
From the 1Department of Rehabilitation, Université Laval, 2Centre for Interdisciplinary Research in Rehabilitation and Social Integration, Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale, Québec City, QC, Canada, 3Centre Mutualiste de Rééducation et de Réadaptation de Kerpape, Ploemeur and 4Université de Bordeaux - Handicap Activité Cognition Santé (EA 4136 HACS), Bordeaux, France
Objectives: To explore: (i) relationships between power wheelchair performance, confidence, mobility and the severity of user’s cognitive impairment; (ii) relationships between cognitive functioning and power wheelchair performance, confidence and mobility; and (iii) how cognitive scores influence power wheelchair performance, confidence and mobility.
Design: Cross-sectional exploratory study.
Subjects: Independent power wheelchair users; ≥18 years.
Outcome measures: Cognitive assessments (Montreal Cognitive Assessment, Motor-Free Visual Perception Test, and Dysexecutive Questionnaire) and power wheelchair driving assessments (Power mobility Indoor Driving Assessment, Wheelchair-Skills-Test-Questionnaire, and Life-Space Assessment). Analyses were completed using multivariate analysis of variance and principal component analysis.
Results: There were a total of 30 participants (with a mean (SD) age of 58 (15) years, who had a mean (SD) of 3 (6.2) years of experience of power wheelchair use, and a mean (SD) score of 22 (5) on the Montreal Cognitive Assessment. There were statistically significant differences in all power wheelchair driving assessments, depending on the severity of cognitive impairment (moderate, p = 0.009; mild, p = <0.001; none, p = 0.009). The first principal component suggested that cognitive functioning, visual perception, and performance explained 69% of the variability in the first principle componenent. The second and third principal components suggested that confidence and the built and social environments also played significant roles in power wheelchair use.
Conclusion: There are correlations between cognitive functioning and power wheelchair use in experienced users, with the severity of cognitive impairment influencing power wheelchair driving outcomes.
Key words: wheelchair; cognition disorders; self-efficacy; mobility limitation; power wheelchair.
Accepted Aug 14, 2021; Epub ahead of print Aug 27, 2021
J Rehabil Med 2021; 53: jrm00226
Correspondence address: François Routhier, Centre intégré universitaire de santé et de services sociaux de la Capitale-Nationale, 525, boul. Wilfrid-Hamel, Quebec City, Canada. E-mail address: Francois.Routhier@rea.ulaval.ca
Doi: 10.2340/16501977-2869
Clinicians report cognitive impairment as a concern when providing power wheelchairs. This study explored differ-ences in power wheelchair use (performance, confidence and mobility) between users with different levels of cognitive impairment, and determined how cognitive impairment influenced power wheelchair use. A total of 30 power wheelchair users completed power wheelchair, cognitive and perceptual assessments. There were statistically significant differences in all power wheelchair assessments depending on the severity of the subject’s cognitive impairment. Cognitive functioning and visual perception were important for power wheelchair performance. Cognitive functioning also influenced power wheelchair confidence, while the built and social environments played significant roles in power wheelchair use. In clinical practice, Montreal Cognitive Assessment scores may provide information to complement power wheelchair assessments, but when used alone may miss some important information. The Power mobility Indoor Driving Assessment, Wheelchair Skills Test Questionnaire, and Life-Space Assessment represent complementary power wheelchair assessments to understand power wheelchair use in adults.
Mobility is a fundamental and basic human right (1) that is essential to health and quality of life (2). For individuals experiencing severe mobility limitations, power wheelchairs (PWC) often become a primary
means of mobility. By enabling independent mobility, PWC may facilitate participation in meaningful activities (3), improve social life (4), and reduce caregiver burden (5). Given the increasing age of the population, and the increased use of PWC by older adults (6), the prevalence of PWC users is expected to continue to grow.
There is a great deal of individual variability among the factors influencing PWC use, including diverse components, such as individual characteristics (e.g. motor, cognitive and perceptual abilities) (7–10), the environment (e.g. social and physical), the nature of the tasks required to be achieved (e.g. daily activities) (9, 10), and self-efficacy (11). Moreover, PWC use includes aspects of “capacity” (i.e. what a person can do in a standard environment) and “performance” (i.e. what a person actually does in their everyday environment) (12). Given the complexities of PWC use, PWC provision is a complex process requiring patient-centred approaches that include the individual, clinicians, and caregivers (9, 13).
