
From the 1Department of Physical Therapy, Ibaraki Prefectural University of Health Science, 2Department of Rehabilitation, Public Nanokaichi Hospital, 3Department of Rehabilitation Center, Hidaka Rehabilitation Hospital, 4Department of Physical Therapy, Ota College of Medical Technology, 5Department of Rehabilitation Center, Hidaka Hospital, 6Department of Rehabilitation Sciences, Gunma University Graduate School of Health Sciences and 7Department of Physical Therapy, Faculty of Health Care, Takasaki University of Health and Welfare, Takasaki, Japan
Objective: To determine which sections of the Balance Evaluation Systems Test (BESTest) distinguish levels of post-stroke functional walking status and to establish their cut-off scores.
Design: A retrospective cross-sectional study.
Subjects and methods: The BESTest was administered to 87 stroke patients who were able to walk without physical assistance upon discharge from the hospital. Subjects were divided into 3 functional walking status groups: namely, household ambulators, limited community ambulators, and unlimited community ambulators. The receiver operating characteristic curve was determined and the cut-off score and area under the receiver operating characteristic curve (AUROC) of each section calculated.
Results: In the comparison of household and limited community ambulators, the accuracies of all BESTest sections were moderate (AUROC>0.7), and the cut-off scores were 36.1–78.6%. In the comparison of limited and unlimited community ambulators, one section (stability in gait) had high accuracy (AUROC=0.908, cut-off scores=73.8%) and 3 sections (biomechanical constraints, anticipatory postural adjustments, and postural response) had moderate accuracy (AUROC=0.812–0.834, cut-off scores=75.0–83.4%).
Conclusion: This study demonstrated that different sections of the BESTest had different abilities to discriminate levels of post-stroke functional walking status, and identified cut-off values for targeted improvement.
Key words: stroke; walking speed; postural balance; BESTest.
Accepted Aug 27, 2021; Epub ahead of print Sep 6, 2021
J Rehabil Med 2021; 53: jrm00230
Correspondence address: Kazuhiro Miyata, Department of Physical Therapy, Ibaraki Prefectural University of Health Science, 4669-2, Ami-Machi, Inashiki-gun, Ibaraki, 300-0394 Japan. E-mail: miyatak@ipu.ac.jp.
Doi: 10.2340/16501977-2870
The Balance Evaluation Systems Test (BESTest), a clinical postural control measure, categorizes postural control systems in 6 different sections. This study investigated which sections of the BESTest distinguish levels of post-stroke functional walking status, which, in turn, is based on walking speed. Among the slower walkers, all sections of the BESTest showed moderate relationships to categories of walking status. Among the faster walkers, 4 sections showed moderate to strong relationships and 2 sections showed weak relationships. This study may have clinical implications for rehabilitation aimed at improving functional walking status in individuals with stroke. These findings will help rehabilitation professionals assess postural control in relation to stroke patients’ ability to walk in different settings (e.g. their household or the community) and determine which postural control systems should be prioritized in therapeutic interventions.
Decline in mobility is one of the major sequelae after a stroke (1). Approximately 30–40% of patients with stroke can engage in only limited community walking (2). Walking speed has been shown to be a valid and reliable measure of functional walking status across the continuum of recovery after stroke (3), which, in turn, is important for enabling the patient to safely perform activities of daily living (ADL). In previous studies, researchers have categorized post-stroke individuals as household ambulators, limited community ambulators, and unlimited community ambulators, based on cut-off scores for comfortable walking speed (4, 5). Recovery of walking speed after stroke is tantamount to recovery of walking ability and is critical to maintaining quality of life.
In patients with stroke, walking speed is related to various functions; however, one of its key determinants is postural control. Postural control is a complex ability that involves several sub-systems (6), an observation reinforced by biomechanical studies (7–9). However, a systematic review of the literature did not provide sufficient evidence that postural control training per se improved walking speed in individuals with stroke (10). Postural control training is complex and not specific to individual postural control systems. For efficient assessment and intervention by a physiotherapist, it is recommended that postural control systems more directly related to walking speed, and hence walking function, be identified.
