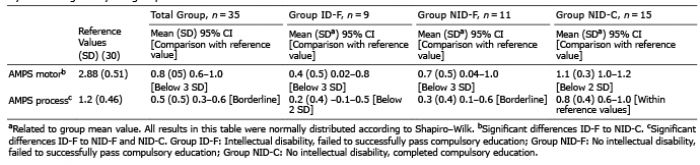 Click to show fullsize
Click to show fullsize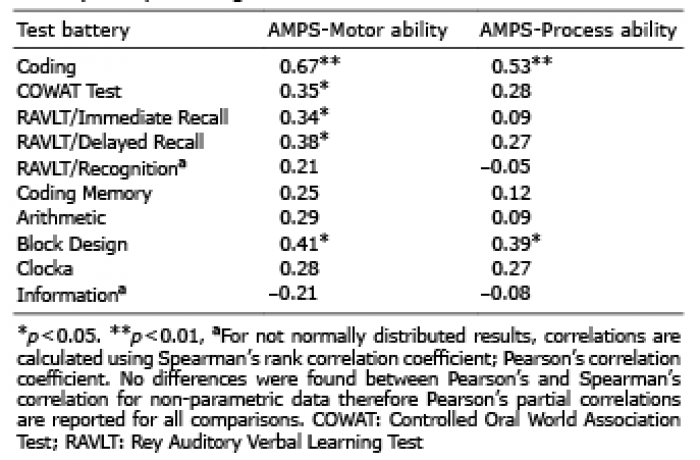 Click to show fullsize
Click to show fullsize