In clinical settings, healthcare professionals reported cognitive functioning as the primary concern when providing a PWC to individuals with cognitive impairment (13). Indeed, cognitive factors, such as being distracted, were reported as an intrinsic factor related to the cause of accident (14). Evidence also suggests that accidents among PWC users increased if the user had executive dysfunction (15). Cognition and visual perception impairments have also been linked to problems with PWC driving capacity (7, 8). However, understanding relationships between cognitive functioning and PWC use are at an early stage of development, and the role of cognitive functioning in PWC use remains unclear.
Psychological factors may also explain PWC use. For example, self-efficacy, defined as belief in one’s capabilities to accomplish a specific task (16), has been correlated with participation in activities of daily living (17). However, to our knowledge, the relationships between PWC confidence and PWC use have not been investigated. Self-efficacy, commonly used interchangeably with the term confidence, is referred to as confidence throughout this paper (11).
Research into the correlations between cognitive functioning, PWC confidence and PWC use is fundamental to ensuring best practice in PWC provision. Such research may help PWC providers (i.e. occupational therapists and physicians) in selecting appropriate assessments, anticipating difficulties with PWC use in daily life, customizing training approaches, and decision-making. Thus, individuals with dual motor and cognitive disabilities may receive greater access to PWC use through enhanced training and increased opportunities for autonomy, occupational engagement, and social participation.
The objectives of this study were: (i) to explore differences in PWC performance, PWC confidence and life-space mobility between levels of cognitive impairment (no, mild, moderate, severe cognitive impairment); (ii) to explore the relationships between cognitive functioning and PWC performance, PWC confidence and life-space mobility; and (iii) to explore how cognitive scores influence PWC performance, PWC confidence and life-space mobility.
Design and setting
A cross-sectional exploratory study was conducted in one rehabilitation centre and one long-term care facility in France and Canada. Recruitment was carried out between October 2019 and February 2020, and November and December 2020. Due to COVID-19 restrictions, recruitment was halted in March 2020. Public health recommendations were followed to complete data collection in each country. Recruitment was only able to continue in November 2020 in France, resulting in an imbalance between Canadian and French participants. The Strengthening Reporting of Observational Studies in Epidemiology (STROBE) for cross-sectional studies was followed. Ethical approval was received from the local institutional review boards and ethics committees at each site, Quebec City (Canada) (MP-13-2020-1841CA) and Ploemeur (France) (2019-A02554-53).
Subjects
PWC users 18 years of age and older, who independently used a PWC for 3 months or longer were included in the study. Individuals were excluded if they could not communicate in English or French, if they were not able to attend 2, 2-h evaluations, or if they had significant behavioural disorders that could impact their ability to consent or to complete the evaluations. The sample was recruited through rehabilitation facilities and wheelchair seating programmes in France and in Canada, with the help of healthcare professionals at each (i.e. occupational therapists and physicians). All participants provided informed consent.
Procedure
Two data collection sessions (approximately 2 h each, 1 week maximum between each session) were performed by an occupational therapist with 6 years’ experience. Data collection was completed at a convenient location chosen by the participants (e.g. home, rehabilitation centre, long-term care facility). During the first session, participants completed a sociodemographic form (i.e. age, sex, marital status, education, civil status) and were asked details about characteristics related to PWC use (i.e. previous experience, hours using the PWC per day, personal or borrowed PWC, joystick or switch access, history of previous accidents). Participants completed the Montreal Cognitive Assessment (MoCA), the Motor-Free Visual Perception Test 3rd edition (MVPT-3), and the Wheelchair Skills Test Questionnaire (WST-Q) version 5.0 (described below). During the second session, participants completed the Life-Space Assessment (LSA), the Dysexecutive Questionnaire (DEX), and the Power mobility Indoor Driving Assessment (PIDA) (described below).
Evaluation tools
Cognitive assessments. Three cognitive assessments were chosen based on their common use in clinical settings by occupational therapists, (i.e. clinicians most involved in PWC provision) and for their frequent citations in the literature related to cognition and driving (18).