The Balance Evaluation Systems Test (BESTest) is a clinical assessment tool that evaluates the examinee’s performance across 6 postural control systems (sections) (11). Therefore, the BESTest assessment results can be used to select interventions that focus on the specific deficits identified in each patient. Reports about the sections of the BESTest are increasing; for instance, each section of the BESTest is reported to have low to moderate accuracy as a fall prediction tool, and the relationships of scores with falls vary among the BESTest sections (12, 13). Effective rehabilitation of postural control to improve walking ability and prevent falls requires a better understanding of the relationship of walking to postural control.
Although previous research has demonstrated that specific sections of the BESTest are able to differentiate between slow and fast walking speeds in older adults with hip fractures (14), studies have not yet examined which section(s) of the BESTest can best identify functional walking status in individuals with stroke. A better understanding of the relationship between functional walking status and the sections of the BESTest can guide the selection of interventions that address problems in specific aspects of postural control to improve the walking ability of individuals with stroke. We thus conducted the present cross-sectional study, first, to determine which of the sections of the BESTest can distinguish levels of functional walking status using the 3 walking status groups recently updated by Fulk et al. (5), and secondly, to establish cut-off scores for these sections in post-stroke individuals.
Design
A multi-centre retrospective cross-sectional study was conducted, and information was collected from medical records. No written or oral consent was obtained from subjects because this was a retrospective observational study and only the existing data were used. Opt-out options for study information were posted on the hospital bulletin board to provide the opportunity for patients to refuse participation. Ethical approval was obtained from the Gunma University Ethical Review Board for Medical Research Involving Human Subjects (#15–73) and the Ethics Committees of Public Nanokaichi Hospital (#20160208), Hidaka Rehabilitation Hospital (#151101), and Hidaka Hospital (#112). All research and reporting of findings were undertaken in compliance with the Declaration of Helsinki of 1975, as revised in 2013 (15).
Participants
The study included individuals with stroke who participated in a rehabilitation programme in 3 convalescent rehabilitation wards between May 2010 and January 2017. For the patient to be included, all the following criteria had to be met: supratentorial stroke, diagnosis of cerebral infarction or cerebral haemorrhage, first unilateral hemispheric stroke, and ability to walk without physical assistance from another person (functional ambulation category (FAC) ≥ 3) (16). Any of the following criteria disqualified the patient from the study: cognitive impairment (Hasegawa Dementia Scale-Revised (HDS-R) < 21/30) (17), other musculoskeletal or neurological disorders, missing BESTest score on discharge, or the patient’s request not to be included in the study.
In Japan, hospitals with a convalescent rehabilitation ward are considered standard post-acute rehabilitation facilities (18). All the present study’s participants underwent a conventional stroke rehabilitation programme prescribed by a physician and conducted by staff physiotherapists, occupational therapists, and speech therapists, as required. The therapies were customized and involved muscle strength, postural control, gait, arm activities, activities of daily living, and cognitive and speech training. Therapy was carried out 7 days/week for 2–3 h per day on weekdays and 1–2 h on weekends and national holidays, on an inpatient basis.
Data collection
The data outlined below were collected from the participants’ medical records and the rehabilitation centre’s database. To help understand each participant’s attributes and stroke-related characteristics, data were collected regarding age, sex, time since stroke onset, type of stroke (ischaemic or haemorrhagic), and affected side. Regarding the lower-extremity motor function, the Brunnstrom recovery stage for lower extremities (BRS lower-extremity) was used (19). The BRS lower-extremity recovery stage classification has demonstrated good reliability for the assessment of motor recovery of the lower extremities after stroke, ranging from stage 1 (flaccidity) to stage 6 (isolated joint movement) (20).
Two core assessments, evaluated by physiotherapists responsible for the participant’s intervention at discharge, were also collected. These physiotherapists had received specific training in comfortable walking speed and the BESTest assessment. Comfortable walking speed is a reliable and validated measure of walking ability after stroke (21). Participants were instructed to walk at their self-selected comfortable speed for a set distance of 6 m (i.e. “Walk at your normal speed from here past the next mark and stop”). The time taken to walk the 6 m was measured using a digital stopwatch and used to calculate the participant’s gait speed and hence, their functional walking status category (i.e. household ambulators, limited community ambulators, and unlimited community ambulators).
The validity and reliability of the BESTest has been confirmed in individuals with stroke (22). The BESTest consists of 27 items, with some items consisting of 2–4 sub-items (e.g. for the left and right sides), for a total of 36 tasks. Each item is scored from 0 (worst performance) to 3 (best performance) points, based on time or performance criteria, resulting in a total possible score of 108 points, which is converted to a percentage score. Each participant’s total score and the score for each section were obtained. The BESTest items are categorized into the following 6 sections: biomechanical constraints, stability limits and verticality, anticipatory postural adjustments, postural response, sensory orientation, and stability in gait.
The “biomechanical constraints” section for standing postural control evaluates the quality of the base of foot support, range of motion, functional ankle and hip strength, postural alignment, and ability to rise from the floor to a standing position. The “stability limits and verticality” section evaluates items for an internal representation of how far the body can move over its base of support before changing that base or losing postural control, as well as an internal perception of the postural vertical. The “anticipatory postural adjustments” section evaluates tasks that require active movement of the body’s centre of mass in anticipation of a postural transition from 1 body position to another, such as standing on tiptoes, standing on 1 leg, and alternate stair touching.
The “postural responses” section evaluates both in-place and compensatory stepping in response to external perturbation induced by the examiner’s hands using the unique “push and release” technique. The “sensory orientation” section evaluates any increase in body sway during a stance associated with altered visual or surface somatosensory information for the control of standing postural control. The task consists of the modified Clinical Test of Sensory Integration for Balance and involves standing on a slope with eyes closed. The “stability in gait” section evaluates postural control during gait, including assessments of changing walking speed, head rotations, and stepping over obstacles.
Data analysis
Descriptive statistics were calculated. The percentage score for each section and the total score for the BESTest were calculated for each participant. The participants were divided into 3 groups according to the recently updated comfortable walking speed criteria of Fulk et al. (5): < 0.49 m/s = household ambulators, 0.49–0.92 m/s=limited community ambulators, and > 0.92 m/s = unlimited community ambulators.
One-way analysis of variance (ANOVA) was used to examine whether each section of the BESTest was able to discriminate among the 3 functional walking status groups in individuals with stroke. The F-value of 1-way ANOVA can be used to determine whether the test is statistically significant. It is calculated as follows: F-value = variance of the group means (mean square between)/mean of the within-group variances (mean squared error). This calculation was followed by a post-hoc Tukey test when significant differences were observed, and effect size r was calculated to understand the magnitude of the difference. The effect size was judged based on 0.1 ≤ r as small, 0.3 ≤ r as medium, 0.5 ≤ r as large (23).
Receiver operating characteristic (ROC) curve analysis was performed to elucidate the postural control system that discriminates functional walking status and determine the optimal cut-off score. ROC analysis is frequently used in studies examining related factors (5, 24). The accuracy of each section of the BESTest was assessed using the area under the receiver operating characteristic curve (AUROC), which can be interpreted as the probability of correctly classifying participants into the designated groups. An AUC value > 0.9 was interpreted as showing high accuracy, 0.7–0.9 as moderate accuracy, 0.5–0.7 as low accuracy, and < 0.5 as strictly due to chance (25). The cut-off score, sensitivity, and specificity values from Youden’s index were then calculated. Positive and negative predictive values were calculated for each section of the BESTest. The sample size needed for this study was estimated based on an alpha level of 0.05, a power of 0.80, and an AUROC of 0.739, taken from a previous study showing the discriminant accuracy of the section of the BESTest (12). It was determined that a sample size of 16 participants was required for each group. All statistical analyses were performed using SPSS Statistics 26.0 (IBM Corp., Armonk, NY, USA). P-values < 0.05 were considered significant.
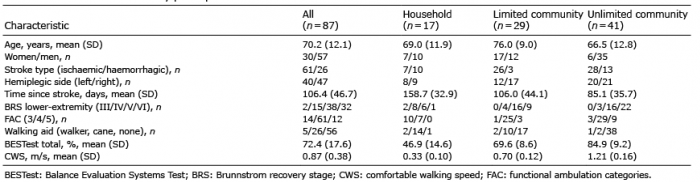
In total, 149 individuals were evaluated by BESTest during the study inclusion period. Of these, 62 were excluded from the study due to infratentorial stroke (n = 12), diagnosis of subarachnoid haemorrhage (n = 7), not their first stroke (n = 9), FAC <3 (n = 13), musculoskeletal diseases (n = 4), and no BESTest results at discharge (n = 17). Thus, the final study population consisted of 87 individuals (35% women) with a mean age of 70.2 years (SD 12.1). Their clinical characteristics are shown in Table I.