Global cognitive level was assessed using the MoCA (version 7.1), a screening tool for cognitive impairment (19). This 30-point assessment covers a spectrum of cognitive functioning including visuospatial and executive function, memory, attention, language, abstraction and orientation. High sensitivity, specificity, reliability and validity have been established in diverse populations (19). A score ≥ 26 indicates no cognitive impairment; 18–25 indicates mild cognitive impairment; 10–17 indicates moderate cognitive impairment; and < 10 indicates severe cognitive impairment (20). The evaluator obtained MoCA certification (MoCA ID CAEPELAL198222-1; November 2019).
Visual perceptual abilities were assessed using the MVPT-3, which comprises 65 perceptual tasks, such as visual discrimination and visual memory. A standard score is available according to the individual’s age, with scores ranging from 55 to 145. Higher scores represent higher visual perceptual ability (21). Construct, convergent, and discriminant validity and reliability have been reported (22).
Everyday manifestations of executive dysfunction were assessed using the self-administered DEX, a 20-item scale assess-ing difficulties with behavioural control, emotion regulation, awareness attention, memory and information processing (23). Items are rated on a 5-point Likert scale (0–4), with each point representing a greater level of severity. Sensitivity has been reported to measure executive dysfunction after brain injury (24).
PWC use assessments: Three PWC use assessments were chosen based on their common use in clinical settings by occupational therapists and for their frequent citations in the literature related to PWC use.
Objective PWC performance was assessed using the PIDA, which includes 30 tasks, such as “entering, spacing and exiting the elevator” and “parking beside a table”. Tasks are scored from 1 (unable) to 4 (optimal performance) (25). A total percentage score based on the total number of skills performed is calculated. Moderately good intra-rater reliability, very good inter-rater reliability, and content validity have been documented (25).
Perceived PWC capacity, confidence and performance were evaluated using the WST-Q version 5.1 for PWC (26). The WST-Q assesses individuals’ perceived capacity, confidence and performance to perform 25 skills using a PWC. Three total scores, from 0–100%, are calculated for each component of the test: capacity, confidence and performance (26). Reliability and validity have been documented (27).
Life-space mobility was measured using the LSA, a 20-item questionnaire assessing mobility in 5 areas: outside the bedroom, outside the home, in the neighbourhood, in the town, and outside the town (28). Items are scored on a scale from 0 to 6, providing a composite score ranging from 0 to 120. Measurement properties of the LSA for wheelchair users have been documented (29).
Data analysis
Descriptive statistics (mean, standard deviation (SD), frequency, proportions) were summarized for sociodemographic information, PWC characteristics and all evaluation outcomes. Multivariate analysis of variance (MANOVA) and post hoc test (Bonferroni) were used to explore differences in PWC performance (PIDA), PWC confidence (WST-Q-confidence) and life-space mobility scores (LSA) depending on level of cognitive impairment (Objective 1). MoCA scores were used to differentiate groups according to their severity of cognitive impairment (no, mild, moderate, severe cognitive impairment). Pearson’s correlation coefficients were calculated to explore relationships between cognitive (MoCa and DEX), perceptual (MVPT-3), PWC performance (PIDA), PWC confidence (WST-Q confidence subscale) and life-space mobility (LSA) scores (Objective 2). Correlations were defined as: strong (r = 0.8), moderate (r = 0.6–0.7) and fair (r < 0.5). Only variables with statistically significant correlations were included in further analyses. To determine the influence of cognition of PWC use, a principal component analysis with varimax rotation was performed with all evaluation tools (MoCA, MVPT-3, WST-Q-confidence, PIDA and LSA) (Objective 3). Scatterpoints were examined for outliers, and all variables with statistically significant correlations were included in the principal component analysis. Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy were used to determine the suitability of the variables for structure detection, with p < 0.05 and a score of greater than 0.6 considered statistically significant, respectively. Principal component analysis was expected to identify 3 principal components. SPSS statistical software version 26 was used for analyses with an alpha level of ≥ 0.05.