Table I. Characteristics of study participants
Results of ANOVA showed significant differences in all sections of the BESTest at the level of walking speed (biomechanical constraints: F(2,84) = 52.7, p < 0.001, stability limits and verticality: F(2,84) = 16.8, p < 0.001, anticipatory postural adjustments: F(2,84) = 50.0, p < 0.001, postural responses: F(2,84) = 28.6, p < 0.001, sensory orientation: F(2,84) = 28.2, p < 0.001, and stability in gait: F(2,84) = 84.2, p < 0.001).
Table II shows the results of the Tukey post-hoc test. Limited community ambulators had a significantly higher score on all sections of the BESTest score compared with strictly household ambulators. The effect size was large except for 2 sections (stability limits and verticality, and sensory orientation). When comparing limited community ambulators with unlimited community ambulators, i.e. the faster walkers, there were significant differences in the biomechanical constraints, anticipatory postural adjustments, postural responses, and stability in gait sections, with unlimited community ambulators demonstrating higher scores on these sections of the BESTest. The effect size was large in 3 sections (anticipatory postural adjustments, postural response, and stability in gait).
Table II. Comparison of section score of the Balance Evaluation Systems Test (BESTest) discriminating the functional walking status
In the comparison of household ambulators and limited community ambulators, i.e. the slower walkers (Fig. 1 and Table III), the accuracies of all BESTest sections were moderate (AUROC = 0.770–0.895). The cut-off score was 36.1–78.6%, which was less than half percentage score, expect for 2 sections (stability limits and verticality, and sensory orientation). The highest sensitivity was obtained for the anticipatory postural adjustments section (100.0%), while the highest specificity was obtained for the stability in gait section (82.4%). Each of the 4 sections had high positive and negative predictive values (> 80.0%).
Fig. 1. Receiver operation characteristic (ROC) curves of the sections of the Balance Evaluation Systems Test (BESTest) for categorizing participants as household or limited community ambulators.
Table III. Optimal cut-off score for discriminating the household (n = 17) vs limited community ambulators (n = 29) in the section of the Balance Evaluation Systems Test (BESTest)
In comparing limited community ambulators with unlimited community ambulators (Fig. 2 and Table IV), the only section with an AUROC of 0.9 or higher was the stability in gait section. The cut-off score determined for these 2 groups was 73.8% (sensitivity = 80.5%, specificity = 89.3%). The accuracies of biomechanical constraints (cut-off score = 83.4%), anticipatory postural adjustments (cut-off score = 75.0%), and postural response (cut-off score = 80.6%) were moderate (AUROC = 0.812–0.834). The accuracies of the stability limits and verticality section and sensory orientation section were low (AUROC < 0.7), and the cut-off scores were also high, at 92.9% and 90.0%, respectively. The highest sensitivity was obtained for the stability in gait section (80.5%), and the highest specificity for the anticipatory postural adjustments section (93.1%). Five sections had high positive predictive value (> 80.0%), and negative positive predictive value of 50.0–76.5% for each section.
Fig. 2. Receiver operation characteristic (ROC) curves of the sections of the Balance Evaluation Systems Test (BESTest) for categorizing participants as limited community or unlimited community ambulators.
Table IV. Optimal cut-off score for discriminating the limited community (n = 29) or unlimited community ambulators (n = 41) in the section of the Balance Evaluation Systems Test (BESTest)
Individuals who have experienced a stroke are known to have postural control dysfunctions and a reduced ability to walk. To our knowledge, this is the first study to examine which postural control systems as defined by the sections of the BESTest are related to speed-based functional walking status. On the relevant sections of the BESTest, the study found significantly different cut-off scores for household ambulators vs limited community ambulators and for limited community ambulators vs unlimited community ambulators. The results of the present study can be used by clinicians to guide their interventions by identifying the postural control systems most closely tied to improving functional walking status.