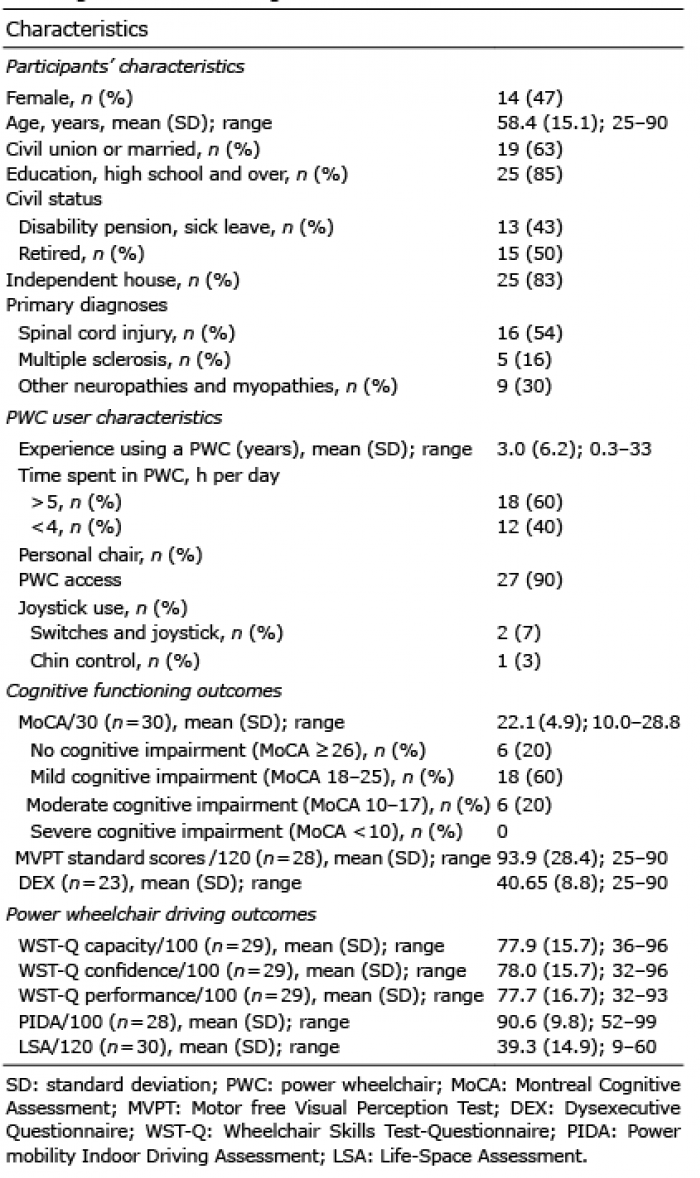
A total of 30 participants (Canada n = 3; France n = 27) were included in the study. The participants mean (SD) age was 58 (15) years, 47% were female (n = 14), and the majority lived in the community (83%, n = 25). One participant did not complete the second part of data collection because of hospitalization unrelated to the study. Participants had a variety of diagnoses (n = 16 spinal cord injury; n = 5 multiple sclerosis; n = 9 various neuropathies or myopathies), 3.0 (SD = 6.2) years of experience using a PWC, and 6 reported at least one accident since receiving their PWC. Twenty-four participants had a MoCA score of 25 or less. Sociodemographic, PWC use characteristics, cognition and PWC users’ scores are summarized in Table I.
Table I. Participants’ sociodemographics, PWC user characteristics and cognitive functionning outcomes
There were statistically significant differences in PWC use scores (PWC performance (PIDA), PWC confidence (WST-Q-confidence) and life-space mobility (LSA)) depending on severity of cognitive impairment (MoCA), as described in Table II. Post hoc analyses indicated a statistically significant difference in PWC performance (PIDA), PWC confidence (WST-Q--confidence) and life-space mobility (LSA) scores be-tween the groups “no cognitive impairment”’ and “moderate cognitive impairments” (p = <0.001; p = 0.002, p = 0.022, respectively); and between “mild cognitive impairment” and “moderate cognitive impairments” (p = 0.001; p = <0.001, p = 0.011, respectively). There were no differences in PWC performance (PIDA), PWC confidence (WST-Q-confidence) and life-space mobility (LSA) scores between those with “no cognitive impairment” and those with “mild cognitive impairment”.
Table II. Power wheelchair (PWC) use scores depending on severity of cognitive impairment
As described in Table III, MoCA scores correlated moderately with PIDA scores and WST-Q (capacity, confidence and performance) and had a small correlation with LSA scores. MVPT-3 standard scores correlated moderately with PIDA scores, and slightly with LSA scores and WST-Q (capacity, confidence and performance) scores. There were no statistically significant correlations between the DEX and PWC driving scores or between DEX and cognitive scores, DEX scores were collected only with 23 participants. PWC use scores (PWC performance (PIDA), PWC confidence (WST-Q-confidence) and life-space mobility (LSA)) had statistically significant correlations between variables.
Table III. Correlation between cognitive and power wheelchair (PWC) use assessments (n = 30)
The factorability of the correlation matrix was ver-ified using Bartlett’s test (χ2[15] = 66.62, p < 0.001) and KMO statistic (KMO = 0.85). All variables had a Measure of Sampling Adequacy (MSA) > 0.7. Two statistical outliers were examined, but did not change the principal components identified. The first principal component (eigenvalue = 3.474, 69% of the total variance) had large statistically significant associations with the PIDA, MoCA, and the MVPT-3 standard score, suggesting that component 1 predominantly measured objective PWC performance, cognitive level and visual perception abilities. The second principal component (eigenvalue = 0.516, 10%) had large statistically significant associations predominantly with WST-Q-confidence and the MoCA, suggesting that factor 2 is based largely on perceived PWC use confidence and cognitive level. Factor 3 (eigenvalue = 0.460, 9%) included the LSA alone, suggesting that factor 3 may represent the built and social environments influencing PWC use. Principal component loadings are shown in Table IV.
Table IV. Principal component loadings from full sample (n=30)
To our knowledge this is the first study to support explicit relationships between cognitive functioning, PWC confidence, PWC performance and life-space mobility among adults with experience using a PWC. Results indicated that individuals with moderate cognitive impairments could safely drive a PWC in optimal environments. Moreover, results showed that cognitive levels (according to the MoCA) explained some of the variability in PWC performance and in PWC confidence, but did not explain variability in life-space mobility.
The current study found a statistically significant difference in PWC use scores (PWC performance, PWC confidence and life-space mobility scores) between “moderate cognitive impairment” group and both “mild cognitive impairment” and “no cognitive impairment” groups. Interestingly, the groups with mild and no cognitive impairment demonstrated no differences in PWC use scores. One hypothesis is that PWC users with moderate cognitive impairment use their PWC differently from people with mild cognitive impairment or without cognitive impairment. Remarkably, participants in the present study who reported previous accidents using their PWC had higher cognitive levels. An explanation could be that users with higher cognitive level are more likely to try new experiences and to take risks, highlighting the impression that individuals with higher cognition may be given more freedom to assume risk. Moreover, users with cognitive impairment may not have the same opportunities to try new experiences or to assume risk, as they are more likely to use a PWC in safe and controlled environments or be assisted by others. While the right to assume risk remains a controversial issue, further research understanding how PWC users with diverse cognitive impairment use a PWC in daily life is required. Previous research related to driving a car after a traumatic brain injury may provide some insight into the next steps for PWC use (30).
Principal component analysis, used as an exploratory approach to identifying relationships (31), suggested 3 components to explain the variability of PWC use that included factors related to cognition, vision, PWC performance, PWC confidence, and the environment. It is noteworthy that the KMO was 0.85, suggesting excellent coherence between variables. The results of the current study are supported by previous research exploring influential factors of PWC use. According to Routhier and colleagues, PWC mobility is influenced by interactions between the user, the environment, daily activities, training and wheelchair specifications (9). Smith and colleagues reported similar influential factors (i.e. individual, environment, wheelchair and task) and added that optimal PWC use requires knowledge of each factor (10). Findings from the current study suggest the importance of specifically considering concepts of cognitive functioning as well as confidence. However, it should be noted that not all factors related to the individual that could have influenced PWC use (e.g. life habits, age, residency) were explored in this study, and these should be consider in future research.
The first principal component suggested that cognitive functioning (MoCA), perceptual abilities (MVPT-3) and PWC performance (PIDA) accounted for 69% of the total variance. Similarly, processes of PWC use have been shown to require a wide range of skills, abilities and knowledge, and 50% of these skills were related to cognitive domains (10). The MoCA comprises diverse cognitive domains (visuospatial/executive, denomination, memory, attention, language, abstraction and orientation) (19) that have been reported as essential for PWC use (7, 8, 32). However, decisions around PWC provision for an individual with cognitive impairment are commonly based on clinician-perceived safety and readiness (13). To fully understand functional cognitive abilities and risk, one solution to enhance safety while promoting training may be to combine appropriate cognitive screening assessments (such as the MoCA) and real-world practical situations for extended periods of time. Such combinations of validated assessments and clinical judgment over longer trial periods have been useful for determining ability to drive a car after a traumatic brain injury (33). Accordingly, the MoCA has been validated to identify driver risk in the context of car driving (34). However, establishing cognitive cut-points to guide clinical decision-making for PWC provision remains questionable, as it may restrict individuals with cognitive impairment from trialling PWC use (35). There is a great deal of work to be done to establish evidence-based intervention for PWC use for individuals with cognitive impairment and to strike a balance between human rights (mobility) and safety (of the individual and others).
The second principal component regrouped cognitive level (MoCA) and PWC confidence (WST-Q confidence). This is not surprising, as confidence involves many cognitive processes (e.g. judgement, knowledge) (36), as well as the interaction of many complex psychological factors (e.g. outcome expectations, motivation). Furthermore, improved capacity and performance would increase accuracy of perceived PWC use through improvement in metacognitive abilities (skills to perceive self-performance and limitations) (37). Interestingly, confidence has also been identified as a possible factor explaining the gap between PWC capacities and PWC performance (38). Specific to the context of PWC driving, improved confidence to use a PWC should improve PWC capacities (what the PWC user can do), while successful experiences using the PWC should improve PWC performance (what the PWC user does in daily life). In fact, confidence has been shown to be influential on manual wheelchair skills training and wheelchair provision (39). Thus, innovative PWC training approaches that aim to enhance PWC confidence should be considered in future research.
In the third principal component, life-space mobility (LSA) was the only variable that explained variance in PWC use. Given that life-space mobility is a concept used to assess patterns of functional mobility over time, the third principal component was described as the built and social environment. In line with the current results, it is largely accepted that the environment can facilitate or hinder PWC use (9, 10).
Finally, through principal component analysis, aspects of PWC performance (PIDA), PWC confidence (WST-Q confidence) and life-space mobility (LSA) were attributed to 3 different components, suggesting that the PIDA, the WST-Q confidence subscale and the LSA captured 3 different aspects of PWC use. This is in line with the intended constructs to be assessed by each tool. In clinical practice, evaluations combining the PIDA, WST-Q confidence and LSA may provide a representative overview of an individual’s ability to use a PWC. Each tool could also be used separately to focus on 1 aspect of PWC use, as deemed important for the individual. For example, the PIDA could be used to objectively assess indoor PWC performance, either inside the home or institutions (25). Given the importance of individuals’ perceived PWC confidence, the WST-Q confidence subscale could be used to determine in which skills the PWC user lacks confidence to better target training. Furthermore, the construct of PWC use confidence may be explored beyond skills-specific confidence using Wheelchair Use Confidence Scale (WheelCon-P) (40). The WheelCon-P evaluates confidence in 6 conceptual areas, including negotiating the physical environment, PWC activi-ties, knowledge and problem-solving, advocacy, managing social situations and managing emotions (40). However, the WheelCon-P has not yet been validated in populations with cognitive impairment. Given the potential influence of PWC confidence on PWC use, further research is warranted among individuals with cognitive impairments.
Study limitations
Although a small sample size of 30 participants was used to explore factors influential in PWC use, the
results provide the first statistical evidence explaining the important role of cognition in experienced PWC users. Due to COVID-19 restrictions, recruitment was halted in March 2020 and only 3 participants were recruited in Canada. Therefore, the sample size is less generalizable than anticipated, and is representative mainly of PWC drivers in France. Generalizability is also limited to experienced PWC users; as novice users or those who have not yet tried a PWC were not included in the current study. Future studies should include individuals who were precluded from PWC provision and novice users to fully explore cognition, PWC confidence and safety concerns. This study took place in Canadian and French institutions; thus, the heterogeneity strengthens the generalizability of our findings.