All sections of the BESTest showed an ability to discern household ambulators from limited community ambulators, with moderate discrimination accuracy. It was clarified that all postural control systems were related to each other to the same degree. The cut-off scores obtained in this study can be thought of as target scores for acquiring the ability to walk to a limited extent in the community from originally only being able to walk in the household. However, all cut-off scores except for stability limits and verticality section were below the cut-off score for predicting falls in individuals with stroke (12, 26). In addition, for anticipatory postural adjustments and sensory orientation sections, the scores were highly discrete, and the potential risk of falling was likely to remain even if the person had the walking status of a limited community ambulator.
In contrast, the accuracy of sections in discriminating between limited community ambulators and unlimited community ambulators differed widely, with 1 section having high accuracy, 3 sections having moderate accuracy, and 2 sections having low accuracy. The cut-off scores were above the fall prediction score in all sections, with stability limits, verticality, and sensory orientation sections above 90.0%. These results suggest that the risk of falling is lower when the walking speed at which a person can walk without restriction in an area is obtained, and that it is necessary to pay attention to specific posture control systems in rehabilitation.
The stability in gait section showed good accuracy in discriminating between groups, with a good combination of sensitivity and specificity, and the positive predictive value was also high. This finding was in line with previous studies that analysed walking speed in relation to BESTest or Brief-BESTest section scores in older adults (14, 27). It is interesting that the stability in gait section is strongly related to walking speed regardless of subject characteristics. However, the relationship between falls and the stability in the gait section differed by disease, with low accuracy for chronic obstructive pulmonary disease patients (AUROC = 0.56) (13) and moderate accuracy for stroke patients and older adults (AUROC = 077–0.81, 0.77, respectively) (12, 26, 28). The stability in gait section evaluates postural control during walking when there is reduced attention to walking, including assessments of changing walking speed, head rotations, stepping over obstacles, and the dual-task timed-up-and-go test. A previous study has shown that individuals with stroke use strategies that prioritize postures over tasks during dual tasks (29). Reductions in postural control while performing dual tasks have been interpreted as indicating interference between competing attentional demands for postural and cognitive tasks (30). We thus speculate that the discrimination accuracy of the stability in gait section including the dual task was high because our 2 walking speed groups (household ambulators and limited community ambulators) prioritized postural control. When assessing the postural control ability of individuals with a stroke, the stability in gait section of the BESTest may be the postural control system that merits the initial focus of rehabilitation, especially when the person has community-level walking status. The cut-off score obtained here is useful for such an evaluation.
Three sections of the BESTest (biomechanical constraints, anticipatory postural adjustments, and postural responses) showed moderate discriminant accuracy for walking status. These results were in line with those of previous studies that examined the relationship between the BESTest section and falls in individuals with stroke (12, 26). These postural control systems have been found to be related to walking speed (7–9, 31–33) and further comprise the essential requirements: elements of locomotion (e.g. walking): progression, postural control, and adaptation. A relationship between each of these 3 essentials of walking and specific sections of the BESTest has been suggested, with progression corresponding to biomechanical constraints; postural control corresponding to stability limits and verticality, anticipatory postural adjustments, postural response, and sensory orientation; and adaptation corresponding to anticipatory postural adjustments, postural response, and stability in gait (14). Also, the cut-off scores obtained between household ambulators or limited community ambulators in these 3 sections were low, from 36.1% to 50.0%. These sections are challenging and may take time to improve, suggesting the need to focus on them early, depending on the likelihood of full recovery.
The remaining 2 sections of the BESTest (stability limits and verticality; sensory orientation) showed moderate accuracy in distinguishing household ambulators from limited community ambulators, but no significant difference in value for limited community ambulators and unlimited community ambulators, and the discrimination accuracy was low. These sections evaluate static postural control in the sitting or standing positions, and the difficulty of the task is low (11, 22). Several studies have shown a relationship between walking speed and these postural control systems (32, 35). Therefore, our finding of a poor discernment ability between limited community ambulators and unlimited community ambulators is very interesting, in that it suggests that these 2 skills may be essential for walking in the community. If an individual experiences a significant decline in the performance on these 2 sections, his or her walking status is likely to decline, and careful evaluation and intervention will be required.