The assessments were selected because they evaluate different aspects of cognitive functioning and because they evaluate PWC use in a variety of ways (objective and subjective evaluation, and in various environments). Acknowledging that neuropsychologist tests may provide deeper understanding of cognitive functioning related to PWC use, we chose tools that would be practical for use by clinicians (e.g. occupational therapists), who are commonly responsible for wheelchair assessment. Other assessments tools, such as the Trail Making Test, may also help to explain the relationship between cognition and PWC use. Moreover, the number of assessments was limited to reduce burden of data collection for participants. Despite the study limitations, these results may guide clinical practices in the selection of assessment for individuals with dual motor and cognitive disabilities who may benefit from a PWC.
In conclusion, there are correlations between cognitive functioning and PWC use among experienced PWC users. Statistically significant differences were found in PWC use scores according to participants’ severity of cognitive impairment. While the results of this study may guide the selection of cognitive and PWC assessments for PWC provision, further research should continue to model the influence of cognitive functioning, PWC confidence and environmental aspects influencing PWC use.
The authors acknowledge Ms Marie-Caroline Delebecque (Centre Mutualiste de Réadaptation de Kerpape, Pleomeur, France) and Ms Anne-Sophie Allaire (Centre interdisciplinaire de recherche en réadaptation et intégration sociale, Québec City, Canada), who provided organizational support for ethics and data collection procedures.
Funding.This work was supported by the Réseau Provincial de Recherche en Adaptation-Réadaptation (REPAR) du Fonds de recherche du Québec – Santé (FRQS), the Quebec Research Network on Aging (RQRV), and the Social Sciences and Humanities Research Council (SSHRC). Alice Pellichero received PhD scholarships from the REPAR, the National Centre of Excellence in Aging Research AGEWELL, the Centre for interdisciplinary research and readaptation and social integration (Cirris) and Participation Sociale et Villes inclusives (PSVI). Krista Best and François Routhier are FRQS Research Scholars (Junior 1 and Senior respectively).
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize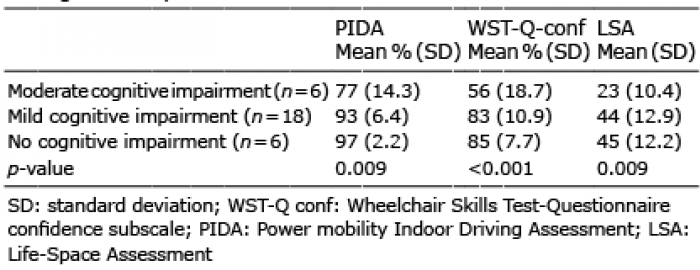 Click to show fullsize
Click to show fullsize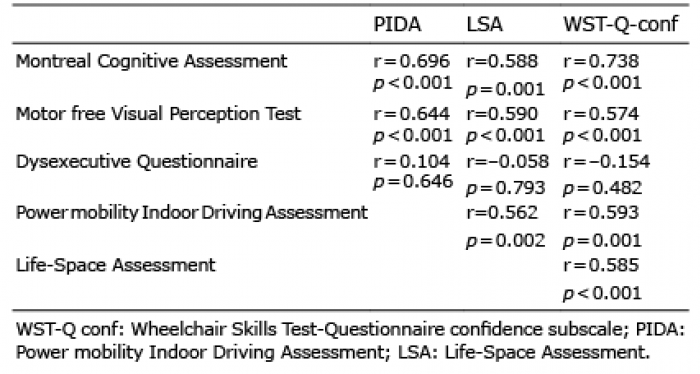 Click to show fullsize
Click to show fullsize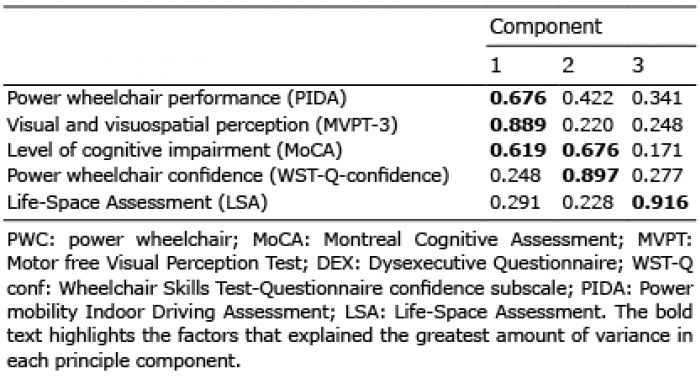 Click to show fullsize
Click to show fullsize