In this study, the patients were mostly men, with approximately half as many women as men. Previously, it has been revealed that there is a sex difference in the effect of ageing on postural control (35, 36). For example, at age 50–75 years, women performed significantly worse on the Functional Reach Test, the Timed-Up-and-Go test, and the Sit-to-Stand Test than men (35). These tasks are also included in the BESTest section, so the results may be affected by sex. Therefore, it is necessary to investigate this issue in a larger population with the same proportion of men and women.
Study limitations
One of the limitations of this study is that the number of patients classified as household ambulators was limited to only 17. Our participants were inpatients with stroke who had received intensive rehabilitation, such that most had surpassed the “household ambulator” walking status. The generalization of the results may therefore be limited. For example, it is unclear whether the section of the BESTest and cut-off scores presented herein are applicable to community-dwelling individuals with stroke, since our participants were inpatients. Accordingly, larger subject groups and the analysis of community-dwelling stroke patients is required for more meaningful results.
In addition, data have been collected from 3 hospitals, and intra-hospital reliability was not evaluated. However, the BESTest is routinely performed at each hospital by well-trained physiotherapists who learned from the videos provided by the developers and participated in in-hospital training on measurement. Finally, the study was retrospective; it used chart review and only univariate analyses, such as ROC curves and comparisons between groups. Confounding factors may have affected the results and generalizability. Additional research is warranted to address these limitations.
It was demonstrated that different sections of the BESTest showed different discriminant accuracy regarding functional walking status in individuals with stroke. In addition, cut-off scores for improvement to the next-higher ambulation level were identified for both household ambulators vs limited community ambulators and limited community ambulators vs unlimited community ambulators: namely, 50.0% and 83.4% for biomechanical constraints, 78.6% and 92.9% for stability limits and verticality, 36.1% and 75.0% for anticipatory postural adjustments, 41.7% and 80.6% for postural responses, 63.4% and 90.0 for sensory orientation, and 50.0% and 73.8% for stability in gait, respectively. These findings will help physiotherapists to assess postural control in relation to walking status in individuals with stroke and to determine which postural control systems should be prioritized in therapeutic interventions.
Funding. This work was supported by JSPS KAKENHI Grant Number JP18K17724.
The authors have no conflicts of interest to declare.


 Click to show fullsize
Click to show fullsize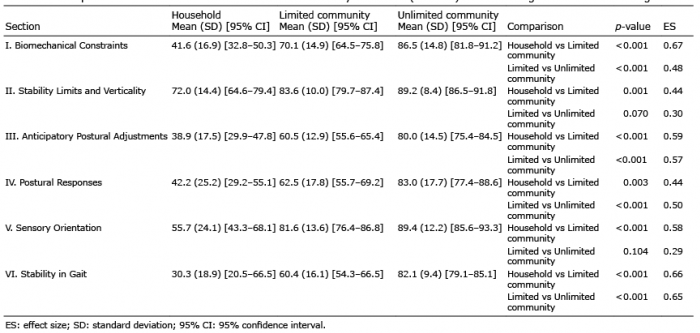 Click to show fullsize
Click to show fullsize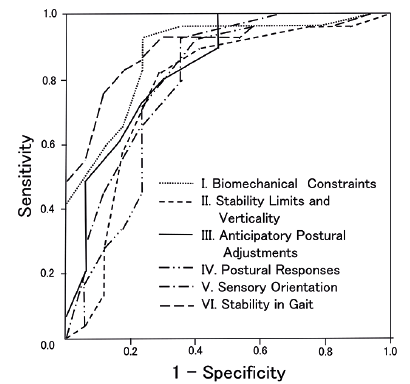 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize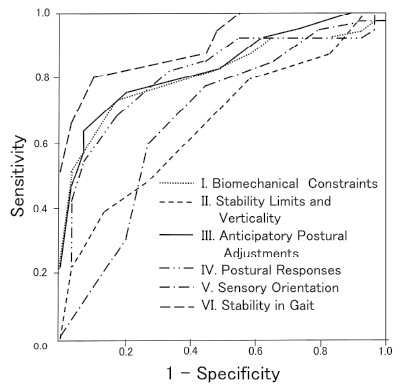 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize